Why tooth position is about balance
Tooth position is not just about bones and brackets; it is about equilibrium between internal and external forces.
The classic equilibrium theory proposes that teeth settle where forces from the tongue, lips, cheeks, and periodontal ligament balance out. Earlier work suggested that:
- Lips and cheeks are usually more influential than the tongue for anterior tooth position.
- Resting pressures are more important than short bursts of functional pressure (speech, swallowing, chewing)
This background is crucial when we try to explain the characteristic retroclination of upper incisors in Class II Division 2.
The Class II Division 2 puzzle
Class II Division 2 is characterized by:
- Distal occlusion of the buccal segments
- Retroclined maxillary central incisors, often with deep overbite
Clinicians have long suspected that these retroclined upper centrals are “held back” by unusually high lip pressure, particularly from the lower lip resting on the palatal aspect of the incisors. At the same time, family and cephalometric data indicate a strong hereditary component; therefore, many authors have referred to “local genetic factors” influencing the lips and anterior dentoalveolar region.
The missing link until Lapatki et al. (2002) was solid experimental proof that lip pressure is actually higher in Class II Division 2 than in Class I, and an explanation of why.
What this study set out to test
Lapatki and colleagues designed a study with two key objectives:
- Compare resting lip pressure on maxillary central incisors (incisal and cervical areas) in Class II Division 2 vs Class I.
- Evaluate whether a high lip line and/or increased peri‑oral muscle activity explain any increase in resting lip pressure.
In other words: Is the problem due to where the lip sits (lip line), how hard the muscles work (hypertonicity), or both?
Key findings on lip line and incisor inclination
Two simple but powerful morphologic differences were found:
- The lip line in Class II Division 2 was, on average, around 5 mm above the incisal edge of the upper centrals, versus about 3 mm in Class I.
- The maxillary central incisors in Class II Division 2 were retroclined by roughly 16 degrees more than in the Class I controls.
Clinically, this means that in Class II Division 2 cases, more of the incisal portion of the upper centrals lies under the lower lip at rest, and the crowns are already tipped lingually.
Resting lip pressure: what actually changes?
The pressure data are the core of the paper:
- In Class I subjects:
- Incisal area often experienced slightly negative or low positive pressures.
- Cervical area typically had mild positive pressure from upper lip contact.
- In Class II Division 2 subjects:
- Incisal area usually had clearly positive pressure from the lower lip.
- Cervical area frequently showed negative pressure (a kind of “suction” or reduced contact).
Notably, the magnitude of negative pressure was similar in both groups; the real difference lay in the positive incisal pressure, which was more than twice as high in the Class II Division 2 group as the positive cervical pressure seen in controls.
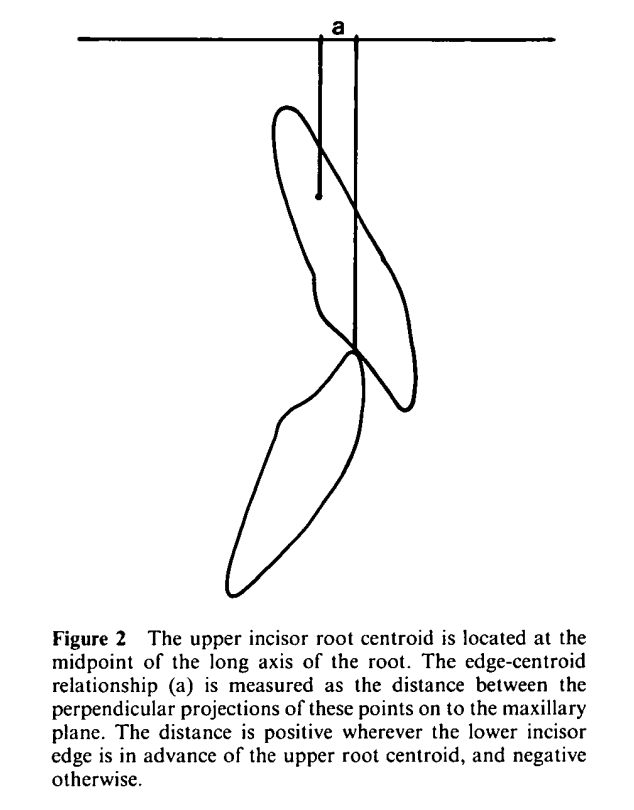
To reflect the real tipping effect, the authors combined incisal and cervical pressure into a weighted average (incisal pressure given more weight because it acts farther from the center of resistance). This effective “lingual tipping load” on the upper centrals was significantly higher in the Class II Division 2 group.
Is it just “strong lips”? EMG says no
Surprisingly, peri‑oral EMG did not show increased resting activity in any of the measured muscles in the Class II Division 2 group:
- No significant inter‑group differences for orbicularis oris (upper and lower), depressor labii inferioris, or mentalis.
- Subjects with hypertonic mentalis appeared in both groups with similar frequency.
- Correlations between EMG activity and lip pressure or lip line were weak and not statistically significant.
So, the data do not support the idea that Class II Division 2 is driven by globally “hyperactive” peri‑oral muscles at rest. Instead, something about the geometry of the lips and teeth seems more important.
Lip line as the key driver
Correlations between lip line and pressure were strong:
- Higher lip line → higher positive incisal pressure
- Higher lip line → more negative or reduced cervical pressure
- Higher lip line → greater overall lingual tipping effect (weighted pressure)
ANCOVA showed that these relationships held across both groups, and there was no significant difference in slope or intercept between Class I and Class II Division 2 when lip line was used as a covariate. In simple terms:journals.sagepub+1
- Wherever the lip is positioned vertically, it determines how much and where pressure is applied to the crown.
- A higher lip line means the lower lip engages more of the incisal surface of the upper centrals, boosting their lingual tipping moment.
Thus, the “local genetic factor” seems to be the vertical relationship between lip line and anterior dentoalveolar structures, not an inherently overactive lip musculature.
How does this fit with clinical Class II Division 2 patterns?
Several well‑known clinical observations become easier to explain:
- Central incisors more retroclined than laterals/canines
Centrals are usually more extruded and thus more deeply engaged by the lower lip. Lateral incisors and canines tend to be shorter and more labial, so they may lie outside the main zone of lip contact, escaping the full tipping effect.
- Labially placed upper laterals or canines
If centrals retrocline early, laterals and canines may erupt relatively labially and can be maintained labial if space is limited or they are less covered by the lower lip.
- Mandibular rotation and soft tissue “excess”
Counter‑clockwise mandibular rotation and infra‑occlusion of buccal segments, often described in Class II Division 2, can increase soft tissue redundancy in the lower face and contribute to a cranially displaced lip line.
The picture that emerges is one where skeletal pattern, tooth eruption, and lip line geometry interact to place the centrals in a zone of sustained, elevated resting pressure.
Clinical implications for orthodontic treatment
For clinicians, the take‑home message is pragmatic and important:
- Class II Division 2 cases are inherently prone to relapse if the underlying lip–tooth equilibrium is not altered.
- Simply proclining upper incisors without addressing the lip line and vertical position of the crowns may leave the lower lip still exerting a high lingual tipping force.
- The authors conclude that intrusion combined with proper torque of the maxillary incisors should be a priority, as this can lower the effective contact of the lower lip on the incisal edges and reduce non‑physiologic resting pressure.
In other words, “stability by design” means repositioning the incisors so that their new equilibrium lies closer to a physiologic balance of lip and tongue forces, rather than continuing to fight an unchanged, unfavorable lip‑pressure environment.