


B.D chaurasia 3rd Edition
B.D chaurasia 3rd Edition
Let’s know why was it introduced..
Bonding agents were introduced to improve or to create the bond between the tooth and the Restorative material.
Which was the first bonding agent ??
It’s sevriton cavity seal. It’s based on glycerophosphoric acid dimethacrylate. It had limitations like high polymerization shrinkage and high thermal expansion.
Primer + Etchants + adhesive , solvents, initiators, fillers particles and others ingredients like polyalkenoic copolymer
• Use of primer it’s to wet the surface properly or to reduce the contact angle. They maintain an expanded collagen network to allow filtration of hydrophobic monomer as well. Ex:- HEMA( Hydroxy ethyl methacrylate ) and TEGDMA ( Tri ethanol glycol dimethacrylate ).
• Conditioners are also called as Etchants. 10% Malic acid for 1 minute , and 37% phosphoric acid for 15 sec and if the concentration of phosphoric acid exceeds more than 50% then it forms monocalcium phosphate monohydrate which inhibits dissolution. Etching is done for both enamel and dentin.
• Mode of action of etchant on enamel :- by selective dissolution of enamel rods at the centre or peripheries or both. They act by increasing the surface energy and increases the surface area which creates microporosities on the surface of enamel.
• Mode of action of etchant on dentin :-It involves removal of smear layer and opening of dentinal tubules
Smear layer :- During tooth preparation the cut material along with water forms a thin film on the floor of the cavities known as smear or debris layer
Smear layer is it desirable? ?
In dentin the smear layer becomes burnished into the underlying dentinal tubules and it lowers the dentin permeability which has a protective effect.
Developing a bonding agent for enamel was easier than those of dentin, What would be the reason ?
Dentin contains water and due to inhomogeneous composition and presence smear layer will be a problem, whereas for enamel it contains more inorganic content that is calcium hydroxyapatite crystals.
• The purpose of using solvents is in order to increase the diffusion of primers and adhesive into micro retentive tooth surface and most common solvents used are ethanol and acetone.
• Adhesives in 1st generation are GPDM, 2nd generation BISGMA, TEGDMA, 3rd generation NPG- GMA,4th generation NPG-GMA, HEMA, 5th generation PENTA , Methacrylated phosphonates, 6th and 7th generation methacrylated phosphonates in water
• The etchant generally was 37% phosphoric acid almost for all generations; and primer was HEMA.
• Initial generations had all the components primer+ etchant + adhesive separately; as time progressed new generations evolved with all in one bonding agent.
• 2 step method :- 5th and 6th generation; 1 step method :- 7th generation ( all in one system )
• Indications for use of bonding agent:- When composite resin is used as Restorative material; And even when the porcelain veneers are bonded and when the exposed dentin is to be desensitized.
• Conditions that satisfy the true adhesion of Restorative material with tooth structure are sound tooth structure must be conserved; optimal retention must be achieved, microleakage should be prevented.
Reference :- Philips and Manapalil text book of dental materials
• It is coordinated and internally programmed cell death it has significance in various physiological processes like involution of thymus in early age , sculpting of tissues during development of embryo and pathological process like diseases of heart like acute MI and CNS diseases like alzehmeirs disease and parkinson’s disease
• In apoptosis single cells or small cluster of cells are involved. When compared to the normal cell the apoptotic cell has more eosinophilic cytoplasm and chromatin condensation.
• Apoptotic bodies are membrane bound spherical bodies with cell shrinkage ,chromatin condensation and eosinophilic cytoplasm. Apoptotic bodies are also referred to as Mummified bodies.
• DNA changes can be seen by gel electrophoresis by H and E stain to see the chromatin condensation and other stains. Flow cytometry for cell shrinkage.
1. Initiators of apoptosis :- Every cell has built mechanism for the cell survival and to activate the signal of cell death. Apoptosis takes place when there is withdrawal of cell survival signals like growth factors , cytokines. And the agents of cell injury like heat and radiation leads to Apoptosis
2. Initial phase of apoptosis :- There are 2 pathways by which apoptosis takes place that is intrinsic and extrinsic pathway by activating the caspases. Intrinsic pathway is the major pathway of cell death. Caspases are nothing but the protein splitting enzymes that will act on nuclear proteins and other protein components.
• Intrinsic pathway :-
• This pathway of cell death is by release of protein cytochrome C from mitochondria to cytoplasm. This triggers the cell to Apoptosis. Protein C is the life line of intact mitochondria. This is regulated by pro and anti apoptotic genes. Anti apoptotic genes are bcl2 , Mcl 1 and bcl x. Pro apoptotic genes are bid , bad. The proapoptotic genes will trigger apoptosis that will release Bak and Bax that will damage the mitochondrial membrane and releases the cytochrome c from mitochondria to cytoplasm that will activate caspases
• Extrinsic pathway :-
• This pathway of cell death is by activation of cell death receptors present on the cell surface. Cell death receptor tumour necrosis factor and related transmembrane protein that is fas and it’s ligand fas l this binding is associated with Fas associated death domain. This will activate caspases
3. Final phase of apoptosis :- There is activation of caspases 8 by intrinsic pathway and caspases 9 and 10 by extrinsic pathway that will act on the nuclear proteins and this leads to the changes in the DNA and cell death.
4. Phagocytosis :- The surface of the cell will undergo changes in order to activate the adjacent macrophages for its phagocytosis. Phosphatidyl serine and thrombospondin molecules is present inside, during apoptosis it comes to the exterior that triggers the cell for its phagocytosis. Phagocytosis is rapid and it’s not accompanied by inflammatory cells.
Reference :- Harsh Mohan
Clinical steps in complete denture fabrication :-
• Diagnosis and treatment planning
• Mouth preparation
• Tray selection
• Primary impression
• Border moulding
• Secondary impression
• Jaw relations
• Teeth selection
• Try in
• Denture delivery
Laboratory steps in complete denture fabrication :-
• Primary cast
• Spacer
• Special tray
• Secondary cast
• Denture base
• Occlusal rims
• Articulation
• Teeth arrangement
• Dearticulation
• Flasking
• Packing
• Curing
• Deflasking
• Finishing and polishing

1️⃣ According to Anatomical Site –
2️⃣ According to rate of caries progression –
3️⃣ According to nature of attack-
4️⃣ Based on chronology –
https://dentowesome.wordpress.com/2020/05/11/pit-fissure-caries/
https://dentowesome.wordpress.com/2020/05/07/dental-caries/
Sudden, rapid & almost uncontrolled destruction of teeth affecting surface that are relatively caries free.
Affect deciduous teeth due to prolonged use of nursing bottle containing milk, sugar or honey.
💬 What is 👶 bottle decay? What causes it and how to prevent it? 👇🏻
Dentowesome|@drmehnaz🖊
Image Source: Google.com
Ridge = Soft tissue + bone
• Residual ridge resorption is a life long process. Residual ridge resorption is maximum upto 3 to 6 months and after that it tappers off.
Alveolar bone :- defined as a bony portion of maxilla and mandible held by the fibres of PDL.
Depending on the type of bone the resorption pattern varies like for spongy bone replaced 3-4 yrs and compact bone replaced 10yrs
Which is the process coupled that is bone deposition by osteoblast and bone resorption by osteoclast.
• Residual ridge resorption pattern varies in different individual
According to American college of prosthodontics
Based on bone ht
Type 1 :- residual bone height 21 mm
Type 2 :- residual bone height 16mm
Type 3:- residual bone height 11 – 13mm
Type 4 :- residual bone height 10mm
Type 1 is having good prognosis and type 4 is having poor prognosis that means it’s difficult to gain stability , retention and support
Epidemiology of residual ridge resorption
•It occurs world wide . RRR is accelerated in 1st 6 months with more loss in mandible than maxilla.
• After menopause that is due to harmonal disturbances osteoblastic activity is very less and it’s dominated by osteoclastic activity
” RESORPTION OF MANDIBLE >>>> RESORPTION OF MAXILLA
Direction of bone resorption :-
• Maxilla resorbs upwards and inwards ( centripetal) to become progressively small
• Mandible resorbs outwards and progressively wider
Etiology of residual ridge resorption :-
• Anatomical factors that is quality and quantity of bone of residual ridge RRR is directly proportional to anatomical factors
• Metabolic process :- RRR is directly proportional to bone resorption factors and inversely proportional to formation factors
• Mechanical factors :- If there is excess stimulus or no stimulus resorption takes place
Consequences of residual ridge resorption :-
– loss of sulcus width and depth
– Displacement of muscle attachment to the ridge
– loss of vertical dimension of occlusion. Reduction of lower facial height
– Increase in relative prognathism. Changes in inter alveolar relation. Change in the location of mental foramen.
Treatment :-
– Prevention of loss of natural tooth. Change in the design of denture like impression technique by using minimal pressure impression and selective pressure impression techniques.
• Provide adequate relief on relief are areas. Avoidance of inclined planes. Centralization of occlusal contacts to increase stability and maximise compressive forces
• Adequate interocclusal distance that is by providing enough free way space . Occlusal table should be narrow .
Source :- Deepak nallaswamy and rangarajan.

The only weapon with which the unconscious patient can immediately retaliate upon the incompetent surgeon is hemorrhage -William S Halsted.
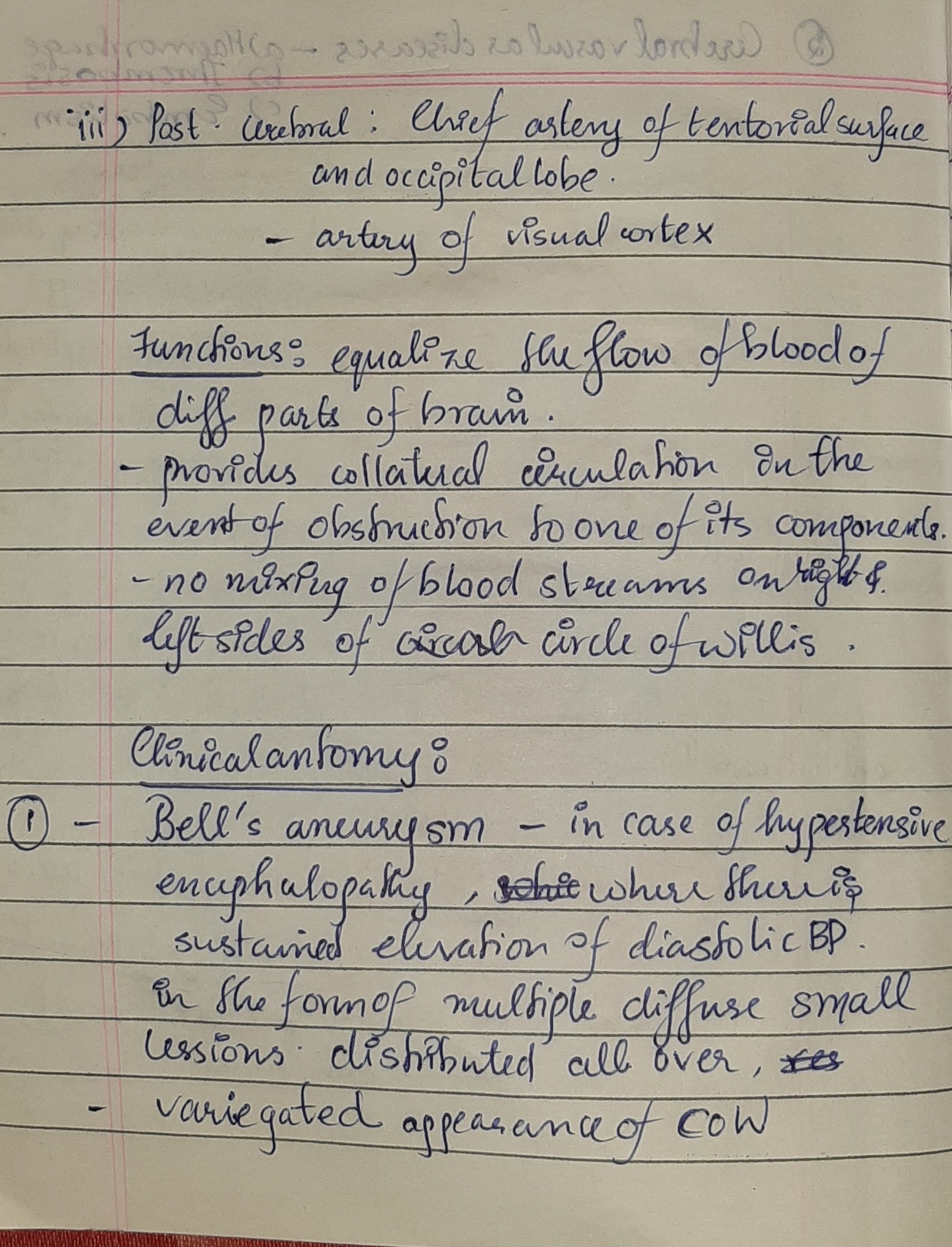
Also known as loop of Willis,Willis polygon and cerebral arterial circle.
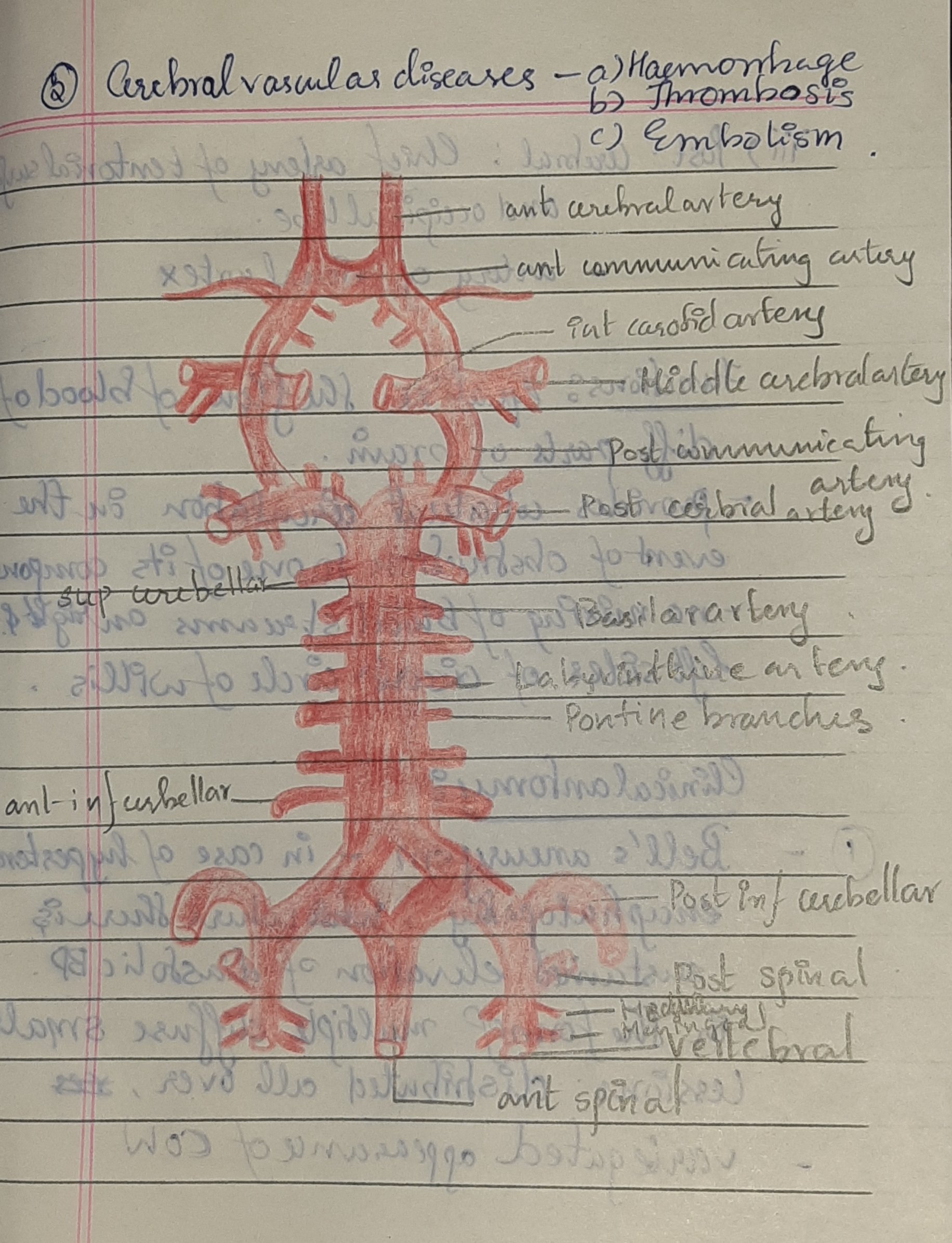
Blood vessels supplying the brain consists of 2 separate vascular systems:
In the base of the brain both systems are connected bilaterally by posterior communicating arteries and left to right side by anterior communicating arteries forming the “Circle of Willis”(COW).

 Other key points:
Other key points:
Mnemonics:
Cell is Clearly Circulating
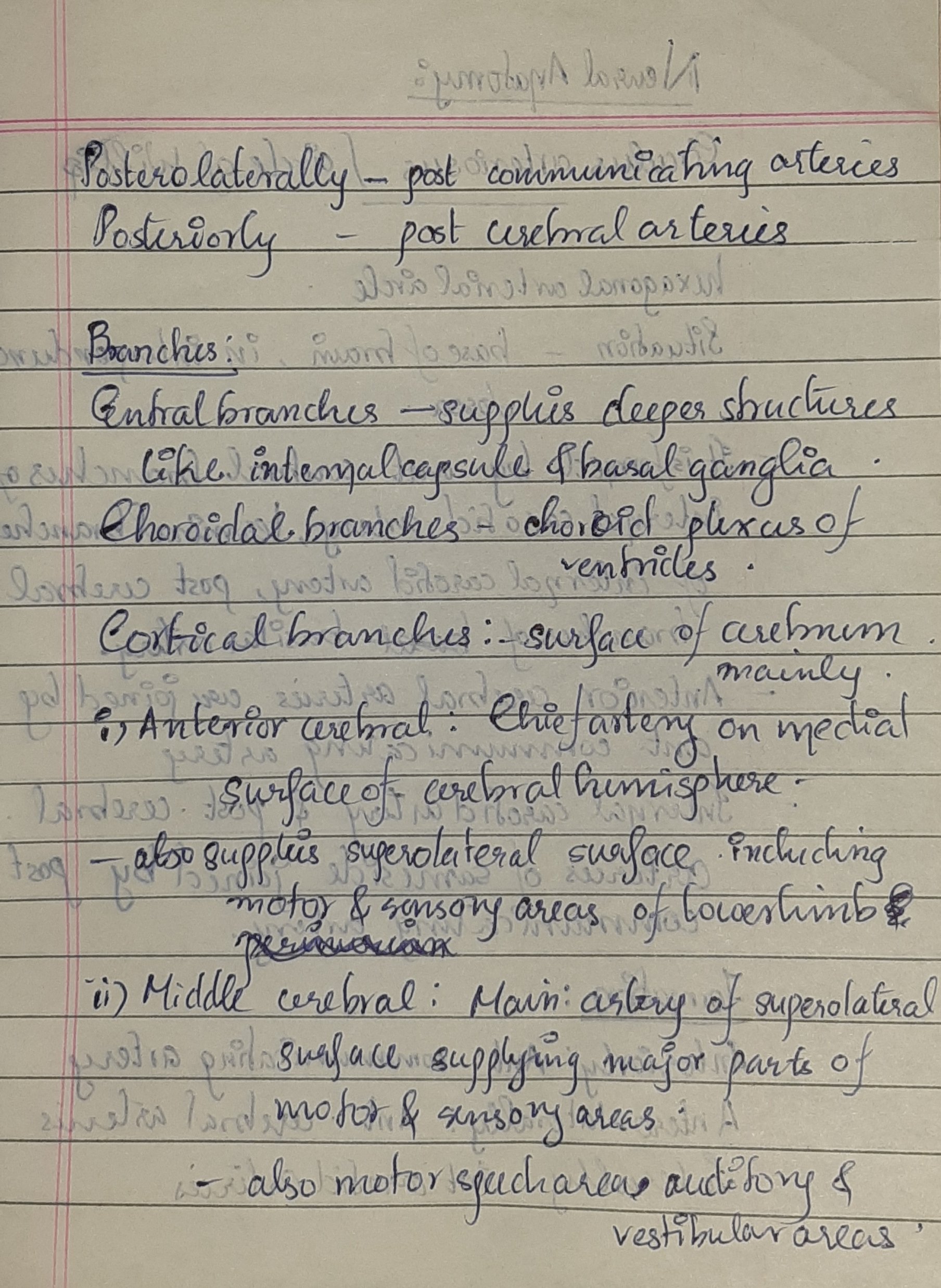
C-Cortical branches
C-Central branches
C-Choroidal branches
Sources: BD Chaurasia’s Human anatomy 7th edition-volume 4
Slideshare.net -Circle of Willis by Luiz Roberto Meier Update 2
Reference:Nikhil Marwah image from book only

Antibiotics can be divided into 2 classes based on their mechanism of action:-
➡️ Bactericidal antibiotics kill bacteria by inhibiting cell wall synthesis. Example:
➡️ Bacteriostatic antibiotics limit the growth of bacteria by interfering with bacterial protein production, DNA replication or other aspects of bacterial cellular metabolism.
They must work together with immune system to remove the micro-organisms from the body. Example:
Note that while it is rational to favor bactericidal agents over bacteriostatic agents, neither has ever been shown to be superior (probably because true recovery from infection cannot occur until the body is able to mount an appropriate immune response, thus “buying time” may be just as good as active killing)
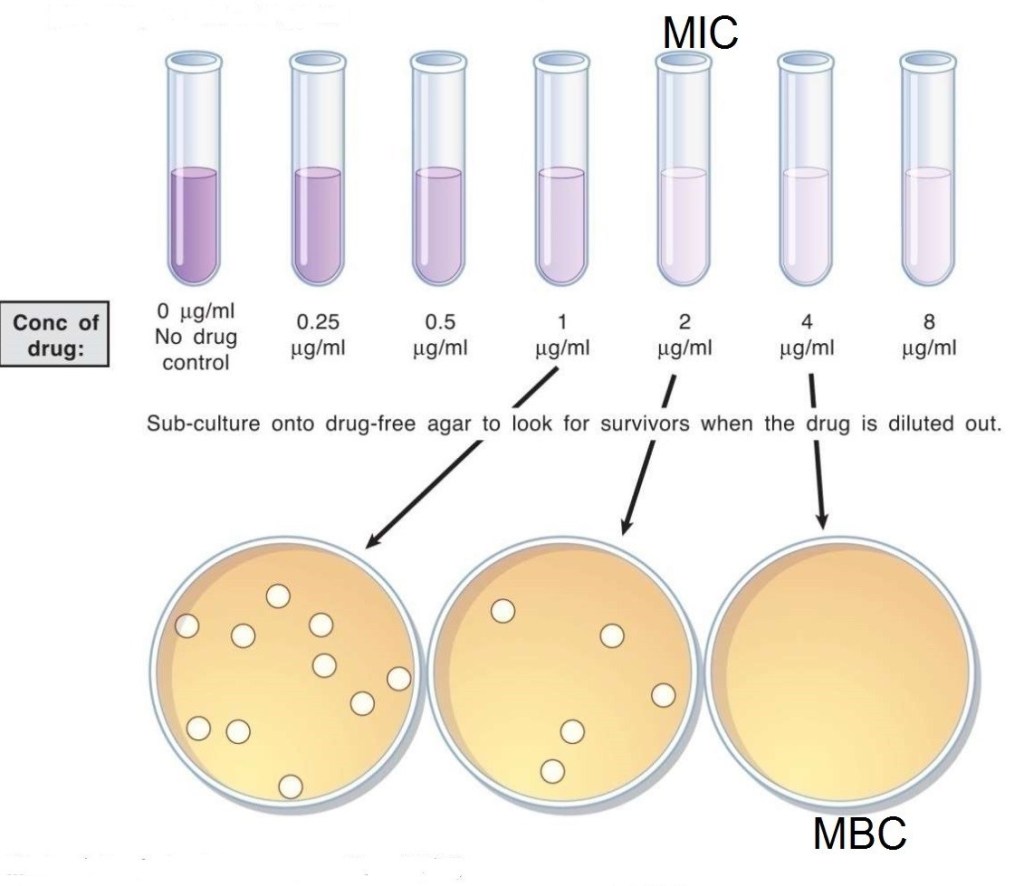
➡️ The MBC is the minimum concentration of drug which can kill the micro-organisms.
➡️ The MIC is the minimum concentration of drug which can inhibit the growth of micro-organisms.
Council for Appropriate and Rational Antibiotic Therapy (CARAT) criteria for accurate use of antibiotic therapy
● Evidence-based results ●Therapeutic benefits
● Safety
● Cost-effectiveness
● Optimal drug dose and duration —Shorter-course, more aggressive therapy
(i) Evidence-based results:
In choosing an antibiotic, clinicians should consider the clinical evidence demonstrating that the drug is clinically and microbiologically appropriate, the efficacy of that drug in well-designed clinical trials, and the antibiotic resistance patterns of the local region. Clinicians should then use their professional judgment to choose the optimal antibiotic.
(ii) Therapeutic benefits:
If possible, the clinician should identify the causative pathogen and use surveillance data on regional antibiotic resistance patterns in selecting the optimal therapeutic agent.
(iii) Safety:
In treating patients with a particular drug, safety must be weighed against efficacy. Clinically applicable treatment strategies should be chosen to maximize efficacy while minimizing side effects.
(iv) Optimal drug for optimal duration:
Optimal drug selection requires finding the antimicrobial class and the specific member of that class that is best suited to treat a particular infection. Because empiric therapy is necessary in most cases, multiple factors have to be considered. Among these are whether the etiologic agent is likely to be gram-positive or gram-negative, whether a narrow or broad-spectrum agent should be chosen, the resistance patterns of the likely pathogen to this drug, both nationally and regionally, and the individual patient’s medical history, including recent antibiotic exposure.
Optimal duration means prescribing the selected drug for the shortest amount of time required for clinical and micro- biologic efficacy. There are many reasons for reducing an- timicrobial therapy to the shortest appropriate duration. They include the potential for reduced occurrence of adverse effects, increased patient adherence, decreased promotion of resistance, and decreased costs.
(v) Cost-effectiveness:
Choosing inappropriate therapy is associated with increased costs, including the cost of the antibiotic and increases in overall costs of medical care because of treatment failures and adverse events.
Dentowesome | @drmehnaz🖊
References:
Thermal properties
The arrangement of atoms and molecules in materials is influenced by the temperature; as a result, thermal techniques are important in understanding the properties of dental materials
Thermal conductivity : thermal conductivity of a substance is the quantity of heat in calories or joules per second passing through a body 1cm thick with a cross section of 1 sq.cm when the temperature difference is 1°C.
Eg – a large amalgam filling or gold crown in proximity to the pulp may cause the patient discomfort when hot or cold foods produce temperature changes, this effect is mitigated when adequate tooth tissue remains or cavity liners are placed between the tooth and filling for insulation.
Specific heat : specific heat of a substance is the quantity of heat needed to raise the temperature of 1g of the substance by 1°C.
Eg – during the melting and casting process, the specific heat of the metal or alloy is important because of the total amount of heat that must be applied to the mass to raise the temperature to the melting point.
Thermal diffusivity : it is a measure of transient heat flow and is defined as the thermal conductivity, divided by the product of the specific heat, times the density.
Eg- for a gold crown or a dental amalgam, the low specific heat combined with the high thermal conductivity creates a thermal shock more readily than normal tooth structure does.
Coefficient of thermal expansion : the change in length per unit length of a material for a 1°C change in temperature is called the linear coefficient of thermal expansion.
Although the coefficient is a material constant, it doesn’t remain constant over wide temperature ranges. For eg, the linear coefficient of thermal expansion of a dental wax may be an average value of 300×10-6/°C upto 40°C, whereas it may have an average value of 500×10-6/°C from 40-50°C.
The coefficient of thermal expansion of a polymer changes as the polymer goes from a glassy state to a softer, rubbery material. This change in the coefficient corresponds to the glass transition temperature.
It is obvious that with the reduction in temperature, there is a contraction of a substance as much as of expansion tht occured during heating. Accordingly, tooth structure and restortive materials expand when warmed by hot food or beverages and contract when exposed to cold substances. Such expansions and contractions may break the marginal seal of a filling in tooth particularly when the difference between coefficient of thermal expansion of tooth and restorative material is too large.
Electrical properties
The ability of a material to conduct an electric current may be stated as conductivity or conversely as the specific resistance or resistivity. The conductivity by materials used to replace tooth tissues is of concern in restorative dentistry.
Dielectric constant : a material that provides electrical insulation is known as dielectric. The dielectric constant of a dental cement generally decreases as the material hardens. This decrease reflects a change from a paste that is relatively ionic and polar to one that is less.
Electromotive force : the electromotive series is a listing of electrode potentials of metals according to the order of their decreasing tendency to oxidise in solution. Those metals with a large negative electrode potential are more resistant to tarnish than those with a high positive electrode potential.
Galvanism : the presence of metallic restorations in the mouth may cause a phenomenon called galvnic action where saliva or bone fluids like electrolytes make up an electric cell.
Corrosion : the corrosion of gamma, gamma 1, gamma 2 phases in amalgam has been studied by electrochemical analysis. The dental amalgam specimens become pitted at the boundaries between the phases or in gamma 2 phase. The addition of copper to amalgam alloys to form copper-tin compounds during hardening has improved the resistance of amalgam to chloride and galvanic corrosion.
Tarnish : the process of steam sterilization of surgical instruments has long presented a serious problem of tenish and corrosion. Many non metallic materials such as cements and composites have shown a tendency to discolor in service because the colored substances penetrate the materials and continue chemical reactions in the composites.
Source : Craig’s textbook of restorative materials
