Dr. Mehnaz Memon🖊
Dentowesome 2020
References: Davidson’s Principles and Practice of Medicine Textbook





Dr. Mehnaz Memon🖊
Dentowesome 2020
References: Davidson’s Principles and Practice of Medicine Textbook

(A)
(B)
5. Regular exercise: Jogging & swimming – ⬇️ Arterial pressure
• Objectives
🔅 To reduce the incidence of adverse cardiovascular events viz coronary heart disease, stroke & heart failure
• Benefits:
🔅Diuretics or β blockers have shown to reduce the risk of
🔅Most of the excess Morbidity & Mortality associated with HT is attributable to CAD. Total CVR = CAD risk x 4/3
🔅 Hypertension in old age:
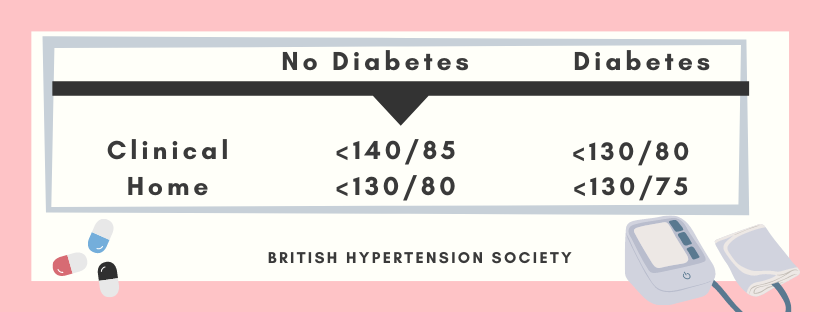
Target BP during AHT



A. ACE Inhibitors:
👉🏻Patients with renal artery stenosis/impaired Renal function (given with utmost care)
⬇️
Reduction of filteration pressure in the glomeruli
⬇️
Renal failure
👉🏻These agents also reduce the progression of Nephropathy in type II diabetes
👉🏻Level of electrolytes & creatinine should be checked before & after 1-2 weeks.
B. ARB’s
👉🏻Have lesser side effects of cough & angioedema than ACE inhibitors
C. Beta-blockers:
👉🏻These drugs are not used now as first line AHT; except in patient with Angina
👉🏻Labetalol & Carvedilol: Have better effect when combined. Labetalol is used as infusion in malignant phase HT.

D. CCB’s
👉🏻The dihydropyridines are effective, well-tolerated particularly in older people
👉🏻Rate–limiting CCB’s: HT with angina. Bradycardia may occur
E. Thiazides & other Diuretics:
👉🏻The loop diuretics have few A/D over thiazides unless there’s renal impairment.

Chart showing Mode of Action & Side effects of AHT’s☝🏻

The influence of comorbidity on the choice of antihypertensive drug therapy

Management of hypertension: British hypertension society guidelines
Criteria:
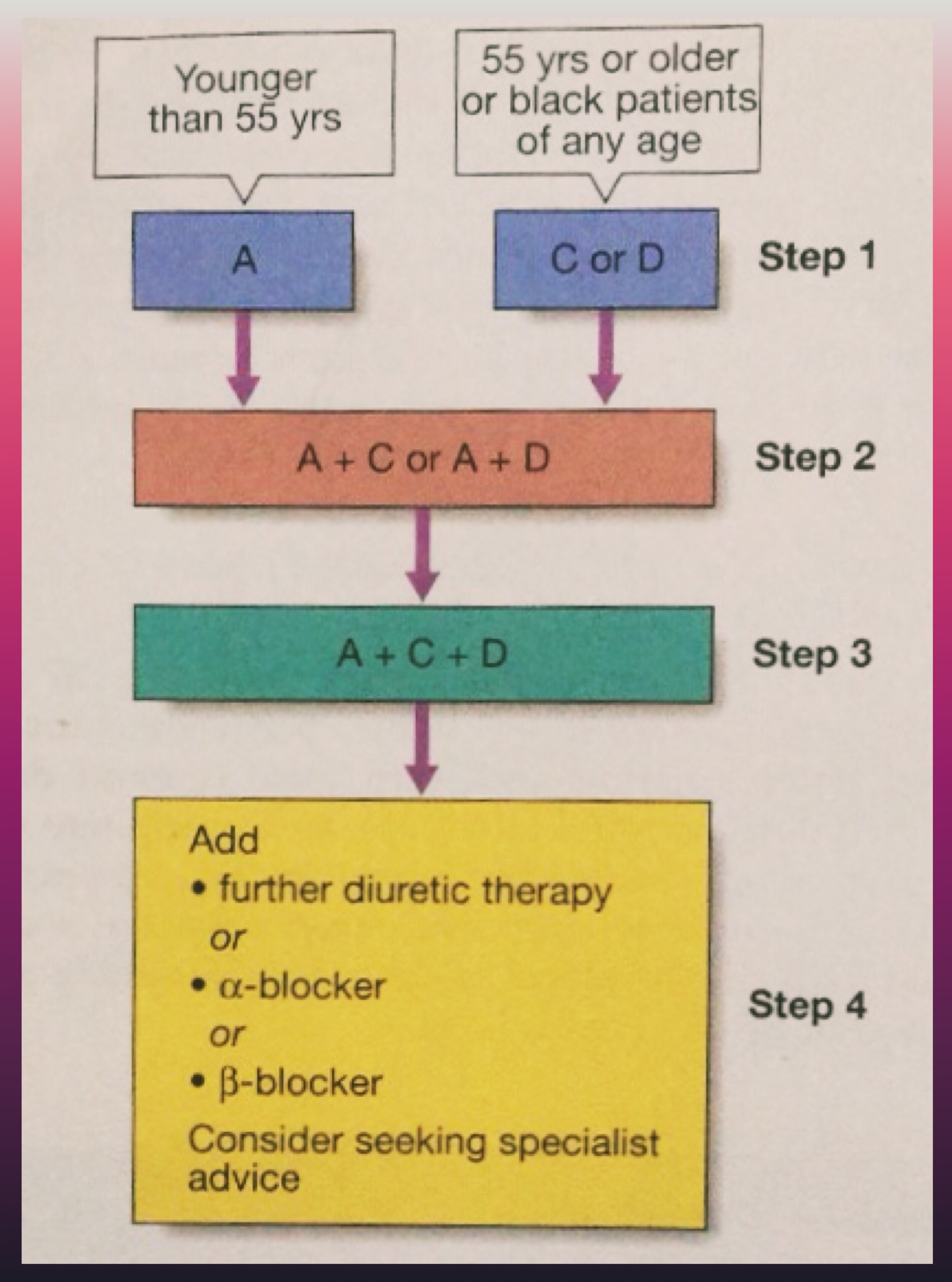
A = ACE inhibitor (consider AT-II receptor antagonist if ACE-intolerant); C = Calcium channel blocker; D = thiazide-type diuretic)
🔅 In accelerated phase HT, lowering BP too quickly may compromise tissue perfusion & can cause –
🔅150/90 mm Hg within 48 hours is ideal along with cardiac failure/hypertensive encephalopathy
🔅Avoid parenteral therapy
🔅Causes of treatment failure include:
📌Aspirin – Antiplatelet
📌Statins – Reduced risk by treating hyperlipidaemia
Dr. Mehnaz Memon🖊
References: Davidson’s Principles and Practice of Medicine Textbook

Hypertension
Definition
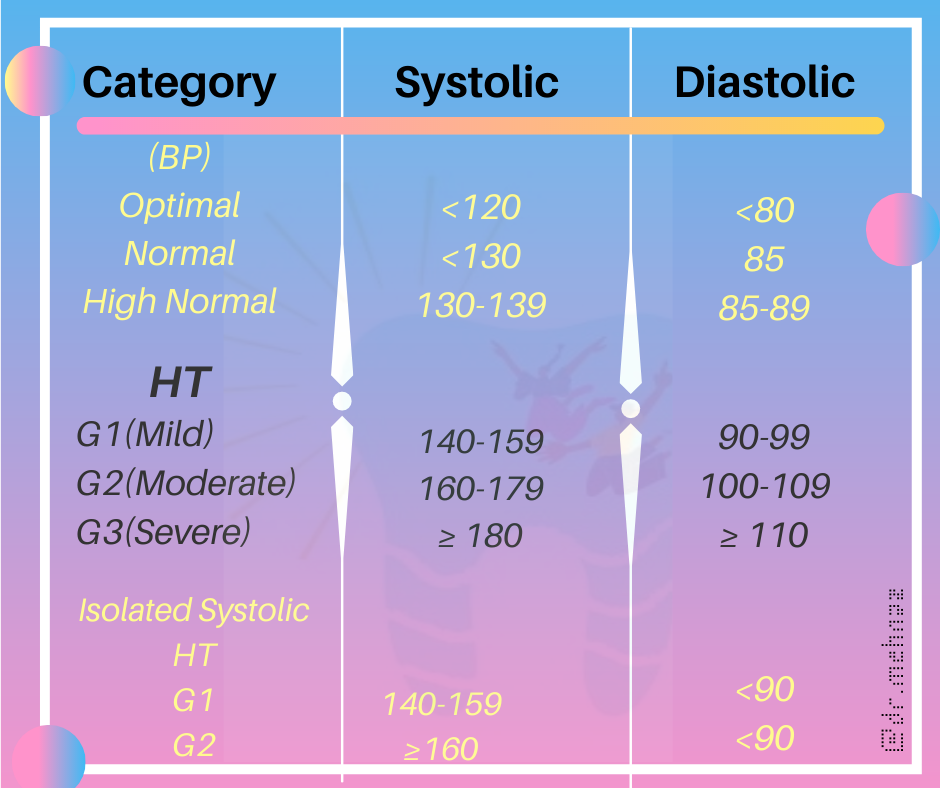
British Hypertension Society
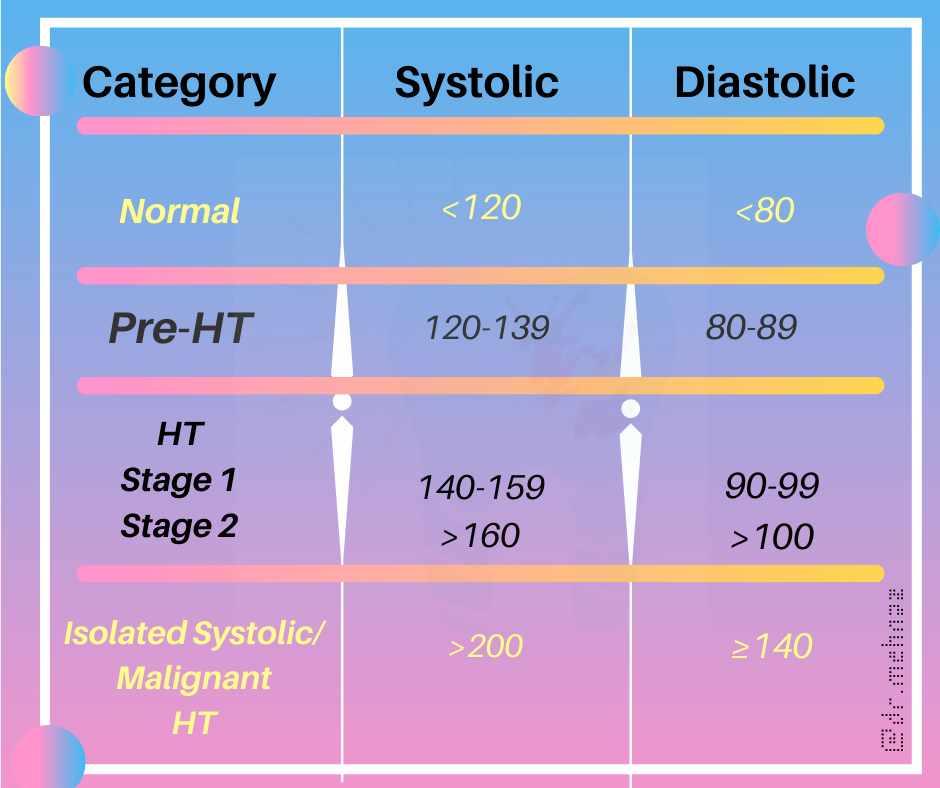
Clinical Classification
References:
Davidson’s Principles and Practice of Medicine Textbook






References:
Davidson’s Principles and Practice of Medicine Textbook
Bisphosphonates are first-line drugs used to treat a wide range of bone disorders, including:
Bisphosphonates are easily identifiable drugs, too. They all contain either of the following two suffixes – –dronate or –dronic acid.

Bisphosphonates act on bone – where they inhibit cells called osteoclasts.
The function of osteoclasts is to break down bone, an essential function for the bone maintenance and repair. However, in diseases such as osteoporosis, osteoclasts can play a pathological role and so, by intervening in how osteoclasts work, it can reduce bone loss and improve bone mass.
Bisphosphonates have a similar structure to naturally occurring pyrophosphate and so are readily absorbed into bone. There, bisphosphonates accumulate in osteoclast cells – triggering cell death. Fewer osteoclast cells lead to reduced bone turnover and an increase in bone mass and reduction in bone loss.
One of the most common side effects of orally administered bisphosphonates is esophagitis – or inflammation of the esophagus. To reduce the risk of esophagitis, patients are counseled to take bisphosphonates in a more cautionary manner compared to other drug classes.
Patients are counselled to take these drugs whilst remaining upright, first thing in the morning and 30 minutes before food/medicines and taken with a full glass of water. Patients should remain upright for 30-minutes post-administration. By taking these steps, the risk of esophagitis or irritation to the esophagus, is substantially reduced.
Other side effects of bisphosphonates include:
Bisphosphonates may also be associated with other side effects not listed in this guide.
Source – PTCB guide to pharmacology
In the NEET MDS Preparation process, the students need to study the previous year exams thoroughly and identify the important topics. This article sheds light on Operative Dentistry & the list of Questions MERITERS experts will answer that are essential for an effective and efficient preparation:
10-13/240 Questions (5%)


Author : V Gopikrishna
INR 1,338 Buy on Amazon

Author : Andre V. Ritter DDS MS
INR 7,595 Buy on Amazon
| Unit | Most Important Topics |
| Cariology | Diagnosis and Treatment planning |
| Operator Positions | |
| Microbiology of Caries | |
| Classification of Caries- GV Black, Root caries, Caries cone | |
| Histo-pathological changes of Enamel and Dentin | |
| Diagnosis of Caries | |
| After Restoration Procedures | |
| Infection control | Occupational Safety and Health ActAerosols and UltrasonicsClassification of Medical, Surgical and Dental InstrumentsSterilization |
| Dental Adhesion | Enamel and dentin bonding systems |
| Direct filling gold | ClassificationManipulationPrinciples of tooth preparation |
| Composites | Composition and classificationCavity preparationPolymerization of composites |
| Amalgam | ClassificationPin retained amalgam restorationsMercury toxicityTrituration |
| Caries and Cavity Preparation | CariologyTooth preparation |
| Sterlization and Isolation | Moist and dry heat sterilization, ETOX gasRubber damMatrices |
| Direct Filling Gold | Types of Direct Filling GoldCavosurface MarginCohesive GoldDegassingCondensation and CompactionProperties of Gold |
| Cast Gold Restorations, Inlays, Onlays | Indications and Contraindications |
| Principles of Tooth Preparations | |
| Finish Lines and Cavosurface Margins | |
| Sprue | |
| Porosities | |
| CAD –CAM | |
| Functional Cusp Bevel | |
| Biomechanical Principles | Cavity Preparation, Smear Layer |
| Rubber Dam in Detail | |
| Separators/ Wedges/ Matrices | |
| Gingival Retraction | |
| Debridement, Polishing Agents | |
| Pulp Protection, Air Abrasion | |
| UltraSonics and Lasers in Cavity Preparation | |
| Walls of Cavity/ Line Angles/ Point Angles | |
| Outline Form, Resistance Form | |
| Retention Form, Bevels | |
| Depth Of Cavity, Ferrules | |
| Instrumentation | Hand Cutting Instruments |
| Instrument Formula | |
| GMT, Angle Former | |
| Hatchets, Angles of Dental Bur | |
| Efficiency of Burs | |
| Carbide/ Diamond/ Stainless Steel Burs | |
| Amalgam Restorations | Indications/ Contraindications of Amalgam Restorations |
| Father of Amalgam | |
| Properties of Amalgam | |
| Creep, Phases of Amalgam | |
| Microleakage, Delayed Expansion | |
| Overhangs, Trituration | |
| Eame’s Technique | |
| Burnishing, Condensation | |
| Mercuric Toxicity | |
| Pin Retained Amalgam Restorations | |
| Types of Pins, Thread Mate System | |
| Bonded Amalgam Restorations | |
| Tooth Colored Restorations | Advantages/Disadvantages |
| Indications/Contraindications | |
| Acid Etching | |
| Skipping Effect | |
| Dentin Conditioner | |
| Primers and Adhesive Resin Generations | |
| Fillers in Composites | |
| C-Factor | |
| Margins and Cavosurface Angles | |
| Shade Determination | |
| BIS-GMA | |
| Compomers | |
| Giomers | |
| Porcelain Restorations | |
| Other topics | Dentin Hypersensitivity |
| Mahler Scale | |
| Box and Tunnel Restorations | |
| Veneers and Laminates | |
| Bonding Agents |
1. Single best answer
2. Image based questions
3. True or false type questions
Please watch the above featured video for more detailed explanation about this article.
We hope this blog will assist you in preparing this subject meticulously for MDS entrance exams.
Prepare judiciously..
SOURCE: MERITERS!!
We have compiled a list of Questions in this article, which MERITERS experts will answer and are very essential for an effective and efficient preparation:


Author : SHILLINGBURG H.T
INR 2,680 Buy on Amazon
Author : Stephen F. Rosenstiel BDS MSD
INR 950 Buy on Amazon
| UNIT NAME | MOST IMPORTANT TOPICS |
| Diagnosis and treatment planning | Diagnostic Casts |
| Indications, Contra Indications | |
| Pontic Designs, Trauma from Occlusion | |
| Mouth Preparation | |
| Cantilever | |
| Retainers and connectors | Components of FPD |
| Indications for Non-Rigid FPD | |
| Partial Veneer Crowns Indications and Contra Indications Porcelain Jacket Crown | |
| Abutments | Ante’s Law |
| Optimum Crown-Root Ratio | |
| Root Surface Area of Each Tooth | |
| Pontics | Types of Pontics and their Important Features |
| Gingival End of Pontic | |
| Pontics Suitable for Anterior Region | |
| Pontics Suitable for Posterior Region | |
| Technical considerations | Forces acting on Abutment Tooth |
| Structural Durability | |
| Retention, Taper | |
| Freedom of Displacement | |
| Reduction, Types of Crowns | |
| Three-Quarter Crowns | |
| Retentive Grooves | |
| Porcelain Jacket Crown | |
| Indications of Laminates | |
| Metal Ceramic Restorations | |
| Types of Finish Lines and their Indications | |
| Pier Abutment | |
| Lost Salt Technique | |
| Maryland Bridge | |
| Rochette Bridge | |
| Virginia Bridge | |
| Miscellaneous | Gingival Retraction |
| Failure of Abutment | |
| Cementation and post- cementation problems | Thickness of Luting Cement |
| Occlusal Disharmony | |
| Occlusal considerations | Variation between Centric Relation and Maximum Intercuspation |
| Canine Protected Occlusion | |
| Bennett Shift | |
| Bennett Movement | |
| Working Side | |
| Non-Working Side | |
| Selective Grinding | |
| Beyron’s Point | |
| Types of Bone Quality | |
| Obturators |
1. Single best answer
2. Image based questions
3. True or false type questions
Please watch the above featured video for more detailed explanation about this article.
We hope this blog will assist you in preparing this subject meticulously for MDS entrance exams.
Prepare judiciously..
SOURCE: MERITERS!!

Source- textbook of pathology for dental students Ramdas Nayak and pinterest


Step 1 – Choose the right equipment:
What you will need:
1. A quality stethoscope
2. An appropriately sized blood pressure cuff
3. A blood pressure measurement instrument such as an aneroid or mercury column sphygmomanometer or an automated device with a manual inflate mode.
Step 2 – Prepare the patient:Make sure the patient is relaxed by allowing 5 minutes to relax before the first reading. The patient should sit upright with their upper arm positioned so it is level with their heart and feet flat on the floor. Remove excess clothing that might interfere with the BP cuff or constrict blood flow in the arm. Be sure you and the patient refrain from talking during the reading.
Step 3 – Choose the proper BP cuff size: Most measurement errors occur by not taking the time to choose the proper cuff size. Wrap the cuff around the patient’s arm and use the INDEX line to determine if the patient’s arm circumference falls within the RANGE area. Otherwise, choose the appropriate smaller or larger cuff.
Step 4 – Place the BP cuff on the patient’s arm: Palpate/locate the brachial artery and position the BP cuff so that the ARTERY marker points to the brachial artery. Wrap the BP cuff snugly around the arm.
Step 5 – Position the stethoscope: On the same arm that you placed the BP cuff, palpate the arm at the antecubical fossa (crease of the arm) to locate the strongest pulse sounds and place the bell of the stethoscope over the brachial artery at this location.
Step 6 – Inflate the BP cuff:Begin pumping the cuff bulb as you listen to the pulse sounds. When the BP cuff has inflated enough to stop blood flow you should hear no sounds through the stethoscope. The gauge should read 30 to 40 mmHg above the person’s normal BP reading. If this value is unknown you can inflate the cuff to 160 – 180 mmHg. (If pulse sounds are heard right away, inflate to a higher pressure.)
Step 7 – Slowly Deflate the BP cuff: Begin deflation. The AHA recommends that the pressure should fall at 2 – 3 mmHg per second, anything faster may likely result in an inaccurate measurement.
Step 8 – Listen for the Systolic Reading: The first occurence of rhythmic sounds heard as blood begins to flow through the artery is the patient’s systolic pressure. This may resemble a tapping noise at first.
Step 9 – Listen for the Diastolic Reading: Continue to listen as the BP cuff pressure drops and the sounds fade. Note the gauge reading when the rhythmic sounds stop. This will be the diastolic reading.
Step 10 – Double Check for Accuracy: The AHA recommends taking a reading with both arms and averaging the readings. To check the pressure again for accuracy wait about five minutes between readings. Typically, blood pressure is higher in the mornings and lower in the evenings. If the blood pressure reading is a concern or masked or white coat hypertension is suspected, a 24 hour blood pressure study may be required to assess the patient’s overall blood pressure profile.
Further Reading/References:
https://www.suntechmed.com/support/product-training-tutorials/1692-how-to-measure-blood-pressure
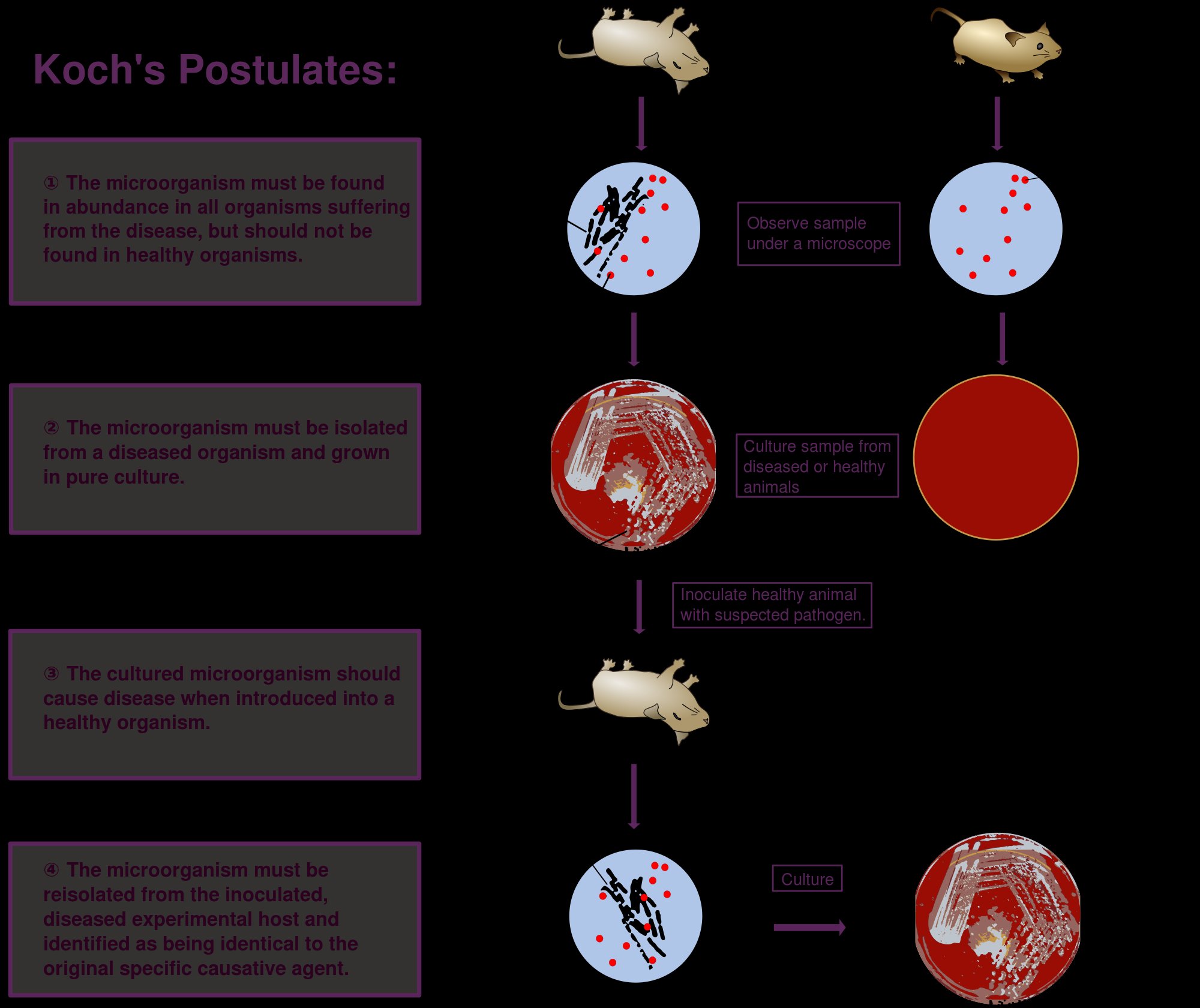
Robert Koch was a German practicioner. He is also known as the father of microbiology.
Koch’s postulates:
According to Koch’s postulates, a microorganism can be accepted as the causative agent of an infectious disease only if the following conditions are fulfilled.
(i) The organism should be constantly associated with the lesions of the disease.
(ii) It should be possible to isolate the organism in pure culture from the lesions of the disease.
(iii) The isolated organism (in pure culture) when inoculated in suitable laboratory animals should produce a similar disease.
(iv) It should be possible to re-isolate the organism in pure culture from the lesions produced in the experimental animals.
Source- textbook of microbiology C P Baveja and Google images
