
Rabie et al., Angle Orthodontist, 2003;73:457–465
Rabie et al., Angle Orthodontist, 2003;73:457–465
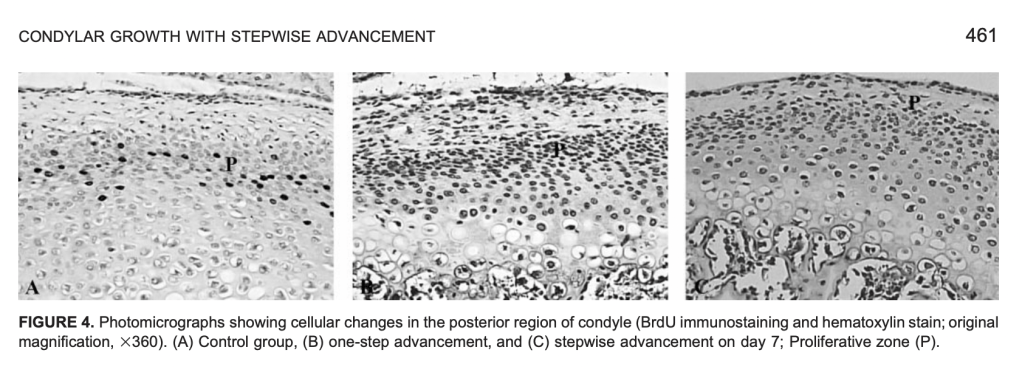
Stepwise mandibular advancement → Mechanical strain → ↑ Replicating mesenchymal cells → ↑ Osteoprogenitor population → ↑ Bone formation → ↑ Condylar growth potential
| Parameter | Details |
|---|---|
| Animal | 250 female Sprague-Dawley rats |
| Age | 35 days |
| Control | Natural growth |
| One-step (OS) | 3.5 mm advancement + 3 mm inferior displacement |
| Stepwise (SW) | 2 mm initial advancement → +1.5 mm on Day 30 |
| Cell marker | BrdU immunostaining |
| Assessment | Replicating mesenchymal cells + new bone formation |
| Regions studied | Anterior, middle & posterior condyle |
| Main site of response | Posterior condyle |
Forward mandibular positioning
↓
Stretching of posterior condylar tissues
↓
Mechanical strain
↓
↑ Mesenchymal cell replication
↓
Mesenchymal cells → chondroblasts / osteoblasts
↓
Cartilage formation + vascular invasion
↓
Endochondral ossification
↓
First advancement: 2 mm
Second advancement: +1.5 mm on Day 30
Cell proliferation precedes bone formation.
| Feature | One-Step | Stepwise |
|---|---|---|
| Advancement | 3.5 mm at once | 2 mm → +1.5 mm |
| Initial cellular response | Greater | Lower |
| Cell replication | Early increase → declines | Repeated increase after each advancement |
| Bone formation | Early peak → declines | Sustained/repeated increase |
| Long-term effect | Returns toward natural growth | Greater bone formation |
| Day 60 bone formation | Similar to natural growth | 49% higher |
First advancement
→ recruits mesenchymal cells
→ cells proliferate
→ differentiate
→ bone formation
Second advancement
→ provides new mechanical stimulus
→ recruits another population of replicating cells
→ increases osteoprogenitor pool
→ additional bone formation
“Advance → Recruit → Differentiate → Form bone → Advance again → Recruit again.”
Rabie et al. demonstrated that stepwise mandibular advancement produces repeated mechanical strain, increasing mesenchymal cell replication in the posterior condyle; this expands the osteoprogenitor cell population and subsequently enhances endochondral bone formation and condylar growth potential.
Banks P, Carmichael G.
JCO. 1999;33(11):620–623.
Instead of advancing the mandible immediately to an edge-to-edge incisor position, advancement is performed gradually using chairside-activated advancement screws + acetal resin spacers.
Large overjet + limited mandibular protrusion → gradual advancement without forcing the mandible forward.
Edge-to-edge bite registration
⬇️
May cause:
Small initial advancement
⬇️
Adaptation
⬇️
Progressive advancement
⬇️
Reduced overjet
✅ Greater orthopedic effect
✅ Less incisor tilting
✅ Better patient comfort
✅ Better speech
✅ Improved compliance
✅ Better appliance positioning during sleep
Maxillary appliance blocks
⬇️
Contain advancement screws
⬇️
Activated by inserting:
Different spacer thicknesses allow controlled incremental advancement.
| Screw | Maximum/indicated advancement |
|---|---|
| Standard screw | Up to 7 mm |
| 16 mm screw | For greater activation |
| 20 mm screw | For very large advancement |
Up to 12 mm stepwise advancement
12-year-old female
Modified Twin-Block
→ Stepwise mandibular advancement
→ Correct overjet
Extraction of maxillary first premolars
Fixed appliances
→ Align and level both arches
Overjet = 12 mm
Maximum comfortable protrusion = only 3 mm
⬇️
3 mm
⬇️ 6–8 weeks
+3 mm spacer
⬇️ 6–8 weeks
+3 mm spacer
⬇️ 6–8 weeks
+2 mm spacer
⬇️
3 + 3 + 3 + 2 = 11 mm
⬇️
Overjet reduced to 0 mm
| Stage | Duration |
|---|---|
| Active Twin-Block phase | 7 months |
| Continued full-time wear | 2 additional months |
| Maxillary first premolar extraction | During continued Twin-Block wear |
| Fixed appliance therapy | 17 months |
| Total active treatment | 24 months |
12 mm overjet
but
Only 3 mm initially
⬇️
❌ Immediate large advancement difficult
⬇️
✅ Start with 3 mm advancement
⬇️
Gradually add spacers
⬇️
Progressive mandibular advancement
⬇️
1. Assess maximum comfortable mandibular protrusion
↓
2. Start with a small advancement
↓
3. Allow neuromuscular adaptation
↓
4. Review at approximately 6–8 weeks
↓
5. Add bilateral spacers
↓
6. Reassess overjet and patient comfort
↓
7. Continue progressive advancement until correction
⭐ Severe overjet
⭐ Limited mandibular protrusive movement
⭐ Patients unable to posture edge-to-edge
⭐ Patients who may not tolerate large initial advancement
⭐ Cases requiring large total mandibular advancement
Initial mandibular advancement
with
Total required overjet correction
Initial advancement: 3 mm
Overjet: 12 mm
The patient does not need to achieve 12 mm advancement immediately.
Instead:
Small advancement → adaptation → reactivation → further advancement
🔹 Modified Twin-Block allows chairside progressive mandibular advancement
🔹 Advancement achieved using screws + cylindrical acetal resin spacers
🔹 Initial advancement can be small when mandibular protrusion is restricted
🔹 3 + 3 + 3 + 2 mm incremental advancement in the reported case
🔹 12 mm overjet → 0 mm overjet
🔹 Active Twin-Block phase: 7 months
🔹 Total active treatment: 24 months
🔹 16 mm and 20 mm screws may be required for greater activation
Banks and Carmichael described a modified Twin-Block appliance that permits controlled, progressive mandibular advancement using advancement screws incorporated into the maxillary blocks and cylindrical acetal resin spacers. This approach is particularly advantageous in patients with severe overjet who cannot initially posture the mandible to an edge-to-edge position. By using small incremental advancements at 6–8-week intervals, muscular adaptation and patient comfort may be improved while potentially reducing unwanted incisor tipping. In the reported 12-year-old patient, an initial 3 mm advancement was progressively increased by 3 mm, 3 mm and 2 mm spacers, reducing a 12 mm overjet to zero over a 7-month Twin-Block phase.
“Can’t advance 12 mm? Don’t force it—start at 3 mm, adapt, add spacers, and advance step-by-step.”
Ng J, Major PW, Heo G, Flores-Mir C.
American Journal of Orthodontics and Dentofacial Orthopedics. 2005;128:212–219.
To determine how much true incisor intrusion is actually achieved during orthodontic treatment.
When incisors appear to intrude clinically, how much is genuine intrusion versus apparent intrusion caused by growth or other tooth movements?
Apical movement of the tooth’s center of resistance/root relative to a stable skeletal reference.
Clinical crown appears to move apically
≠
True intrusion of the entire tooth
Apparent intrusion may result from:
| Incisor group | Mean true intrusion |
|---|---|
| Maxillary incisors | ~1.5 mm |
| Mandibular incisors | ~1.9 mm |
True incisor intrusion is possible, but the amount achieved is relatively small.
Forces should be directed through or near the center of resistance.
Correct force vector
→ Intrusive movement
Incorrect force vector
→ Intrusion + tipping
Loss of posterior anchorage may produce:
Posterior extrusion
↓
Mandibular clockwise rotation
↓
Apparent bite opening
This may be mistaken for true incisor intrusion.
In growing patients:
may influence measured intrusion.
Labial tipping of incisors
can produce an apparent reduction in overbite without equivalent bodily intrusion.
Ng et al. (2005), in a systematic review and meta-analysis, evaluated the amount of true incisor intrusion achieved during orthodontic treatment. The study demonstrated that genuine incisor intrusion is achievable, but the magnitude is relatively limited, approximately 1.5 mm for maxillary incisors and 1.9 mm for mandibular incisors. Therefore, the reduction in overbite observed clinically should not be attributed entirely to true incisor intrusion, as it may also result from incisor inclination changes, posterior tooth extrusion, mandibular rotation, and growth-related changes. This finding emphasizes the importance of distinguishing true intrusion from apparent or pseudo-intrusion when evaluating deep-bite correction.
“Deep bite correction ≠ pure intrusion; true intrusion is modest—~1.5 mm upper, ~1.9 mm lower.”
Danz JC et al. European Journal of Orthodontics. 2014;36:522–530
| Parameter | Finding |
|---|---|
| Study design | Retrospective long-term follow-up |
| Original sample | 855 former orthodontic patients |
| Eligible deep bite cases | 185 |
| Final analyzed complete-treatment sample | 43 |
| Relapse cases | 4/43 |
| Median follow-up | 11.9 years |
| Relapse definition | Incisor overlap <50% after treatment → ≥50% at follow-up |
| Relapse prevalence | 10.3% |
| Median increase in overlap in relapse group | 6.7% |
| Range of increase | 3.2–19.8% |
| Stable cases | ~90% |
| Major conclusion | Long-term vertical relapse was low and clinically small |
Increased vertical overlap of maxillary and mandibular incisors
Measured as:
1. Dentoalveolar
2. Skeletal
Growth
→ Mandibular growth rotation
Function
→ Muscular and functional influences
Dental changes
→ Incisor overeruption
→ Loss of arch form
→ Lower incisor crowding
→ Upper anterior spacing
Periodontal remodeling
→ Reorganization of periodontal tissues
Retention
→ Inadequate or absent retention
Treatment outcome
→ Incomplete leveling
→ Persistent deep bite
→ Poor incisor contact
Other factors
→ Lower lip pressure
→ Sagittal relapse
→ Bolton discrepancy
→ Interincisal angle
↓
Intrude upper and/or lower incisors
Best when: Excessive incisor eruption contributes to deep bite
↓
Pseudo-intrusion
Incisor proclination increases effective vertical clearance.
↓
Posterior tooth eruption
↓
Possible clockwise mandibular rotation
↓
↑ Lower anterior facial height
↓
Open bite / reduce deep bite
⚠️ Clockwise rotation does not necessarily occur in every patient.
More stable than expected
90% remained without vertical relapse
Only 10.3% demonstrated recurrence to ≥50% incisor overlap.
And even in these cases:
The amount of relapse was small
Median increase = 6.7%
This is the most clinically important message from the study.
T1: Deep bite
↓
T2: Successfully corrected
↓
T3: Deep bite returns
T1: Deep bite
↓
T2: Still deep bite
↓
T3: Deep bite persists or worsens
Deep bite at long-term follow-up was more likely due to PARTIAL CORRECTION than TRUE RELAPSE.
| Group | Deep bite at T3 |
|---|---|
| True relapse | 4 patients |
| Partial treatment | 7 patients |
Finish the correction!
Incomplete leveling and incomplete establishment of anterior contact may be more problematic than relapse after successful correction.
Persistent deep bite + incomplete treatment
→ ↑ Gingival contact
→ ↑ Palatal impingement
→ ↑ Risk of traumatic contact
In the relapse group:
Absence of retention may facilitate:
⚠️ However: The study was not large enough to prove retention as a relapse risk factor.
Possible explanations:
Median age at T2 ≈ 17 years
↓ Less remaining growth
More periodontal remodeling may have occurred before debonding.
Majority received:
Most patients achieved:
The study could not identify reliable predictors of deep bite relapse because:
No clinically reliable prediction model for individual deep bite relapse could be established.
☐ Deep bite fully corrected
☐ Curve of Spee adequately leveled
☐ Stable anterior incisor contact
☐ No gingival contact
☐ No palatal impingement
☐ Evaluate incisor inclination
☐ Assess interincisal angle
☐ Check arch form
☐ Check anterior spacing
☐ Evaluate sagittal relationship
☐ Plan long-term retention
Monitor for:
🔍 Increased overbite
🔍 Loss of anterior contact
🔍 Upper anterior spacing
🔍 Lower anterior crowding
🔍 Loss of arch length
🔍 Sagittal relapse
🔍 Growth-related mandibular rotation
Long-term relapse of successfully treated moderate deep bite was relatively uncommon and small. Approximately 90% remained stable after a median 11.9-year follow-up, while 10.3% showed relapse, with a median increase in incisor overlap of only 6.7%. Importantly, persistent deep bite at long-term follow-up was more commonly associated with incomplete treatment than true relapse.
“Correct it completely → Establish anterior contact → Retain it → Relapse is usually small.”
| Parameter | Miniscrew Mechanics | Utility Arch |
|---|---|---|
| Indication in study | Deep bite ≥4 mm + excessive gingival display + normal vertical dimensions | Same |
| Patients | Postpubertal; mean age 20.9 yrs | Mean age 15.25 yrs |
| Appliance | 4 maxillary incisors bonded | 4 maxillary incisors + maxillary first molars banded |
| Initial leveling | 0.016″ and 0.016 × 0.022″ NiTi | Passive preformed NiTi utility arch |
| Working wire | 0.016 × 0.022″ SS anterior segment | 0.016 × 0.016″ blue Elgiloy |
| Miniscrew position | Distal to maxillary lateral incisors | — |
| Miniscrew size | 1.2 mm × 6 mm | — |
| Loading | 1 week after placement | — |
| Intrusion force | 80 g | — |
| Force application | Close to center of resistance | Through utility arch |
| Treatment duration | 6.61 ± 2.95 months | 6.61 ± 2.46 months |
| Intrusion rate | 0.44 mm/month | 0.27 mm/month |
| Incisor vertical movement | 2.97 mm | 1.81 mm |
| True intrusion at CR | 1.75 mm | 0.86 mm |
| Incisor protrusion | 0.79 mm — NS | 3.91 mm — significant |
| Incisor angular change | 3.85° — NS | 13.55° — significant |
| Molar movement | No significant movement | Distal tipping |
| Overbite reduction | 2.18 mm | 2.32 mm |
| Root resorption | No signs detected in miniscrew group | Not evaluated in this study |
| Main advantage | True intrusion + minimal protrusion + minimal posterior side effects | Effective overbite correction but greater incisor proclination and molar tipping |
| # | Question | Answer |
| 1 | Define friction in orthodontics | Force opposing relative motion between two systems (bracket, archwire, ligation) that are in contact |
| 2 | Why is friction inevitable in orthodontics? | Because the bracket, archwire, and ligation are always in physical contact during sliding mechanics |
| 3 | Name the two types of friction | Static friction and kinetic friction |
| 4 | Define static friction | Friction that opposes an applied force; its magnitude equals whatever is needed to prevent motion until overcome. |
| 5 | Define kinetic friction | Friction that opposes the direction of motion once movement has started; usually less than static friction. |
| 6 | Which type of friction is clinically more relevant in orthodontics, and why? | Static friction, because continuous sliding motion along the archwire rarely occurs clinically. |
| 7 | Why is kinetic friction considered practically irrelevant in tooth movement? | Because orthodontic tooth movement is not continuous sliding but an intermittent, quasi-static process. |
| 8 | What is meant by “quasi-static thermodynamic process” in sliding mechanics? | A slow process that passes through a sequence of states close to equilibrium, rather than true continuous motion. |
| 9 | Who authored the classic critical review on friction and resistance to sliding? | S. Jack Burrow, published in AJO-DO 2009. |
| 10 | What does resistance to sliding (RS) mean? | The total resistance encountered by a wire sliding through a bracket comprises friction, binding, and notching. |
| # | Question | Answer |
| 11 | In sliding mechanics, where are forces applied relative to the center of resistance (Cres)? | Away from the center of resistance of the segments being moved |
| 12 | What is the consequence of applying force away from Cres? | It generates moments that tip the segments in different planes |
| 13 | Describe the sagittal-plane effect of retraction force in extraction cases | Anterior segment tips distally, posterior segment tips mesially |
| 14 | Describe the transverse-plane effect | Mesial out-rotation of canines and mesial in-rotation of premolars |
| 15 | Describe the vertical-plane effect | Deepening of the bite |
| 16 | How does frictionless mechanics counter these unwanted moments? | Alpha and beta moments incorporated into loops compensate for the moments generated by the applied force |
| 17 | How does sliding mechanics generate the necessary counteracting moments? | Through the interaction between bracket and wire (contact and binding), not through loop bends |
| 18 | What is expressed as a result of bracket-wire interaction in sliding mechanics? | First, second, and third order movements (tip, torque, in-out) |
| 19 | Why is understanding sliding biomechanics a prerequisite to understanding friction’s role? | Because friction’s clinical significance depends on how forces and moments are generated during sliding |
| 20 | What produces the tipping, torqueing, and in-out corrections in sliding mechanics if not loop bends? | Interactive contact/binding between archwire, bracket, and ligation |
| # | Question | Answer |
| 21 | Is friction entirely undesirable in orthodontics? | No; friction is both a hindrance during sliding and a necessity for generating corrective couples |
| 22 | What is desired during retraction with sliding mechanics? | Reduced friction so the wire can freely slide through the bracket |
| 23 | What stops further tipping of a tooth during retraction? | Contact of the bracket with the wire, which prevents further tipping |
| 24 | What creates the moment of the couple during retraction? | Classic frictional contact between bracket and wire plus the wire’s resilience |
| 25 | What moment is induced in the anterior segment during retraction? | Distal root uprighting moment |
| 26 | What moment is induced in the posterior segment during retraction? | Mesial (root) uprighting moment |
| 27 | What happens after the uprighting movement occurs? | The frictional contact between bracket and wire is relieved |
| 28 | What happens to the tooth once contact is relieved? | It is free to tip again for the next cycle |
| 29 | What is this repeating cycle called? | Stick-slip phenomenon, also called “walking of the canine” |
| 30 | Is stick-slip specific to canine retraction only? | No; a similar contact-based couple is created for torqueing and in-out movements as well |
| 31 | Summarize the ideal friction requirement in sliding mechanics | Low friction is needed for sliding, but adequate frictional contact is needed to deliver couples |
| 32 | What are the two opposing frictional requirements in sliding mechanics called (concept)? | The friction paradox — lower friction desired for translation, higher friction/binding desired for couple generation |
| # | Question | Answer |
| 33 | Why is force decay necessary in regular sliding mechanics? | For the couple from bracket-wire interaction to be adequately expressed for tip, torque, and in-out correction |
| 34 | What happens if the applied force does not decay or is too high? | The couple generated will be inadequate for tipping, torqueing, and in-out movements to occur |
| 35 | Which reference discusses force decay in incisor retraction with mini-implant anchorage? | Upadhyay, Yadav, and Nanda, Journal of Orthodontics 2014 |
| 36 | How does high sustained force affect binding-generated couples? | It prevents adequate binding-based couple generation needed for correction movements |
| # | Question | Answer |
| 37 | Name three clinical scenarios where sliding mechanics is typically used | Generalized spacing cases, premolar extraction cases, enmasse distalization with implants |
| 38 | Does implant-assisted space closure fall under friction or frictionless mechanics? | Friction mechanics, since it involves the archwire sliding through brackets |
| 39 | What is the major biomechanical difference between conventional and implant-assisted sliding? | Difference in space utilization and line of force |
| 40 | How much anchorage loss occurs with implant-assisted sliding? | Almost none — anchorage conservation is nearly full |
| 41 | Which types of space closure can be achieved with implant-supported sliding? | Group A or Group C space closure |
| 42 | Why is the line of force diagonal in implant-assisted sliding? | Because implants are usually placed higher than the molar hooks |
| 43 | How does implant placement affect the line of force relative to Cres? | It brings the line of force closer to the center of resistance |
| 44 | What effect does this closer line of force have on the moments generated? | Moments are of lesser magnitude compared with conventional mechanics |
| 45 | What effect does lower moment magnitude have on the required couple? | The moment of the couple required also becomes lesser |
| 46 | Can the line of force be modified in implant mechanics? | Yes, infinitely, based on implant and hook position relative to the case requirement |
| # | Question | Answer |
| 47 | Who developed V-bend sliding mechanics and when? | Thomas F. Mulligan, in the 1970s |
| 48 | What is the primary clinical application of V-bend mechanics? | Closing space by moving individual teeth (canine retraction or molar protraction) |
| 49 | What key concept did Mulligan introduce? | Differential moment as a means of effective intraoral anchorage |
| 50 | How is differential moment achieved? | By applying unequal alpha and beta moments |
| 51 | How are moments and forces applied separately in V-bend mechanics? | Moments via the continuous archwire and its bends; force via auxiliaries like elastomeric chain or closed-coil springs |
| 52 | Why is an off-center V-bend used? | To create unequal moments, with a higher moment applied to the anchorage teeth |
| 53 | How does bend position affect wire segment length and moment? | Bend closer to a bracket shortens that wire segment; shorter wires have higher bending moments than longer wires |
| 54 | Which bracket experiences the higher moment: closer or farther from the V-bend? | The bracket closer to the V-bend |
| 55 | How does a higher moment affect tipping of that segment? | The segment with higher moment undergoes less tipping for the same reciprocal force, establishing differential anchorage |
| 56 | What V-bend angle is used for 0.016″ round stainless steel wire? | 45° |
| 57 | What V-bend angle is used for 0.018″ wire? | 30° |
| 58 | What V-bend angle is used for 0.020″ wire? | 15° |
| 59 | What is the relationship between wire size and V-bend angle? | Inverse relationship — thinner wire needs a larger V-bend angle |
| 60 | Who published the force system analysis of V-bend sliding mechanics? | Siatkowski RE, JCO 1994 |
| # | Question | Answer |
| 61 | State the first law of friction | Frictional force is proportional to the normal applied load by a constant, the coefficient of friction |
| 62 | State the second law of friction | The coefficient of friction is independent of apparent contact area |
| 63 | State the third law of friction | The coefficient of friction of a couple is independent of the sliding velocity |
| 64 | According to the second law, should bracket/wire dimensions matter clinically? | Theoretically no, but clinically dimensions matter with respect to the critical contact angle |
| 65 | Why does dimension still matter despite the second law? | Because dimensions determine the critical contact angle, beyond which binding/notching (not classical friction) dominates |
| # | Question | Answer |
| 66 | Who proposed dividing resistance to sliding into three components? | Kusy and Whitley . |
| 67 | Name the three components of resistance to sliding | Friction (FR), binding (BI), notching (NO) . |
| 68 | Define friction (FR) component | Static or kinetic friction due to wire contact with flat bracket surfaces . |
| 69 | Define binding (BI) component | Contact between wire and the corners of the bracket, occurring when the tooth tips or wire flexes . |
| 70 | When does binding occur clinically? | When a force applied to move a tooth causes it to tip until the wire contacts the bracket corners . |
| 71 | Define notching (NO) component | Permanent deformation of the wire at the wire-bracket corner interface . |
| 72 | Is notching reversible? | No, it represents permanent wire deformation . |
| 73 | What is the sequence of resistance components as contact angle increases? | Friction → Binding → Notching |
| # | Question | Answer |
| 74 | Define the contact angle (θ) | The angle between the archwire and the bracket slot |
| 75 | Define the critical contact angle (θc) | The angle boundary between classical frictional behavior and binding/notching phenomena . |
| 76 | What happens when θ ≤ θc? | Classical friction occurs |
| 77 | What happens when θ > θc? | Binding and notching begin, increasingly restricting sliding mechanics . |
| 78 | What is the theoretical maximum θc for nominal bracket/wire dimensions? | Approximately 3.7 degrees for standard slot sizes . |
| 79 | What range does θc typically fall within? | Between 0 and approximately 4 degrees . |
| 80 | Who established the mathematical derivation for θc? | Kusy and Whitley (EJO 1999) . |
| 81 | Why is knowledge of both wire AND bracket dimensions necessary to calculate θc? | Knowledge of the archwire-bracket combination is needed, not either component alone . |
| 82 | What clinical strategy minimizes binding and notching? | Selecting archwire and slot size combinations that keep the contact angle low |
| 83 | Should sliding mechanics ideally begin when θ is much less than θc, equal to θc, or greater? | Sliding should be initiated when θ approximates θc, avoiding over-alignment before sliding and avoiding exceeding θc . |
| # | Question | Answer |
| 95 | Why would an orthodontist prefer stainless steel wires for sliding mechanics? | Lowest surface roughness and coefficient of friction, giving more efficient force delivery |
| 96 | Why might beta-titanium be avoided during heavy sliding mechanics despite good elasticity? | Higher friction and greater variability in frictional forces reduce efficiency of force delivery |
| 97 | How does implant-assisted sliding reduce the friction-related side effects of conventional sliding? | By reducing moment magnitude near Cres, it reduces the binding-generated moments and associated tipping |
| 98 | Compare frictionless and friction (sliding) mechanics in generating couples | Frictionless mechanics use built-in loop moments (alpha/beta); sliding mechanics rely on bracket-wire binding/friction contact |
| 99 | What is a clinical implication of understanding the critical contact angle? | It can help avoid unnecessary over-alignment before sliding and prevent excessive binding, potentially reducing treatment time . |
| 100 | Summarize the key biomechanical principle for effective sliding mechanics | Balance low sliding friction (for translation) with adequate binding contact (for necessary couple generation) while selecting materials/dimensions to control the coefficient of friction and critical contact angle |
| Approach | Indications |
|---|---|
| Extraction of lower premolars | Severe crowding, deep Curve of Spee, moderate negative overjet |
| Extraction of 3rd molars + distalization with TADs | Mild crowding, mild–moderate COS, mild–moderate negative OJ |
| MEAW therapy | Minimal crowding, moderate–severe COS, retreatments |
| Increase vertical dimension + Class III elastics | Low-angle cases, deep bite, minimal crowding |
| Approach | Effect |
|---|---|
| Extraction (premolars) | Faster incisor retraction, profile improvement |
| MBS distalization | Non-extraction, increases lower facial height, slower movement |
Study on 86 CBCTs: hyperdivergent, neutral, hypodivergent.
| Facial Type | Between 1st & 2nd Molars | Mesial Root of 2nd Molar | Distal Root of 2nd Molar |
|---|---|---|---|
| Hyperdivergent | 11 mm from crest | 9 mm from crest | 11 mm from crest |
| Neutral | 11 mm from crest | 11 mm from crest | – |
| Hypodivergent | 11 mm from crest | 11 mm from crest | – |
General conclusion:
| Feature | Liou IZC‑6 | Lin IZC‑7 |
|---|---|---|
| Position | Lateral to MB root of 6 | Lateral to MB root of 2nd molar |
| Buccal bone | Thin | Thick |
| Inter‑radicular risk | Often inter‑radicular | Mostly extra‑alveolar |
| En‑masse distalization | Some limitation | Facilitates |
| Root damage risk | Higher | Lower |
| Angle | 55°–70° | 55°–70° |
Three PA heights: 4 mm, 7 mm, 10 mm
| PA Height | Incisor Response | Canine Response |
|---|---|---|
| 4 mm (short) | More extrusion + lingual tipping | – |
| 7 mm (middle) | Preservation of anterior torque, no occlusal plane change | – |
| 10 mm (long) | Buccal tipping + intrusion of lateral incisors; no extrusion of centrals | Increased lingual tipping + extrusion |
Key point:
Conclusion:
Models:
Results:
Conclusion:
Conclusion:
Conclusion:
Conclusion:
