Raymond P. Begg — Australian orthodontist; favourite student of Edward H. Angle
Trained under Angle using the edgewise appliance
Returned to Australia → patients came from very far away → wanted to see patients once every 6 weeks → needed a simple, low-compliance, efficient appliance
Developed the Light Wire Differential Force Technique (also called Begg technique)
Worked alongside AJ Wilcock, an Australian metallurgist, who designed the high-tensile wire specifically for Begg
Begg was NOT a self-promoter — no marketing, worked quietly → it was Kesling who propagated his work more than Begg himself
Why Begg Broke Away from Angle
Angle’s Philosophy
Begg’s New Philosophy
Non-extraction in ALL cases
Extraction when indicated
Occlusion-based treatment planning
Soft tissue profile + occlusion considered
Bodily movement (edgewise)
Uncontrolled tipping → then uprighting
High anchorage demand → headgear
Low anchorage demand → no headgear needed
Heavy rectangular wires
Light round wires (AJ Wilcock)
Key insight: Both Begg AND Tweed (also Angle students) observed massive relapse in non-extraction cases → jaws couldn’t accommodate all teeth → independently concluded extraction was necessary
PART 2: TWO THEORIES — PHILOSOPHICAL BACKBONE
Theory 1: Theory of Attritional Occlusion
STONE AGE MAN │ ├── Diet: Coarse food (bones, raw meat, grain) ├── Proximal attrition → 10.56 mm reduction/arch ├── Occlusal attrition → vertical dimension decreases └── Result: Space created for all 32 teeth including 3rd molars → Perfect alignment → No crowding
CIVILIZED MAN (Today) │ ├── Diet: Soft, refined, melt-in-mouth food ├── No proximal attrition → no space gained ├── No occlusal attrition └── Result: Crowding → 3rd molar impaction → malocclusion = "Disease of Civilization" (like diabetes, hypertension)
NACF (Natural Anterior Component of Force):
Hereditary tendency for teeth to drift anteriorly
In Stone Age man: NACF + proximal attrition = accommodated 3rd molars
In modern man: NACF present but no attrition → crowding
NACF + continued eruption in absence of attrition → basis of Begg’s extraction philosophy
Begg’s quote:“When in doubt, extract” (Note: this is NOT followed in contemporary practice — we now use continuing diagnosis)
Sir’s clinical observation: Even second molars are now getting impacted — the same phenomenon Begg described is worsening generation by generation due to increasingly soft diets.
Theory 2: Theory of Differential Force (Storey & Smith)
⚠️ Exam trap: Experiment used edgewise brackets (NOT Begg brackets) and studied canine retraction ONLY (NOT entire anterior segment)
Force Applied
Effect on Canine
Effect on Molar
Outcome
Light (150–200g)
Optimal → Frontal resorption → Steady movement
Sub-optimal → Does NOT move
✅ Retraction + Anchorage preserved
Heavy (>200g)
Supra-optimal → Hyalinization → Lag phase → Sudden dump
Optimal → Molar PROTRACTS
❌ Anchorage LOST
Why this happens:
Ideal orthodontic force = 22–26 g/cm² of root surface area(must say “per cm²” for full marks)
Canine root area = small → 150–200g = OPTIMAL → frontal resorption → steady movement
Molar root area = large → 150–200g = SUB-OPTIMAL → no movement
Heavy force on canine → Hyalinization (avascular necrotic zone) → Undermining resorption (osteoclasts tunnel from adjacent bone) → Lag phase → sudden movement dump
Simultaneously heavy force on molar = OPTIMAL → molar protracts → anchorage LOST → “dishing in” of profile
PART 3: BEGG APPLIANCE — THREE KEY COMPONENTS
Component
Details
Function
Ribbonwise bracket (inverted Angle bracket)
Wire enters from gingival side, NOT occlusal side
Permits uncontrolled tipping in BOTH mesiodistal AND buccolingual planes
AJ Wilcock high-tensile wire
Zero stress relaxation; light force maintained for 6 weeks
Light, constant, lasting force — precursor to HANT wires
Round molar tube (0.022″)
Free sliding; double back bend pre-built in; two-point contact with round wire
Anchorage preservation + free anterior sliding
Ribbonwise Bracket — Orientation
ANGLE'S EDGEWISE BRACKET (original): Wire enters from OCCLUSAL side Slot: 0.022" × 0.028" rectangular → Bodily movement → High anchorage demand
BEGG BRACKET (inverted): Wire enters from GINGIVAL side Wide open slot → 0.022" round wire → Uncontrolled tipping freely in: ├── Mesiodistal plane (crown goes distal, root mesial) └── Buccolingual plane (crown goes labial/lingual freely) → Low anchorage demand ✓ → Single point contact in both planes → EXCEPT for rotation: Two-point contact (wire touches base + bracket → generates couple)
Round Molar Tube — Two-Point Contact
ROUND WIRE IN ROUND TUBE:
┌───────────────────────┐ │ · · │ ← Two-point contact └───────────────────────┘ Mesial end Distal end
Two-point contact → COUPLE formed Couple → aims at BODILY MOVEMENT of molar Molar does NOT tip mesially → Anchorage preserved Simultaneously: Wire slides FREELY anteriorly → Canine/anterior retraction with low friction ✓
BUT: Round wire in round tube = NO buccolingual control → In 5-extraction cases needing B-L molar control: → Use DOUBLE BACK BEND in oval tube
AJ Wilcock Wire — Properties & Comparison
Property
AJ Wilcock Wire
Heat-Activated NiTi (Modern)
Made by
AJ Wilcock (metallurgist)
Various manufacturers
Material
High-tensile stainless steel
Nickel-titanium
Stress relaxation
Zero
Very low
Force at 6-week recall
Same as day of placement
Near same
Historical significance
Precursor to all light-force wires
Modern equivalent
Recall interval
6 weeks
6–8 weeks
PART 4: CLASSIFICATION OF BEGG TECHNIQUE
BEGG TECHNIQUE │ ├── CONVENTIONAL / TRADITIONAL BEGG │ ├── Ribbonwise bracket (original Begg bracket) │ ├── AJ Wilcock wire │ ├── Original 3-stage philosophy │ └── Propagated by: Kesling, Fletcher, Viazis │ ├── MODIFIED BEGG │ ├── SAME philosophy as conventional │ ├── DIFFERENT bracket (NOT ribbonwise) │ └── Brackets: PAGE bracket, Chun Hoon bracket │ └── REFINED BEGG (Dr. VP Jayade) ├── SAME Begg ribbonwise bracket ├── SAME basic Begg tenets ├── CHANGED mechanics ├── 10° and 5° offset incorporated into molar tube └── More emphasis on finishing
📖 Reference: Refined Begg — book by Dr. VP Jayade; Dr Manjunath Sir personally studied each page of this book with Dr. Jayade during PG training
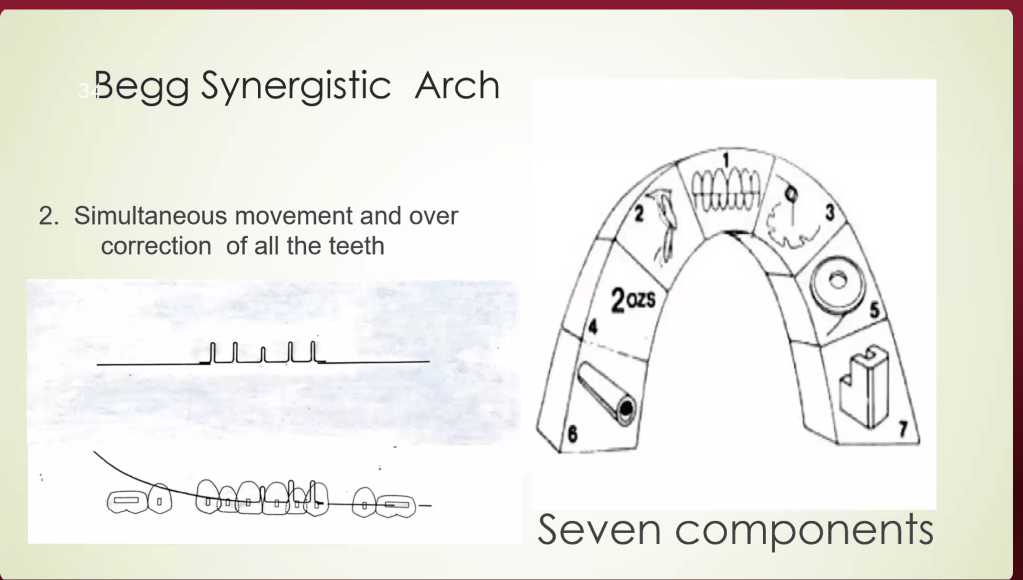
PART 5: BEGG SYNERGISTIC ARC (Kesling — 7 Components)
#
Component
Details
1
Diagnosis & Treatment Planning
Accounts for lack of attrition; extraction justified; overcorrection planned from start
2
Simultaneous movement
All teeth move at once (NOT sequential like standardized wire)
3
Simultaneous overcorrection
Both teeth AND jaws corrected simultaneously
4
Light intermaxillary elastics (IME)
Class II elastics used throughout treatment; light force
Permits uncontrolled tipping in B-L and M-D planes
7
AJ Wilcock wire
High-tensile; zero stress relaxation; light force
Begg separated crown-moving and root-moving forces into different stages → that’s why NO headgear, NO TPA was needed even in critical anchorage cases
PART 6: THREE STAGES OF BEGG TREATMENT
BEGG 3-STAGE TREATMENT FLOWCHART
┌──────────────────────────────────────────────────────────────┐ │ STAGE 1 │ │ ALIGNMENT & LEVELING │ │ │ │ Wire: AJ Wilcock 0.014" round │ │ Auxiliaries: Anchor bends, tip-back bends, Class II IME │ │ Pin used: STAGE 1 PIN (more play → free tipping) │ │ Wire type: MULTI-LOOP ARCH WIRE (MLAW) for crowded cases │ │ Movement: Uncontrolled tipping (alignment) │ │ Anchorage: FRIENDLY — no anchorage taxation ✓ │ │ Deep bite: Anchor bend → intrusion anteriors │ └─────────────────────────┬────────────────────────────────────┘ │ ▼ ┌──────────────────────────────────────────────────────────────┐ │ STAGE 2 │ │ SPACE CLOSURE │ │ │ │ Wire: AJ Wilcock 0.016" round │ │ Auxiliaries: Class II IME, space closure springs │ │ Pin used: STAGE 2 PIN (moderate play) │ │ Movement: Uncontrolled DISTAL tipping of anterior crowns │ │ Anchorage: STILL FRIENDLY ✓ │ │ Molar tube: Wire slides back freely; two-point contact │ │ prevents mesial molar tipping │ └─────────────────────────┬────────────────────────────────────┘ │ ▼ ┌──────────────────────────────────────────────────────────────┐ │ STAGE 3 │ │ TORQUING + UPRIGHTING (Root Movement) │ │ │ │ Wire: AJ Wilcock 0.020" round │ │ Auxiliaries: Torquing auxiliaries, uprighting springs │ │ (passive BRAKING springs — thick wire gauge) │ │ Pin used: STAGE 3 / HOOK PIN (minimal play → root control) │ │ Movement: Controlled ROOT movement │ │ Crowns: HELD in place by braking springs │ │ Roots: Moved lingually/distally (torquing + uprighting) │ │ ⚠️ ANCHORAGE CRITICAL HERE — root movement forces tend │ │ to move crown labially → anchorage taxation │ └──────────────────────────────────────────────────────────────┘
PART 7: ⭐ ANCHORAGE — CRITICAL PHASE COMPARISON (VIVA FAVOURITE)
Dr Manjunath Sir specifically called this a favourite VIVA question
Appliance
Anchorage Critical In
Reason
MBT / Straight Wire
Stage 1 — Alignment
Inbuilt mesial tip in all brackets (central, lateral, canine) → when full-size wire placed → mesial tipping → pulls molars mesially → anchorage loss → need TPA
Begg
Stage 3 — Torquing & Uprighting
Root movement forces → crown tends to move labially → anchorage taxation. Stages 1 & 2 are tipping against bodily movement of posteriors → anchorage FRIENDLY
PART 8: ⭐ BRAKING MECHANICS (MAJOR SECTION — EXAM IMPORTANT)
Braking = Preventing UNWANTED tooth movement to BUILD UP ANCHORAGE in the anterior segment
Braking in the Mesiodistal Plane:
SITUATION: Applying force for PROTRACTION of posteriors Problem: Anterior crowns want to tip DISTALLY (unwanted)
SOLUTION: Uprighting spring on anterior teeth ↓ Crown pushed MESIALLY Root goes distally Crown does NOT move distally ↓ Posteriors come forward ✓ Anteriors are held (braked) ✓
Braking in the Buccolingual Plane:
SITUATION: Force applied → Begg bracket permits free tipping Problem: Anterior crowns want to tip LINGUALLY (unwanted)
SOLUTION: Torquing auxiliary = PALATAL ROOT TORQUE (PRT) ↓ PRT → Labial crown torque Crown does NOT go lingually ↓ Anteriors held (braked) in B-L plane ✓
Braking in Contemporary Straight Wire:
Problem
Solution
Lower anterior torque in MBT = –6° = crown lingual
Increase lingual root torque in 0.019 × 0.025 wire
Crown going distal during protraction
V-bend (Gable bend) next to canines → anterior = anchorage unit
Key: Gable bend next to canines → moment is higher on anterior segment → aims at bodily movement → anterior = anchorage unit
PART 9: ⭐ CONTEMPORARY PROTRACTION MECHANICS
Sir explained the full sequence for posterior protraction in contemporary practice:
STEP 1: Consolidation → Figure-of-8 ligation from 3 to 3 → Entire anterior root surface combined → Force applied on posteriors becomes SUBOPTIMAL for anteriors to move → Posteriors come forward, anteriors stay ✓
STEP 2: Wire Cylinderization (posterior segment) → Thin/round wire in posterior → Less friction → posteriors slide forward more easily
Sir’s teaching:“You should be biomechanically strong. Without TADs, without headgear, you can treat critical anchorage cases with correct biomechanics alone.”
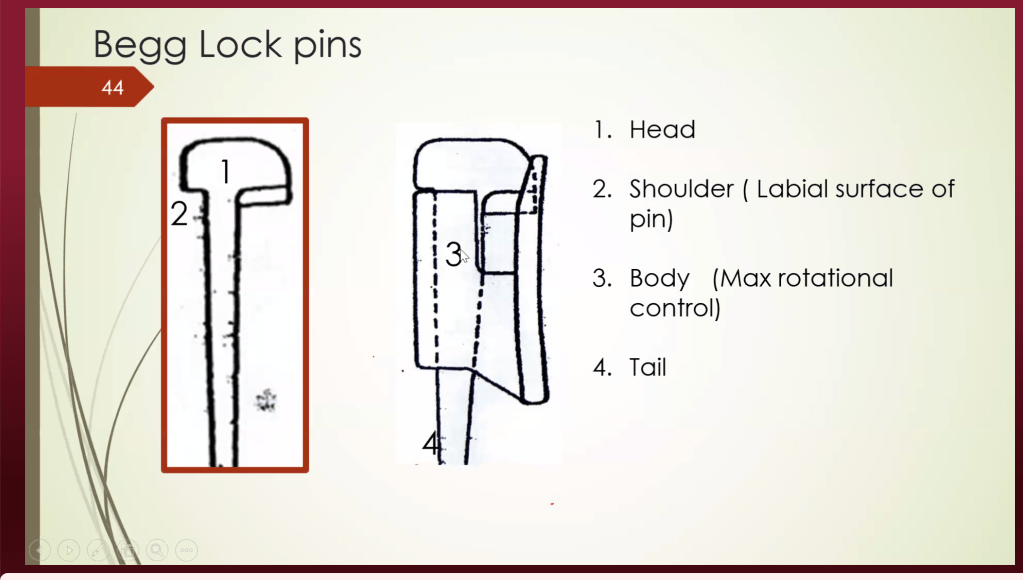
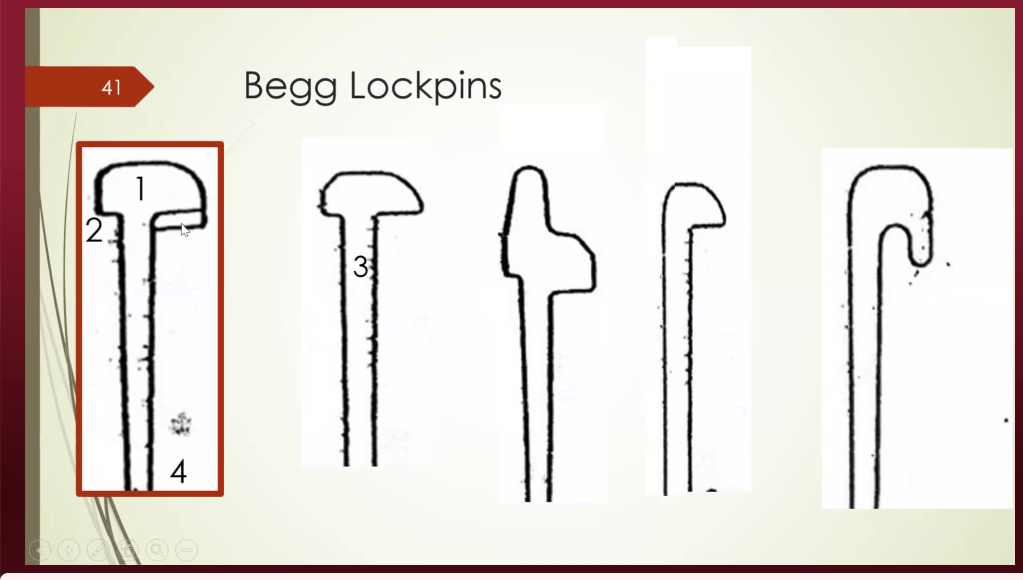
PART 10: BEGG BRACKETS — LOCK PINS (DETAILED)
The wire in the Begg bracket is held using brass lock pins, NOT ligature wires:
Root movement (torquing + uprighting); holds all corrections achieved in Stage 1 & 2
🔑 More play in pin → more tipping. Less play → more crown control → root movement.
PART 11: MULTI-LOOP ARCH WIRES (MLAW)
A unique Begg Stage 1 feature — used for severe crowding:
MLAW — MECHANISM:
Loops added into AJ Wilcock stainless steel wire │ ├── Increases LENGTH of wire ├── Increases FLEXIBILITY in looped segment └── Rigid end → canine tipping/retraction Looped end → aligns crowded anteriors simultaneously
SIMULTANEOUS ACTIONS IN STAGE 1: ┌─────────────────────────────────────────┐ │ 1. Space creation (distal tip of canine)│ │ 2. Alignment of crowded anteriors │ │ 3. Intrusion (deep bite correction) │ │ 4. Derotation (bends incorporated) │ └─────────────────────────────────────────┘
Contemporary equivalent: Rigid sectional wire on anchor segment + Flexible sectional wire on crowded segment → Same simultaneous correction principle
PART 12: ANCHOR BEND = GABLE BEND — BIOMECHANICAL PRINCIPLE
ANCHOR BEND (Begg) = GABLE BEND (Contemporary)
Examples: • Anchor bend closer to MOLAR → Molar = anchorage → Intrusion of anteriors • Gable bend next to CANINE → Anterior = anchorage → Safe for protraction
PART 13: TIP EDGE — BEGG’S MODERN EQUIVALENT
Tip Edge Appliance by Kesling = uses Differential Straight Wire Technique
Same philosophy as Begg: tipping first, then uprighting
Tip Edge bracket = Begg tipping freedom + edgewise finishing capability in ONE bracket
If you cannot practice conventional Begg in your college → learn Tip Edge → same biomechanical principles
PART 14: CLINICAL CASE — RELAPSE LESSON
Sir presented a 25-year-old female, non-extraction spacing case, relapsed after 4 years with space reopening lateral to lateral:
Causes of relapse:
Eruption / mesial drift of third molar → NACF → lower incisors procline → upper space reopens
Bolton’s discrepancy (smaller lateral incisors) → if retracted without build-up/IPR → relapse inevitable
Untreated soft tissue imbalance → profile not corrected → relapse
Retainer note: Sir does NOT give fixed retainer canine to canine (canine occlusion breaks it). Fixed retainer lateral to lateral + Hawley in upper arch.
Clinical pearl:“Always warn patients — maintain retainers until third molars have fully erupted or been extracted.”
PART 15: EXTRACTION vs. NON-EXTRACTION — CLINICAL DECISION MAKING
Sir’s clinical guidelines (from 23 years of experience):