1. CONCEPT OF PRESCRIPTION IN ORTHODONTICS
What Is a “Prescription”?
- The symbol Rx originates from the Eye of Horus (Egyptian mythology) — god of healing, protection, and health
- In Latin, “recipe” = “to take”
- As per Samuel Weinstein (Prof., University of Connecticut): “If malocclusion is a disease, orthodontic treatment is a cure. The medicine is force.”
Components of the Orthodontic Appliance
| Type | Examples |
|---|---|
| Active | Archwires (NiTi, SS), elastic chains, coil springs |
| Passive | Brackets, bands, tubes |
- Bracket = a passive handle used to apply forces via wire engagement
- Materials: plastic, stainless steel, ceramic, titanium
- The prescription (tip, torque, in-out) is built into the bracket or molar tube
2. HISTORICAL EVOLUTION OF BRACKET SYSTEMS
| Year | Appliance/Event | Key Feature |
|---|---|---|
| 1900 (approx.) | E.H. Angle — Active arch / E-arch | Teeth tied to arch with gold ligature wire; screw for expansion |
| 1910 | Pin and Tube Appliance | Pin attached to tube; direction of pin guided tooth alignment |
| Pre-1928 | Ribbon Arch Appliance (Angle) | First prototype of bracket; vertical slot; lacked torque and tipping control |
| 1928 | Edgewise Appliance (Angle) | Horizontal slot; wire inserted edge-on; major breakthrough |
| Post-1928 | Begg Bracket (modification of Ribbon Arch) | Used round wires instead of rectangular; active tipping via wire deflection |
| Post-1928 | Swain’s Modification | Added curved wings (Levy’s bracket) for rotation correction |
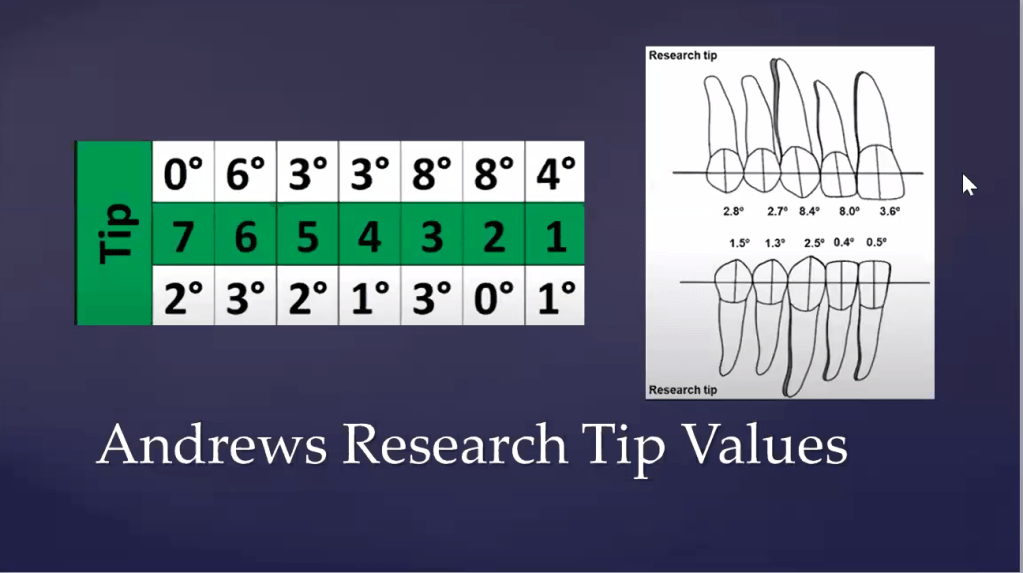
| 1965 | Andrews’ Straight Wire Appliance | Built-in angulation + inclination + prominence in bracket |
| 1970 | SWA came into clinical existence | |
| 1989 | SWA textbook published | “The Straight Wire — Concept and Appliance” |
Edgewise = wire inserted edge-on (the edge of the rectangular wire enters the horizontal bracket slot)
Edgewise Bracket Modifications (CME/Twin Bracket Types)
- Extra-wide bracket
- Intermediate bracket
- Standard bracket
- Junior bracket (smallest of all) — named “Sajesh Singh”
3. ANDREWS & THE 6 KEYS TO OPTIMAL OCCLUSION
Andrews studied 120 individuals with ideal untreated occlusion (1962–1972) to derive these keys:
| Key | Description |
|---|---|
| Key 1 – Molar Relationship | MB cusp of upper 1st molar in buccal groove of lower 1st molar; mesiolingual cusp of upper 1st molar in central fossa of lower 1st molar; distal ridge of upper 1st molar occludes with distal ridge of lower 2nd molar |
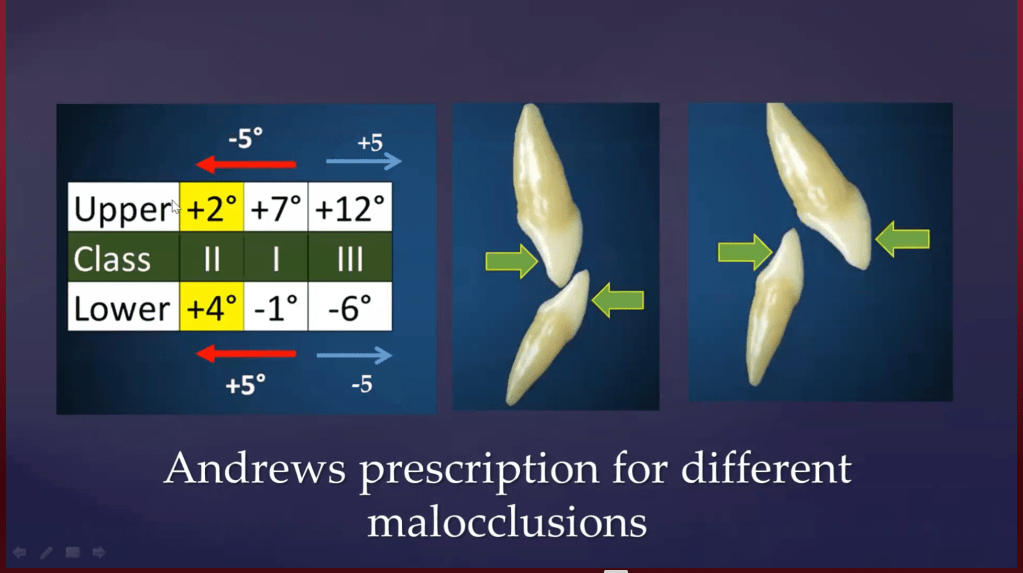
| Key 2 – Crown Angulation (Tip) | Crown is mesially inclined; gingival portion of long axis is distal to crown — present in all teeth; needed for mesial component of force and masticatory efficiency |
| Key 3 – Crown Inclination (Torque) | Crown is labially inclined in anteriors; progressively lingually inclined in posteriors; facilitates mutual protected occlusion |
| Key 4 – Absence of Rotation | No unwanted rotations = no premature contacts, no untoward crossbites |
| Key 5 – Tight Contacts | No spacing; prevents tooth migration and secondary malocclusion |
| Key 6 – Curve of Spee (Flat) | Curve of Spee ≈ flat (0–1.5 mm); deep curve → crowding; reversed curve → spacing |
4. WIRE BENDING CLASSIFICATION
A. Based on Purpose
| Type | Description | Example |
|---|---|---|
| Primary Bends | Essential bends for alignment | 1st, 2nd, 3rd order bends |
| Secondary Bends | Compensate for bracket placement errors | Repositioning bends |
| Tertiary Bends | Auxiliary loops added to wire | U-loops, helical loops, stop bends |
B. Primary Bends (Orders)
| Order | Also Called | Plane | Purpose |
|---|---|---|---|
| 1st Order | In-Out bend / Horizontal bend / Offset bend | Horizontal (bucco-lingual) | Corrects labiolingual position; accounts for in-out prominence differences (lateral incisor set-in, molar prominence) |
| 2nd Order | Tip / Artistic bend / Vertical bend / Up-down bend | Vertical (mesiodistal) | Corrects mesiodistal crown/root angulation (tip); anchor bends, gable bends, step-up/step-down, V-bends are all 2nd order |
| 3rd Order | Torque | Labiolingual (root movement) | True torque = moves the ROOT labially or palatally; cannot be placed in round wires |
Key Point: Torque strictly refers to root movement only — not crown tipping
Why Straight Wire? — The 76-Bend Problem
Without prescription brackets, a plain edgewise bracket on a full arch requires:
- 76 total primary wire bends to passively seat the archwire
- 46 bends for angulation, inclination, and offset
- 33 bends for prominence and occlusal-gingival slot positioning
- Heavy SS wire needed → excessive force delivery
- Solution: Build all bends into the bracket → place a straight wire passively
5. ANATOMY OF THE BRACKET
| Part | Description |
|---|---|
| Wings | Used for ligation; modification possible for rotation control |
| Slot | Where archwire engages; slot is angulated/torqued to express prescription |
| Base | Bonded to tooth surface; can have varying stem height (for in-out) |
| Stem | Connects base to face/slot |
| Face | Outer surface of bracket |
| Identification marks | Distogingival laser etch or color-coding (indicates R/L) |
Level slot concept: All bracket slots across the arch should be in a single horizontal plane
6. GENERATIONS OF STRAIGHT WIRE APPLIANCE (SWA)
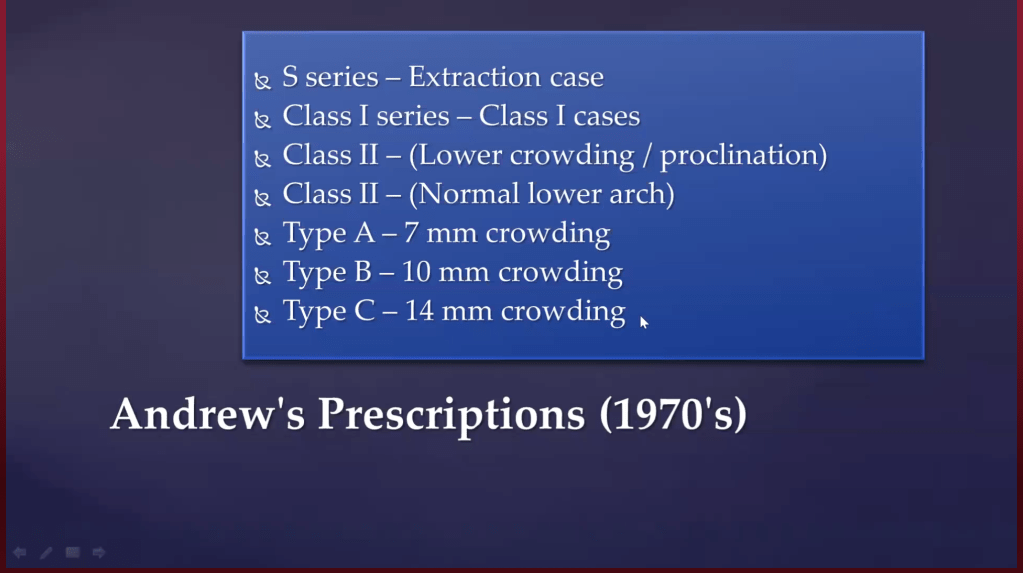
Generation 1: Andrews Prescription (1970)
Andrews derived values from 120 ideal occlusion cases:
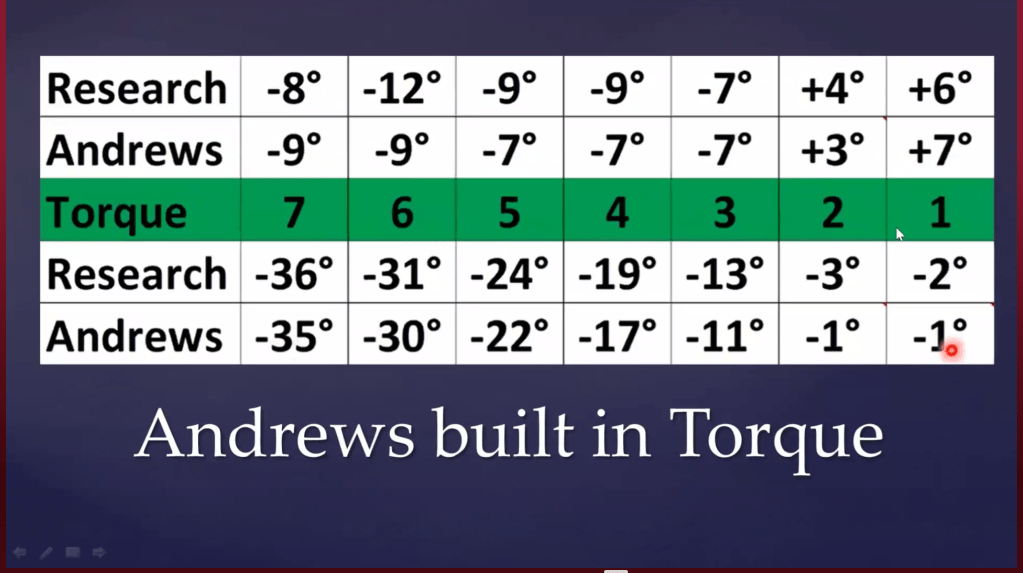
Andrews Torque Values (Ideal Occlusion):
| Tooth | Torque (°) |
|---|---|
| Max. Central Incisor | +6 |
| Max. Lateral Incisor | +4 |
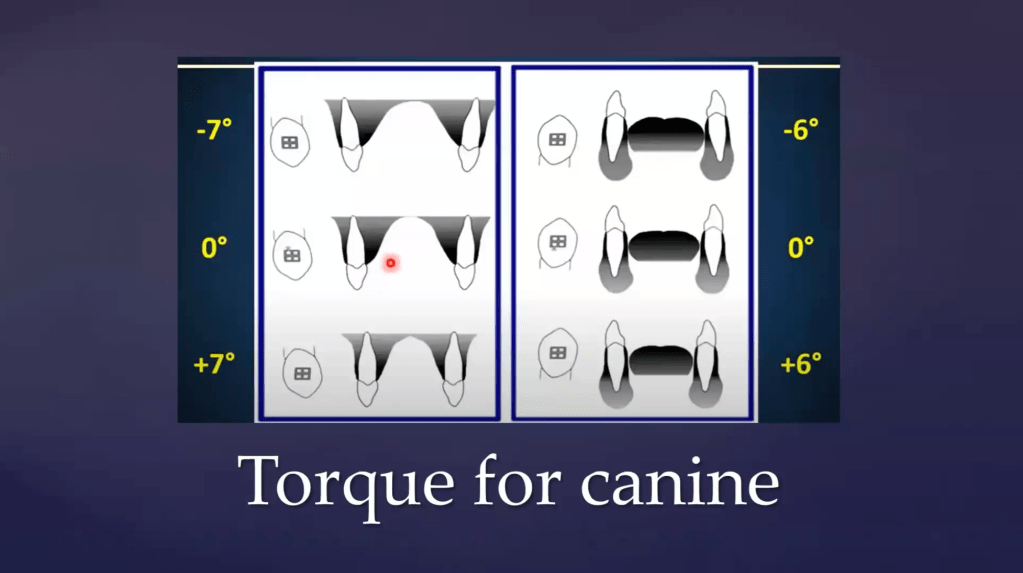
| Max. Canine | −7 |
| Max. Premolars | Progressively negative |
| Max. Molar | Progressively negative |
| Mand. Incisor | −2 |
| Mand. Molar | −36 |
Rationale for torque values:
- +6° (Central) → root centered in cortical plate; facilitates anterior guidance
- +4° (Lateral) → slightly less due to in-out difference between central and lateral
- −7° (Canine) → enables canine-guided occlusion; during lateral excursion, lower canine contacts palatal of upper canine, producing posterior disclusion on non-working side
- Negative posterior torque → creates Curve of Wilson; food bolus locking mechanism for masticatory efficiency
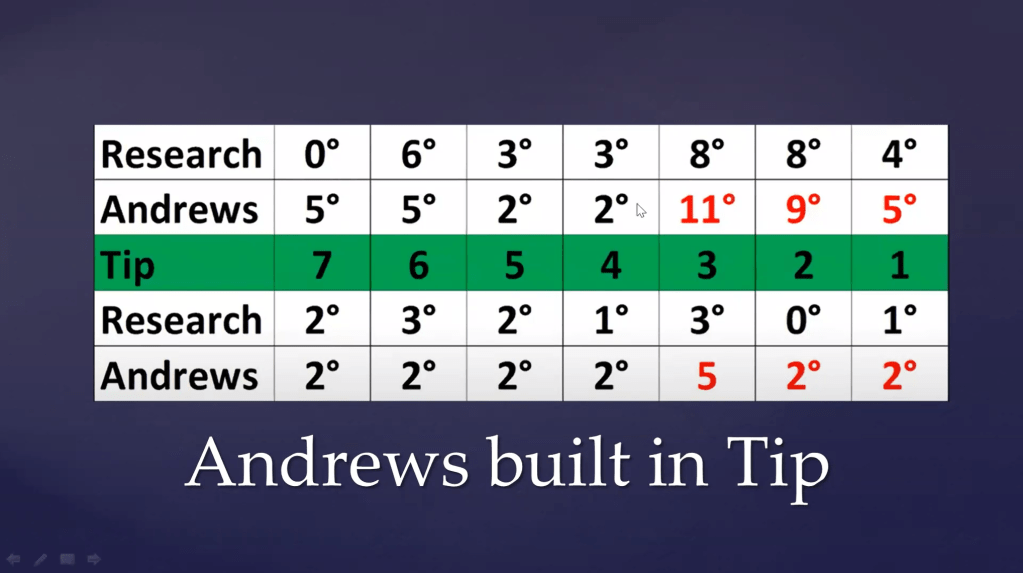
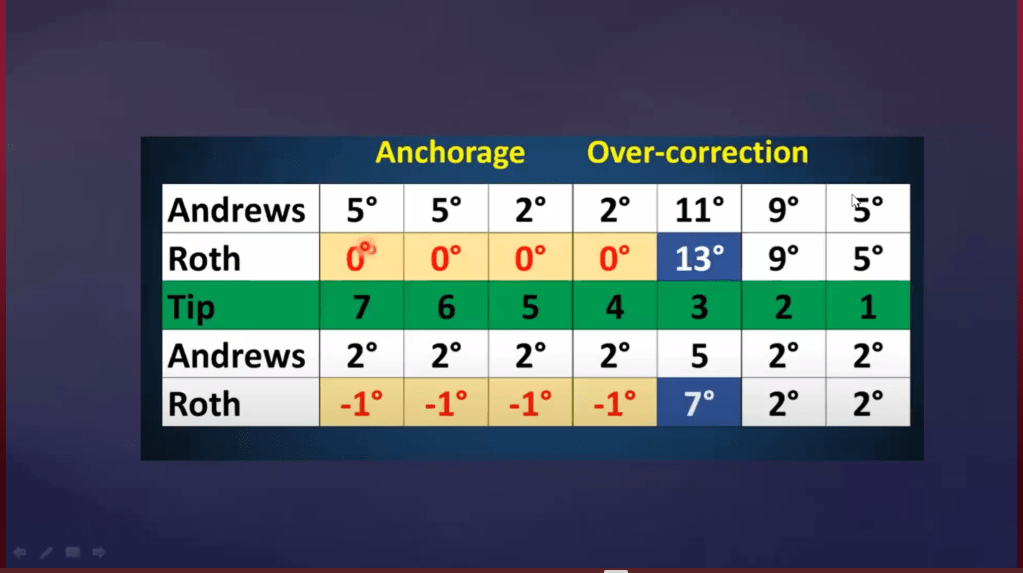
Andrews Tip Values: +5° central, +9° lateral, +11° canine; 0° premolars and molars
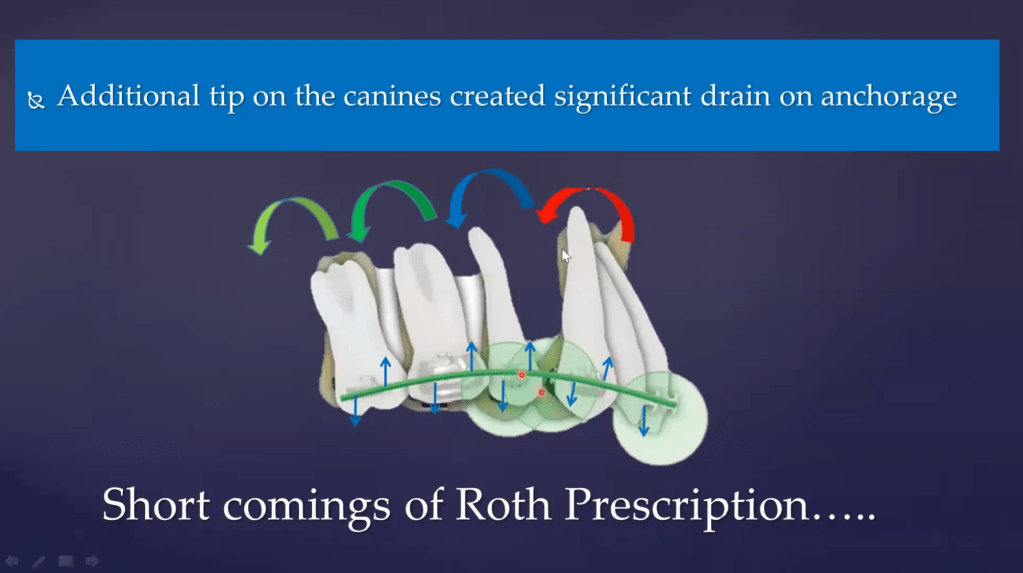
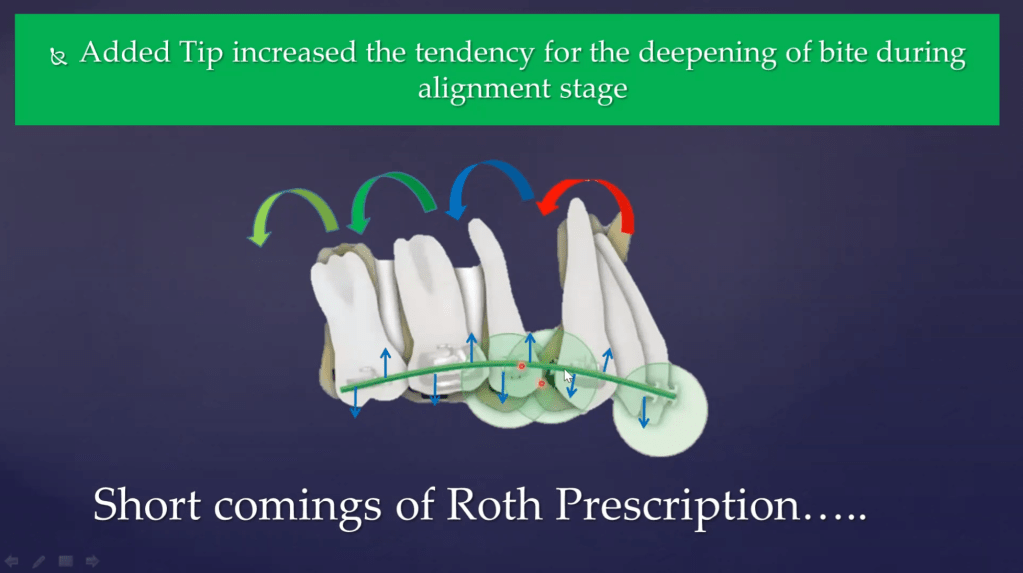
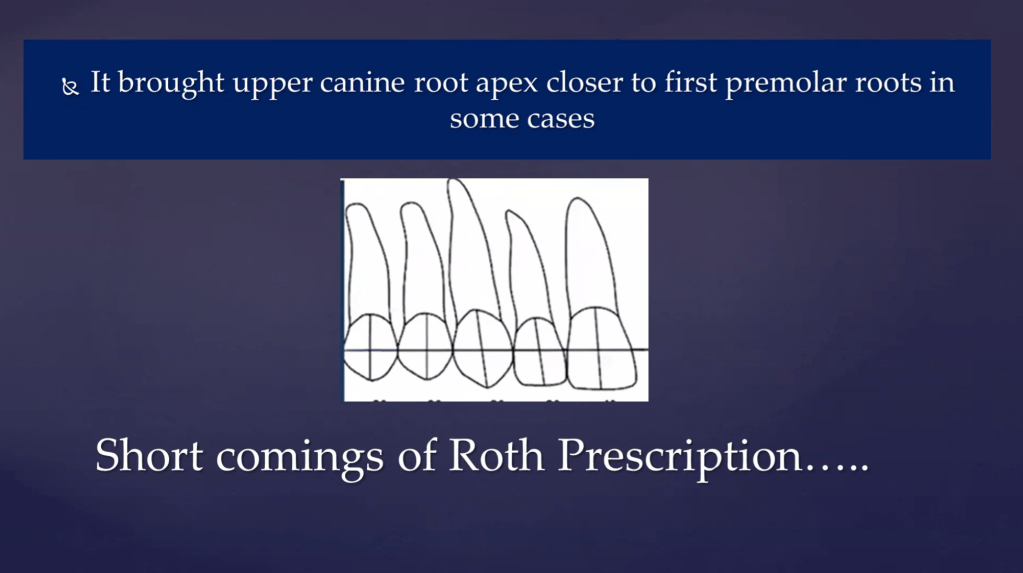
Generation 2: Roth Prescription (Modification of Andrews)
Roth’s 3 Core Concepts:
- Reduce inventory (simplify bracket types)
- Build in over-correction (correct beyond ideal to compensate for relapse)
- Achieve functional occlusion goals (canine guidance, mutually protected occlusion)
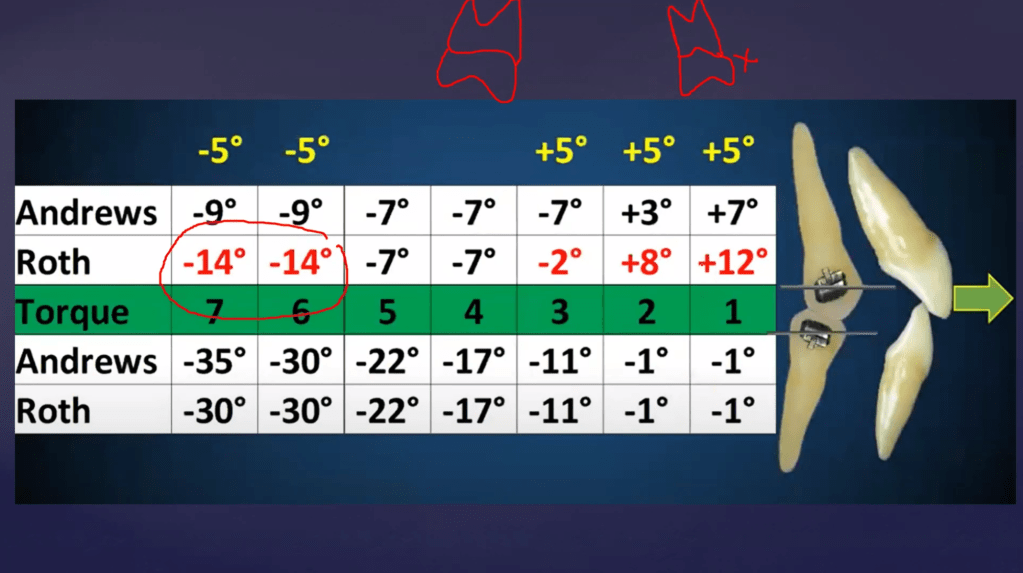
Changes Roth Made vs. Andrews:
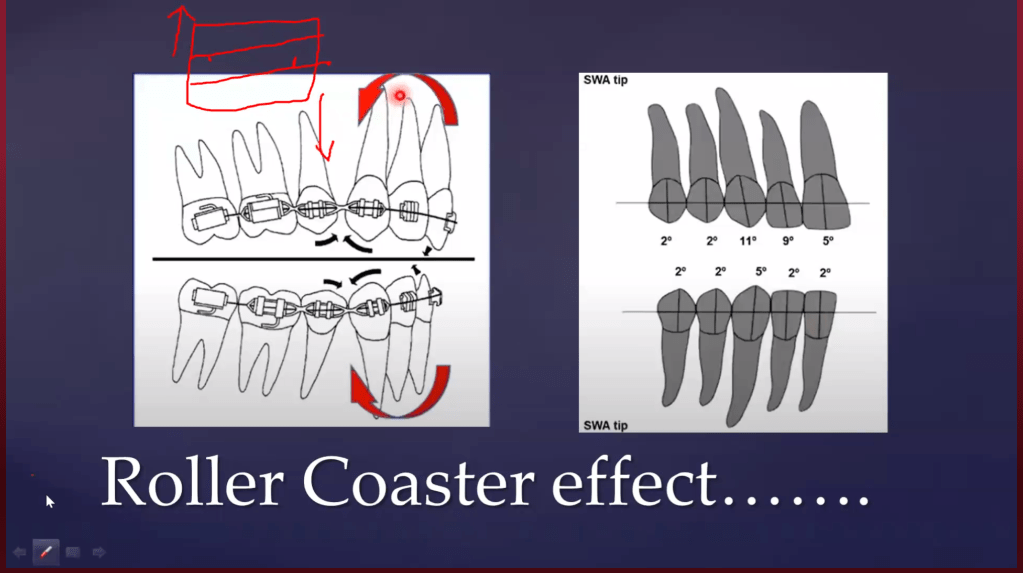
Roller-Coaster Effect:
- During canine retraction, there is a tendency for distal tipping of the crown and mesial tipping of the root
- This creates a “roller-coaster” arch profile
- Roth increased canine tip to 13° to pre-correct this, so that the canine translates bodily during retraction
Roth’s Problem (Anchor Loss):
- 13° tip expressed immediately in initial NiTi archwire → mesial movement of canine
- This occupied extraction space prematurely (anchor loss from the start
Generation 3: MBT Prescription (McLaughlin, Bennett, Trevisi)
Key Philosophy of MBT:
- Retract only on full-size rectangular SS wire (0.019×0.025 in 0.022 slot) to prevent roller-coaster effect mechanically
- E-chain retraction should not begin on lighter wires

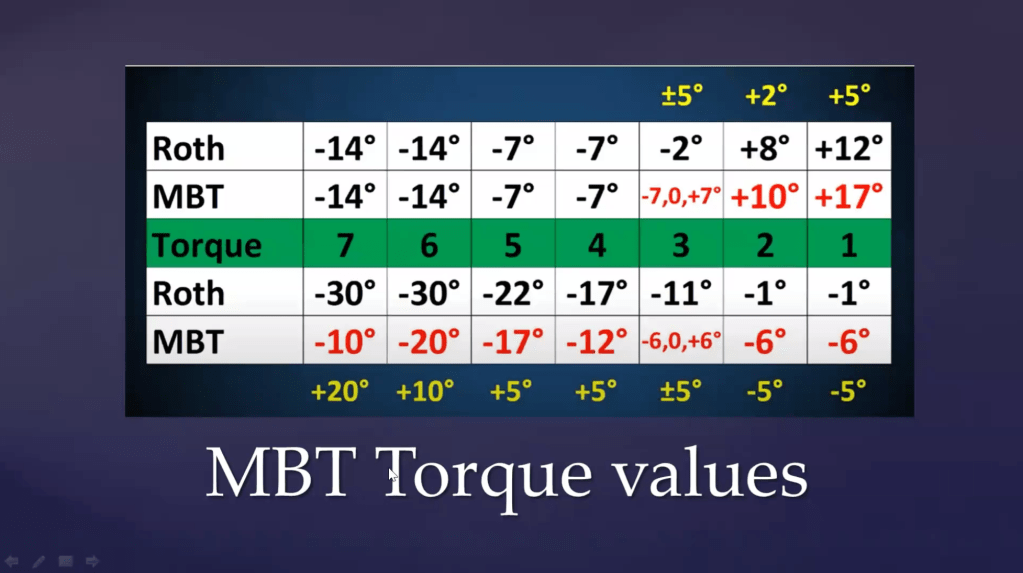
Changes MBT Made:
MBT for Lingually Placed Mandibular Lateral Incisor:
- Built-in torque of −6° (lingual crown torque) in MBT for lower incisors
- When aligning a lingually displaced lower lateral, as the crown is brought labially, the built-in torque counteracts the tendency for lingual root torque — no additional torque bending required
7. TORQUE EXPRESSION & SLOT SIZE
Slot Size Comparison
| Slot | Advantages | Preferred For |
|---|---|---|
| 0.018″ | More torque expression with full-size wire; less play; better for torque-sensitive cases | Non-extraction cases, torque control priority |
| 0.022″ | More play; works well with E-chain retraction on large wire; better sliding mechanics | Extraction cases, anchorage management |
For maximum torque expression:
- Use 0.018 slot + 0.016×0.022 SS wire (only 2° play)
- Wire stiffness: SS > TMA for torque; TMA acceptable for 2nd order bends
- Round wires cannot express 3rd order (torque) — must use rectangular wire
Bracket Placement Height & Torque
| Placement | Effect on Root Torque |
|---|---|
| Cervical | Lingual root torque (less expression) |
| Mid-crown (ideal) | Ideal torque expression |
| Incisal | Labial root torque (more expression) |
SAP (Straight Arch wire Placement) protocol: Must be very precise in bracket placement height as it directly controls torque expression
8. WAGON WHEEL CONCEPT (Andrews)
- Torque induces tip loss in a ratio of 4:1
- For every 4° of torque expressed → 1° of mesial tip is lost
- 20° torque = 5° mesial tip loss
- 40° torque = 10° mesial tip loss
- 90° torque = 23° mesial tip loss
- Mesial tip loss → all roots diverge → anchorage loss + tendency for spacing
Clinical implication: When using full-torque expression (e.g., MBT on SS), anchor cinch and proper retraction strategy are critical
9. ANTI-ROTATION BUILT INTO BRACKETS
During space closure with E-chain, unwanted rotations occur as side effects:
| Tooth | E-chain Side Effect | Built-in Anti-Rotation |
|---|---|---|
| Canine | Mesial-in, distal-out | Mesial-out, distal-in built into bracket |
| Premolar | Mesial-in, distal-out | Mesial-out, distal-in (opposite) |
- One wing is placed slightly further than the other to generate a counter-moment
- Net rotation = zero → tooth translates bodily
10. IN-OUT (PROMINENCE) DIFFERENCE
Why different stem heights between brackets?
| Tooth | Prominence | Stem Height |
|---|---|---|
| Max. Central Incisor | Most prominent | Least stem height |
| Max. Lateral Incisor | Set-in lingually | More stem height added |
| Canine | Intermediate | Intermediate |
| Mand. 2nd Premolar | Smaller than adjacent | Extra offset added |
| Molar | More buccal | Offset bend or increased stem |
All brackets, when placed, should bring all slots to the same labial level (level slot)
MBT Molar Tube (Buccal Tube) Features:
- Placed parallel to occlusal cusp → automatic 10° offset (takes care of molar in-out discrepancy)
- Zero degree tip
- ~14° torque built in
11. PRESCRIPTION CHOICE BY MALOCCLUSION
| Malocclusion/Situation | Preferred Prescription | Reason |
|---|---|---|
| Class II Div 1 — Critical anchorage | MBT | Zero/reduced tip in posterior = maximum anchorage conservation |
| Class II — Class 2 elastics | MBT | Excellent torque values; better force management |
| Class III — Class 3 elastics | Roth | Built-in torque assists in managing Class III dentoalveolar compensation |
| Crossbite (posterior) | Roth | Better posterior torque values counteract crossbite tendency |
| Scissor bite | MBT | Better torque control |
| Non-critical anchorage extraction cases | Andrews or Roth | Both acceptable; add wire bends for side effects |
Important caveat: Any prescription can be used for any case, but side effects must be compensated with appropriate wire bends, especially 3rd-order (torque) bends
Class II Finishing — Contralateral Molar Tube Trick
- In Class II finishing, using a lower 2nd molar tube on the contralateral upper 1st/2nd molar provides the needed rotation for Class II molar relationship without wire bending
12. TRAMPOLINE EFFECT
- When an active tieback is placed, the masticatory forces act on it like a trampoline
- The bouncing (juggling) forces of mastication continuously reactivate the tieback
- Forces are maintained for up to 3 months without patient revisit
- Clinical significance: Active tiebacks maintain space closure forces between appointments, unlike passive tiebacks or E-chains alone
13. KEY CLINICAL TIPS FROM DR. TARULATHA
- Torque is ONLY for root movement — never use the term for crown inclination changes alone
- Retraction should be done on full-size rectangular SS wire (MBT philosophy) to prevent roller-coaster effect
- Round wires cannot express 3rd order bends — always go to rectangular for torque needs
- Bracket placement height is critical — especially in SAP protocol; even 1 mm error changes torque expression significantly
- For torque expression: SS > TMA; use TMA only for 2nd order corrections
- Group A anchorage cases → use MBT; avoid Roth in high-anchorage-demand cases
15. SLOT SIZE & TORQUE EXPRESSION — DETAILED NUMBERS
Play (Degrees of Freedom) by Slot & Wire Combination
| Slot Size | Arch Wire | Play (°) | Torque Expression |
|---|---|---|---|
| 0.018″ | 0.016×0.022 SS | 6.8° | Moderate |
| 0.018″ | 0.018×0.025 SS | 1.2° | Excellent |
| 0.022″ | 0.016×0.022 SS | ~19.8° | Poor |
| 0.022″ | 0.019×0.025 SS | ~11.2° | Better; standard for MBT retraction |
| 0.022″ | 0.021×0.025 SS | ~minimal | Near-complete torque expression |
Key rule: To achieve full/complete torque expression, the slot must be filled snugly → requires 0.021×0.025″ SS in 0.022 slot
Summary: For best torque expression → prefer 0.018 slot with appropriate rectangular SS wire (only 1.2° play with 0.018×0.025 SS)
16. PRESCRIPTION CHOICE FOR CLASS II DIVISION 2
- Centrals are retroclined → roots are labially placed → need positive palatal root torque → MBT (+17°) is ideal for centrals
- Laterals are proclined (Class II Div 2 Type 1 laterals) → need roots to go labially → Roth (+8°) preferred for laterals
- Andrews (+7°) for centrals has less torque in comparison and may be insufficient for this caseConcept: You can mix prescriptions tooth-by-tooth within the same arch based on individual tooth requirements — this is called hybridizing or bracket prescription maneuvering
17. BRACKET PRESCRIPTION MANEUVERING — DETAILED
Using the same bracket inventory in alternative ways — inverting, switching, swapping, or substituting — to achieve a variable/customized prescription without needing custom brackets.
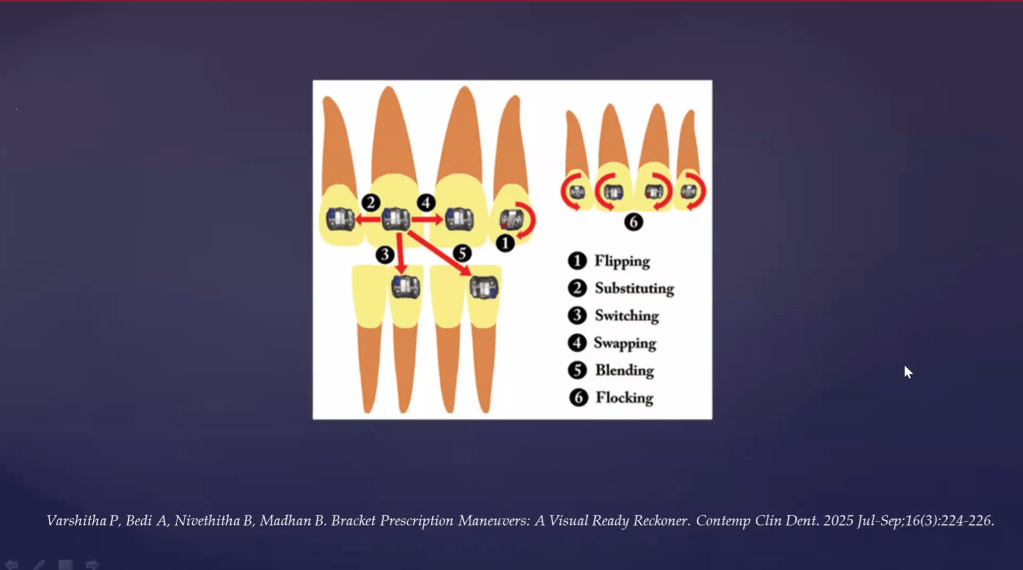
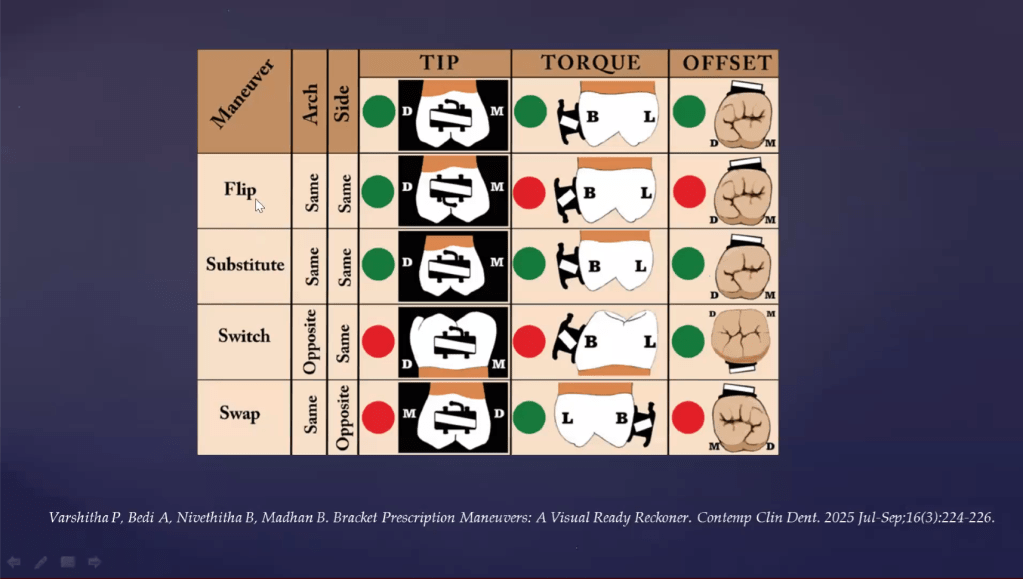
Types of Maneuvering
| Type | Description | Effect on Tip/Torque |
|---|---|---|
| Flipping | Bracket is inverted (turned upside down) on the same tooth | Changes torque (e.g., lingual crown torque → labial root torque) |
| Substituting | Bracket of one tooth placed on an adjacent/different tooth (e.g., lateral incisor bracket on canine in lateral agenesis) | No change in tip or torque — same values, just expressed on different tooth |
| Switching | Maxillary incisor bracket transferred to mandibular incisor of same side (inter-arch, same side) | Changes both tip and torque (upper vs lower tooth anatomy differs) |
| Swapping | Bracket transferred across midline within the same arch (intra-arch maneuvering) | Reverses tip direction; used in Class III camouflage |
| Blending | Combination of switching + flipping | Compound changes to tip and torque |
| Flocking | Inverting all incisor brackets of maxillary anterior segment at once | Bulk torque alteration for the anterior segment |
Clinical Applications of Maneuvering
| Clinical Situation | Maneuvering Used | Rationale |
|---|---|---|
| Lingually placed lateral incisor | Flipping (inverting bracket) | Converts lingual crown torque to labial crown torque to erupt lingual tooth |
| Lateral agenesis — canine in lateral space | Substituting (lateral bracket on canine) | Expresses lateral incisor tip/torque on canine for aesthetic finishing |
| Fixed functional appliance (e.g., Forsus) | MBT brackets on lower anteriors | Built-in lingual crown torque in MBT counteracts proclination tendency from FF appliance |
| Class III camouflage — retroclination of lower anteriors | Swapping (cross midline) | Converts mesial tip to distal tip → root moves mesially, crown tilts distally = retroclination |
| Class III with fixed functional — prevent proclination | MBT lower incisor brackets | Lingual torque of MBT resists labial tipping from functional forces |
18. CLASS III MANAGEMENT WITH BRACKET MANEUVERING
- In Class III camouflage, you want retroclination of lower incisors (crown distal, root mesial)
- When you use a swapped bracket (e.g., crossing the midline — right bracket placed on left side), the built-in mesial tip of the bracket is now expressed as distal crown tip
- Result: Lower incisor crown goes distally, root tips mesially → retroclination achieved
Similarly, in fixed functional appliance cases:
- FF appliances generate a mesial component on lower incisors → proclination risk
- By using MBT brackets on lower anteriors, the built-in lingual crown torque (negative torque) of MBT naturally counteracts the proclination tendency
19. TORQUE & TIP INTERACTION — ADDITIONAL NUANCE (MBT vs Roth)
- MBT reduced tip, increased torque — rationale:
- Reduced tip → less anchor loss from the start (no canine mesial movement in initial arch wires)
- Increased torque → compensates for roller-coaster effect
- When torque is expressed → tip is lost (wagon wheel, 4:1 ratio); by pre-loading torque, the tip loss from torque expression itself becomes the corrective force against roller-coaster
- MBT mandates retraction only on 0.019×0.025 SS in 0.022 slot to ensure all these torque values are actually expressed before and during retraction
20. FLIPPING — DETAILED MECHANISM FOR LINGUALLY PLACED LATERAL INCISOR
- Normally, MBT upper lateral has a positive torque (labial crown torque / lingual root torque)
- For a lingually placed (palatally displaced) upper lateral incisor, if you simply engage, the wire will tip the crown labially but the root may not follow correctly
- By inverting/flipping the lateral incisor bracket:
- The positive torque (lingual root torque) is reversed to labial root torque
- This drives the root labially and corrects the lingually impacted position without additional 3rd-order wire bends
RECOMMENDED READING
- Harris Khan’s Textbook on Bracket Prescription (available on ResearchGate)
- Mo Al-Mzani & Harris Khan articles on variable bracket prescription
- Andrews’ original research (1972–1989) and SWA textbook (1989)

