🎤 “So here’s the thing — most people pick a career because their parents told them to, or because they panicked after Class 12. But Dr. Akansha Kashyap? Nope. She picked dentistry like it was a love affair between science and art — and guess what? She got the gold medal to prove it. 🏅✨
She’s the kind of dentist who can fix your smile in the morning and sell you a handmade art piece in the evening. Honestly, if she wasn’t drilling cavities, she’d probably be designing album covers. 🎨🦷
In this interview, she spills about: 💡 How to juggle academics without losing your mind (or your hobbies) 🌟 Why mentors + creativity = survival kit in dentistry 🖊️ And a piece of advice so good, you’ll want to embroider it on your scrubs.
So… why are you still here? Go read the full interview — it’s like fluoride for your brain. 🧠💎
In this issue, Oral Pathologist Dr. Shivani Bhandari opens up about her inspiring path—from the first spark of ambition in her school days to navigating academic pressure, personal loss, and carving her own niche in the dental world.
💡 You’ll find:
Honest stories of resilience and motivation when life tests you the hardest.
Practical advice on balancing studies, hobbies, and responsibilities.
A refreshing reminder that dentistry is more than a profession—it’s a platform to innovate, teach, create, and inspire.
If you’re a dental student or young professional, this magazine isn’t just for reading—it’s for redefining what your future could look like.
👉 Dive in. Get inspired. Start shaping your own unique path in dentistry.
Hey future orthodontists! 👋 Ready to dive deep into one of the most fascinating pieces of research in functional orthodontics? Today we’re breaking down Voudouris et al.’s groundbreaking study on condyle-fossa modifications during Herbst treatment. This isn’t just another research paper – it’s a paradigm shift that changes how we understand functional appliances!
Why This Research Matters 🎯
For decades, we’ve been taught that functional appliances work through lateral pterygoid muscle hyperactivity. But what if that’s completely wrong? This study flips the script and introduces the revolutionary Growth Relativity Theory.
Study Overview 📊
Study Component
Details
Sample Size
56 subjects total
Primate Subjects
15 cynomolgus monkeys (Macaca fascicularis)
Human Subjects
17 Herbst patients + 24 controls
Key Focus
8 juvenile primates (24-36 months)
Treatment Duration
6, 12, and 18 weeks
Activation Amount
4-8mm progressive advancement
The Revolutionary Methodology 🔬
What made this study special? Three cutting-edge techniques that previous research lacked:
1. Permanent EMG Electrodes 📡
Old method: Temporary, transcutaneous electrodes
New method: Surgically implanted permanent electrodes
Muscles monitored: Superior and inferior lateral pterygoid, masseter, anterior digastric
2. Tetracycline Vital Staining 💡
Intravenous tetracycline injection every 6 weeks
Fluorescence microscopy with UV light
Result: Crystal-clear visualization of new bone formation
3. Computerized Histomorphometry 🖥️
Quantitative analysis of bone formation
Measured area and thickness of new bone
Statistical validation of results
The Shocking Results That Changed Everything 😱
What Everyone Expected vs. What Actually Happened
Traditional Theory
Actual Findings
⬆️ Lateral pterygoid hyperactivity
⬇️ DECREASED muscle activity
Muscle-driven growth
Viscoelastic tissue-driven growth
Unpredictable results
Consistent, reproducible changes
Key Findings Summary 📈
Super Class I Malocclusion Development: All experimental subjects developed severe Class I relationships
Glenoid Fossa Remodeling: Forward and downward growth (opposite to natural backward growth)
Condylar Growth Enhancement: Increased mandibular length in all subjects
Muscle Activity Paradox: Growth occurred with DECREASED EMG activity
The Growth Relativity Theory Explained 🧠
Think of it like this: Imagine the retrodiskal tissues as a giant elastic band 🎸 stretched between the condyle and fossa.
Patient: 14-year-old with severe Class II, mandibular retrognathism Traditional thinking: “The Herbst will make the lateral pterygoid muscles work harder to grow the condyle” Reality: The Herbst creates reciprocal stretch forces that stimulate bone formation through mechanical transduction, not muscle hyperactivity!
Treatment Contributions Breakdown 📊
The researchers found that achieving a 7mm change along the occlusal plane involved multiple factors:
Vertical distraction of condyle from articular eminence
Prevents condylar resorption
Avoids TMJ compression
Optimizes stretch forces on retrodiskal tissues
Treatment Timeline and Bone Formation 📅
Progressive Changes Over Time
Time Point
Bone Formation Area
Key Observations
6 weeks
Early changes
Extensive cartilage proliferation
12 weeks
1.2mm average
Peak bone formation rate
18 weeks
Maximum response
Doubled postglenoid spine thickness
Correlation: r = 0.95 between treatment time and bone formation! 📈
Clinical Decision-Making Flowchart 🗺️
Class II Patient Evaluation ↓ Age Assessment ↓ ┌─────────┴─────────┐ ↓ ↓ Mixed Dentition Permanent Dentition ↓ ↓ Herbst with Consider Herbst vs Occlusal Coverage Alternative Treatment ↓ ↓ Continuous Monitor for: Activation - Condylar resorption 1-2mm every - Disk displacement 10-15 days - Relapse potential
Key Clinical Takeaways for Practice 💡
Do’s and Don’ts
✅ DO
❌ DON’T
Use continuous activation
Rely on intermittent wear
Include occlusal coverage
Ignore vertical dimension
Monitor for 6+ months
Expect immediate results
Plan retention carefully
Assume permanent changes
Red Flags to Watch For 🚩
Condylar resorption – prevented by proper vertical dimension
TMJ pain – indicates excessive compression
Rapid relapse – inadequate retention period
Disk displacement – poor appliance design
The Retention Challenge 🔄
Critical Finding: Without adequate retention, positive condyle-fossa changes can relapse due to:
Return of anterior digastric muscle function
Perimandibular connective tissue pull
Natural tendency for condyle to seat posteriorly
Retention Protocol Recommendations:
Minimum 6 months active retention
Progressive reduction of appliance wear
Monitor muscle reattachment process
Long-term follow-up essential
Clinical Scenario Application 🎯
Case: 13-year-old female, Class II Division 1, severe mandibular retrognathism
Treatment Plan Based on Research:
Herbst with occlusal coverage (NOT standard Herbst)
Progressive activation 1.5mm every 2 weeks
12-week minimum treatment duration
Expect 70% orthopedic response
Plan extended retention phase
Expected Outcomes:
Forward fossa remodeling
Increased mandibular length
Super Class I result requiring finishing
Need for comprehensive retention protocol
Future Implications 🔮
This research suggests that functional appliances should be renamed “dentofacial orthopedic appliances” because they work through:
Viscoelastic tissue forces
Mechanical transduction
Growth modification, NOT muscle function
Study Limitations and Considerations ⚖️
Strengths:
Rigorous methodology with multiple validation techniques
Control groups and statistical analysis
Novel technological approaches
Limitations:
Animal model – translation to humans requires validation
Small sample size – justified but limits generalizability
This groundbreaking research fundamentally changes how we understand functional appliances. The key shifts in thinking:
From muscle hyperactivity → To tissue stretch forces
From unpredictable results → To consistent orthopedic changes
From simple tooth movement → To complex TMJ remodeling
From empirical treatment → To evidence-based protocols
Memory Aid for Boards 📚
“VOUDOURIS RULES” 🧠
Viscoelastic forces drive change
Occlusal coverage prevents resorption
Undermining old muscle theories
Decreased EMG activity during growth
Orthopedic effects dominate (70%)
Underaged patients respond best
Retention critical for stability
Inferior-anterior fossa growth
Super Class I results expected
Questions for Self-Assessment 🤔
What percentage of Herbst treatment effects are orthopedic vs orthodontic?
Why does EMG activity decrease during successful treatment?
What prevents condylar resorption in Herbst appliances?
At what age is condylar growth potential highest?
What is the Growth Relativity Theory?
Remember: This research doesn’t just change what we know about Herbst appliances – it revolutionizes our understanding of functional orthodontics entirely! 🚀
Keep studying, future orthodontists! The field is constantly evolving, and staying current with research like this will make you better clinicians. 📖✨
Welcome to an exciting exploration of one of the most innovative modifications in functional orthodontics! As orthodontic students, mastering the nuances of appliance design and modification is crucial for your future success. Today, we’re diving deep into the groundbreaking Twin Block advancement modification developed by Carmichael, Banks, and Chadwick – a system that has transformed how we approach Class II treatment with enhanced precision and patient comfort.
🎯 Why This Modification Matters for Your Future Practice
The Twin Block appliance, introduced by Clark in 1982, has become one of the most popular functional appliances in the United Kingdom and is arguably the most successful in treating Class II division 1 malocclusions. However, the original design had significant limitations that this modification brilliantly addresses.
The Problem with Traditional Twin Block Reactivation 🚫
Inconvenient chairside acrylic additions
Unpleasant taste and smell for patients
Inaccuracy due to polymerization shrinkage
Time-consuming laboratory modifications
Limited ability to make small, gradual adjustments
Understanding the Core Principle
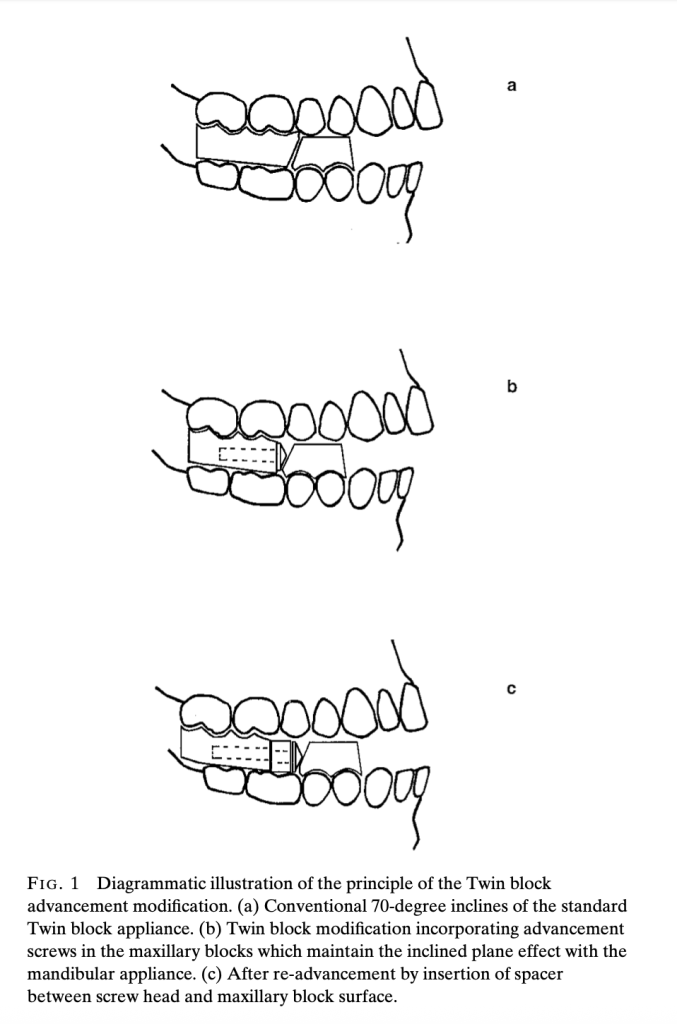
The modification incorporates stainless steel screws with conical heads into the upper appliance blocks, maintaining the crucial 70-degree inclined plane effect regardless of screw rotation. This ingenious design allows for controlled, measurable advancement using polyacetal spacers.
Technical Specifications: What You Need to Know
Component
Specification
Clinical Purpose
Stainless Steel Screws
3mm diameter, 18/8 M3 grade
Provide structural strength and stability
Screw140° included angle (70° working angle)
Maintain 70° inclined plane regardless of rotation
Screw Lengths
12mm and 16mm (longer for >5mm advancement)
Accommodate various advancement needs
Spacers Material
Polyacetal co-polymer resin
Enable precise, measurable advancement
Spacer Lengths
1mm, 2mm, 3mm, 4mm, 5mm
Allow stepwise progression (2-3mm typical)
Spacer Diameter
6mm diameter
Ensure proper fit and function
Thread Housing
Injection-molded acetal resin with lateral tags
Prevent fractures and ensure consistent fit
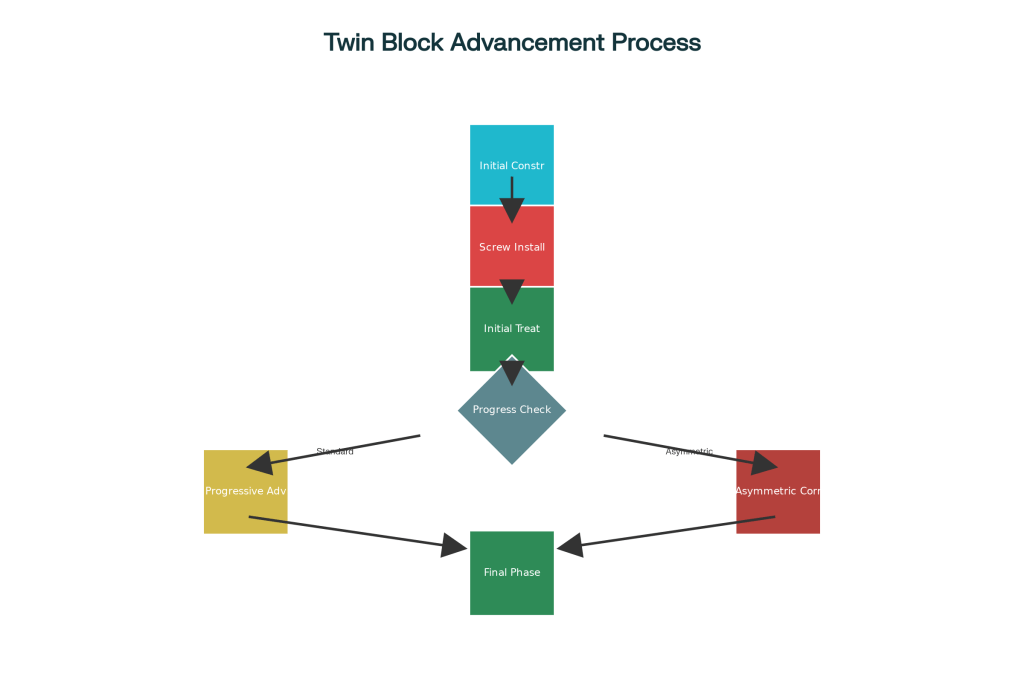
The treatment process follows a logical, patient-friendly progression that maximizes compliance and comfort while achieving optimal results.
Phase 1: Initial Construction and Setup
Bite Registration: Take protrusive wax bite with comfortable advancement (may be as little as 2-3mm in some patients)
Screw Installation: Insert 3mm diameter stainless steel screws with 140° conical heads into upper blocks
Initial Delivery: Begin treatment with screws inserted without any spacers
Phase 2: Progressive Advancement
Monitoring: Assess overjet reduction at each visit
Advancement: Add 1-5mm polyacetal spacers between screw heads and blocks
Typical Increments: 2-3mm per advancement visit
Maximum Advancement: Up to 9mm using longer 16mm screws
🎭 Clinical Scenarios: Real-World Applications
Scenario 1: The Dolichofacial Challenge 😰
Patient: 12-year-old female with long face pattern
Challenge: Weak craniomandibular musculature, poor tolerance for large protrusions
Traditional Problem: Patient bites blocks together instead of maintaining protrusive position
Modified Solution: Start with minimal 2mm advancement, progress gradually with 1-2mm spacers
Outcome: Improved compliance and comfort, successful Class II correction
Scenario 2: The Large Overjet Case 📏
Patient: 13-year-old male with 12mm overjet
Challenge: Requires significant mandibular advancement but limited initial tolerance
Traditional Problem: Would require multiple appliance remakes or uncomfortable large advances
Modified Solution: Begin with comfortable 3mm advancement, systematically add spacers over 6 months
Outcome: Achieved 9mm total advancement with excellent patient acceptance
Scenario 3: The Asymmetric Correction 🎯
Patient: 11-year-old with Class II and dental centerline deviation
Challenge: Need for different advancement amounts on each side
Traditional Problem: Difficult to achieve asymmetric correction with conventional methods
Modified Solution: Use different spacer lengths – 3mm right side, 5mm left side
Outcome: Successful centerline correction along with Class II improvement
Scenario 4: The Class III Application 🔄
Patient: 10-year-old with developing Class III malocclusion
Challenge: Requires gradual reactivation for optimal growth modification
Modified Solution: Incorporate screws into maxillary appliance for controlled reactivation
Advantage: Small increments reduce patient discomfort and improve compliance
🎨 Material Science: Understanding Polyacetal Resin
Why Polyacetal is Perfect for This Application:
Strength: 10 times stronger than conventional acrylic resin
Safety: Non-toxic and non-allergenic properties
Durability: High resistance to surface wear and low water absorption
Workability: Can be trimmed and polished with standard dental instruments
Biocompatibility: Proven safe for intraoral use over extended periods
Less tolerance for large protrusions, gradual advancement essential
Start with 2-3mm advancement, progress gradually
Brachyfacial (Short Face)
Deep overbites present
Overbite reduction more problematic due to reduced block trimming
Use Phase 1 appliance or plan fixed appliances to follow
Mesofacial (Average)
Balanced growth pattern
Standard advancement protocol works well
Standard 2-3mm increments per visit
Class III Cases
Requires gradual reactivation
Small increments of reactivation necessary
Utilize modification for controlled gradual advancement
💡 Clinical Tips for Success
For Dolichofacial Patients 📐
Start conservatively with minimal advancement
Monitor for tendency to bite blocks together
Consider Phase 1 appliance for overbite reduction
Emphasize proper appliance positioning during sleep
For Brachyfacial Patients 🔽
Plan for overbite management strategies:
Option 1: Use initial upper removable appliance (Phase 1)
Option 2: Gradual Twin Block wear reduction during retention
Option 3: Upper removable retainer with anterior inclined bite plane
General Clinical Guidelines 📋
Advancement Frequency: Every 3-4 weeks based on patient adaptation
Typical Increments: 2-3mm spacers for most patients
Maximum Achievement: Up to 9mm total advancement reported
Block Height Requirement: Minimum 6mm between second premolars
⚠️ Troubleshooting Common Issues
Problem: Block Cracking After Advancement 🔧
Cause: Inadequate block height or retrospective screw insertion Prevention: Ensure adequate 6mm block height, incorporate screws during initial construction Solution: Use screw thread housing system for reinforcement
Problem: Difficulty Removing Screws 🔄
Cause: Direct screw insertion into acrylic creating tight fit Solution: Use screw thread housing to facilitate easy removal and adjustment
Problem: Screw Alignment Issues 📏
Cause: Manual positioning without proper guides Solution: Use alignment rods during construction for precise positioning
📍Scene: Department of Orthodontics, South India You’re sipping your 4th cup of filter kaapi ☕, scrolling through cephs, and bam! You spot that patient who walks in looking like they’re always mid-pout. Not because they’re annoyed – but because their upper and lower jaws are both chillin’ way ahead of where they’re supposed to be!
Say hello to the one and only: 💥 Bimaxillary Prognathism (BP)! 💥
🧠 First, What’s the Problem in BP?
Teeth: Proclined upper/lower incisors
Bone: Bony base might be normal or slightly prognathic
Profile: Convex, often with a shallow mentolabial sulcus
Patient Goal: Most patients want facial esthetics, not just dental alignment.
✅ Orthodontic Treatment (OT): When is it Enough?
🦷 Recommend OT when:
Feature
What to Look For
Why It Works
Skeletal
Skeletal Class I or mild Class II
Easy to camouflage with incisor retraction
Vertical Pattern
Normodivergent or mild open bite
Not too much vertical correction needed
Dental
Proclined and protrusive incisors (U1-NA > 7 mm, IIA < 115°)
Can retract and upright teeth
Chin
Moderate Pog-NB or prominent chin
Profile will improve with incisor retraction
Soft Tissue
Mild lip strain, acute NLA, small interlabial gap
Incisor retraction improves esthetics
Age
Adolescents or young adults
Bone remodeling is more effective
🔬 Clinical Clue: If the patient shows good incisor protrusion, decent chin, and minimal vertical discrepancy, OT alone (with 4 premolar extraction and maximum anchorage like TADs) is effective.
BUT WAIT! 😬 It’s not all rose petals and retraction:
😨 Root resorption
🌀 Over-tipping the incisors (like they’re diving into the lingual pool)
😳 Too much upper incisor show = accidental rabbit cosplay 🐰
🚀 New tech to the rescue:
Miniscrews = anchorage champs 💪🏽
Torque control = no flaring disasters
Rapid ortho techniques = get that smile faster! 🏎️💨
But still… sometimes, it’s just not enough.
🛠️ Anterior Segmental Osteotomy (ASO): When is It Needed?
🧱 Recommend ASO when:
Feature
What to Look For
Why OT Fails
Skeletal
Skeletal Class II with mandibular deficiency
Can’t fix jaw position with braces
Vertical Pattern
Hyperdivergent, steep SN-GoMe, open bite tendency
Difficult to close lip or rotate chin
Dental
Incisors upright or not protrusive (U1-NA < 5 mm, IIA > 120°)
Not enough room to retract teeth
Chin
Retrusive chin (low Pog-NB)
Profile won’t improve without surgery
Soft Tissue
Large interlabial gap, obtuse nasolabial angle
Lip strain and eversion won’t resolve
Age
Adults > 25 yrs, with high esthetic demand
Faster and more definitive solution
🔬 Clinical Clue: If the incisors are already upright but the face still looks full/lips strained, you can’t “retract” anymore — go for ASO.
👎🏽 But, ASO comes with a long list of side dishes (a.k.a. complications):
🦷 Root cutting (Poor canine gets the axe 😢)
🧊 Temporary lower lip numbness
🦴 Wound healing issues
🦷 Necrosis or ankylosis if you’re not careful
🧩 Occlusion mess – especially around canines and premolars
⚠️ Often, post-ASO ortho is still needed to fine-tun
🔍 The Big Question: OT or ASO? 🤔
You can’t just toss a coin! The decision depends on:
Skeletal pattern
Soft tissue thickness
Degree of dentoalveolar protrusion
Chin position
Patient expectations (a.k.a. “I want to look like my fav actor” syndrome 🎥)
📈 Discriminant Analysis = Your Clinical GPS 📍
To make life easier, the researchers did stepwise discriminant analysis to find THE SEVEN COMMANDMENTS (ahem… key variables) that can predict who should get OT vs. ASO:
No.
Variable
Meaning
1️⃣
IIA (°)
Interincisal Angle
2️⃣
U1-NA (mm)
Upper incisor to NA distance
3️⃣
CF (°)
Craniofacial angle (skeletal volume idea)
4️⃣
Interlabial gap (mm)
Resting mouth opening
5️⃣
Lower NLA (°)
Lower nasolabial angle
6️⃣
Ptm-N (mm)
Posterior maxillary length
7️⃣
PNS-ANS (mm)
Anterior maxillary length
👩⚕️ Let’s Apply: Clinical Scenarios
🩺 Scenario 1: OT is Ideal
25-year-old female
U1-NA = 9 mm, IIA = 110°
CF = 155°, Pog-NB = +1.5 mm
Lower NLA = 61°
Interlabial gap = 1.5 mm
✅ Go with OT
Great incisor proclination
Good chin projection
Lips will improve with retraction
No skeletal Class II red flags
🩺 Scenario 2: ASO Recommended
28-year-old female
U1-NA = 4.5 mm, IIA = 120°
CF = 150°, Pog-NB = -1 mm
Lower NLA = 70°
Interlabial gap = 3.2 mm
✅ Go with ASO
Incisors already upright — nothing more to retract
Receded chin, large gap → lip incompetence won’t fix with OT
More obtuse NLA = lip eversion
🩺 Scenario 3: Neither OT Nor ASO Alone Is Sufficient
30-year-old male
Severe skeletal Class II
SNB = 74°, CF = 145°
Pog-NB = –4 mm, IIA = 123°
Large interlabial gap
❌ OT will fail ❌ ASO alone won’t help
🟢 Best: Two-jaw surgery (maxillary ASO + mandibular advancement) — To correct both jaw position and dental alignment.
🛠️ Simplified Decision Rule (Mnemonic Style)
“OT IF the teeth are the issue, ASO IF the face is the issue.”
🦷 Teeth protrusive, chin okay → OT
👄 Face convex, lip strain, chin poor → ASO
🦴 Jaw discrepancy → Consider Two-jaw Surgery
CLINICAL BASED MCQS
1. A 23-year-old female presents with lip incompetence, protrusive incisors, and Class I molar relationship. Cephalometric values show IIA = 118°, U1-NA = 7 mm, Ptm-N = 45 mm, and CF = 5°. What is the most appropriate initial treatment approach?
A. Begin OT with maximum anchorage B. Consider ASO followed by OT C. Non-extraction OT with miniscrew support D. Two-jaw surgery with setback of mandible
✅ Answer: B Explanation: IIA < 120°, U1-NA is high, and Ptm-N is short with low CF, favoring poor response to OT alone—ASO is indicated.
2. In a borderline BP case with normal upper incisor inclination, low interlabial gap, and skeletal Class I tendency, which factor would most strongly tip the decision toward OT rather than ASO?
A. Presence of shallow mentolabial sulcus B. Reduced NLA C. Short posterior facial height D. Smaller Ptm-N and normal U1-NA
✅ Answer: D Explanation: If upper incisors are not overly protrusive and soft tissue strain is minimal, OT alone may be sufficient.
3. A patient treated with OT showed flat profile, reduced upper lip protrusion, but residual lip incompetence and an obtuse lower nasolabial angle. What was likely missed in the pre-treatment assessment?
A. Overjet measurement B. Posterior maxillary depth C. Interlabial gap evaluation D. Chin projection assessment (Pog-NB)
✅ Answer: D Explanation: A recessed chin (low Pog-NB) can lead to persistent lip strain even after dental retraction. Skeletal correction might have been more suitable.
4. Which combination of cephalometric changes at T0 is most predictive of failure with OT but success with ASO ?
A. IIA = 130°, U1 exposure = 3 mm, CF = 6° B. U1-NA = 10 mm, Ptm-N = 43 mm, posterior facial height = low C. L1-APog = 2 mm, SN-GoMe = 27°, upper NLA = 110° D. Ramus height = 53 mm, facial depth = 130 mm, Björk sum = 390°
✅ Answer: B Explanation: Excessive upper incisor protrusion and reduced posterior maxillary length are signs of poor OT prognosis, favoring ASO.
5. A patient shows borderline criteria for both OT and ASO. What non-cephalometric clinical factor might guide the decision most effectively?
A. Dental arch shape B. Smile arc C. Lip strain on closure D. Curve of Spee
✅ Answer: C Explanation: Persistent lip strain despite normal incisor inclination is a strong indication for skeletal intervention.
6. If a patient has mild crowding, increased U1-NA, normal IIA, and a steep occlusal plane, what would likely happen if treated with OT alone?
A. Successful dental compensation and facial balance B. Improved profile with reduced lip eversion C. Residual lip incompetence and soft tissue dissatisfaction D. Increased interincisal angle and chin projection
✅ Answer: C Explanation: Without correcting steep occlusal plane and protrusive upper incisors, soft tissue results may remain suboptimal.
7. What is the clinical relevance of Ptm-N distance in treatment planning?
A. Represents vertical maxillary height B. Reflects maxillary length, affecting incisor support C. Indicates anterior-posterior mandibular position D. Directly correlates to upper lip thickness
✅ Answer: B Explanation: Ptm-N represents posterior maxillary length, crucial for determining maxillary support for anterior teeth.
9. In a clinical setting, what would justify two-jaw surgery over ASO alone for a BP patient?
A. Prominent upper incisors and increased U1-NA B. Skeletal Class II due to mandibular retrusion and steep occlusal plane C. Excessive overbite with upright lower incisors D. Soft tissue eversion without incisor proclination
✅ Answer: B Explanation: Skeletal Class II due to mandibular deficiency cannot be corrected with ASO alone—mandibular advancement is indicated.
Hey there, future smile designers! 👩⚕️👨⚕️ Let’s take a dive into something that keeps many orthodontists up at night (besides coffee and ceph tracings): Class II malocclusion—aka the “Oops, my mandible missed the memo to grow” situation. 😅
😬 What’s Class II Anyway?
Imagine your upper jaw (Maxilla the Diva 💁♀️) is strutting too far forward, while the lower jaw (Manny the Mandible 😶) is chilling way too far back. Not cute. That’s Class II malocclusion, and it happens in about 24% of orthodontic patients. That’s right—almost a quarter of your future clientele is walking around with a misaligned overbite!
🎯 The Game Plan: Grow that Jaw, Baby!
When the patient is still in their growth spurt era (cue dramatic puberty montage), we can:
Stimulate the mandible to catch up ⏩
Inhibit maxillary growth to slow the diva down 🛑
Or heck—do both like an orthodontic multitasker! 🙌
🤖 Enter: Fixed Functional Appliances (FFAs)
Now these appliances are like your strict tuition master. They don’t rely on patient mood, sugar levels, or whether the moon is in retrograde. They push the jaw forward 24/7. No break. No excuses. Not even during your cousin’s wedding in Madurai.
✅ The Good:
Works full time, even when the patient is playing PUBG.
No compliance issue, because we all know teenage boys only remember cricket scores, not elastics. 🙄
❌ The Problem:
These devices sometimes push the lower front teeth forward like an autorickshaw in peak traffic 🚖💨—anchorage loss, da! Which means:
Less skeletal correction
More chance of relapse (like that one ex who keeps coming back…even after you blocked them) 😑
🔩 TADs to the Rescue!
Temporary Anchorage Devices (TADs) are like your elder sister who holds the line when relatives start asking about your marks. Strong. Silent. Supportive. 💪
But for serious cases, we need the big guns—miniplates. Surgical anchors that go into the bone. Yes pa, real screws in real bones. 🪛🦴
🦷 Enter: Forsus Fatigue Resistant Device (FRD)
This one is like the Rajinikanth of functional appliances. No-nonsense. Always working. Introduced in 2001, this hybrid hero pushes the mandible forward while gently whispering to the maxilla, “Slow down, akka!”
The latest version? Forsus FRD EZ2 – sounds like something from an engineering boy’s final-year project, no? 😄
It attaches from maxillary molar to mandibular archwire and applies forces that say:
“Mandible, get up and move!”
“Maxilla, sit down and behave.”
All day, all night. No complaints. Just action. 💥
🔬 So What Did This Turkish Study Do?
Our fellow dental researchers in Turkey (no, not the country you eat during Christmas, pa—the actual country 🇹🇷) asked:
“Which is better—conventional Forsus FRD or Forsus FRD with miniplate anchorage?”
They wanted to see how each affects:
🦴 Skeletal changes
🦷 Tooth movement
👃 Soft tissue profile
So here’s how the groups panned out:
MA-Forsus Group (Miniplate Anchored): 15 bravehearts (2 girls + 13 boys) said, “Surgery? Bring it on!” They were fitted with Forsus FRD EZ2 + Miniplates for approx 9.4 months.
C-Forsus Group (Conventional): 15 polite refusals (8 girls + 7 boys) said “No knife, please!” Treated with standard Forsus FRD EZ2 for approx 9.46 months.
All patients got 0.018″ Roth brackets. But like filter coffee, how you serve it makes all the difference ☕👇
MA-Forsus: Only upper arch teeth got bonded (minimalist vibes)
C-Forsus: All maxillary and mandibular teeth bonded, second molars too (go big or go home)
For C-Forsus kids:
Maxillary molars got the headgear tubes
Mandibular archwire joined the fun between canine & premolar
(Simple setup, but no drama-free guarantee)
For MA-Forsus champs:
These kids got a full VIP treatment, surgical-style 🏥💪
🪛 Miniplate Insertion:
Under local anesthesia (brave heroes, truly)
A 10mm horizontal incision ~5mm above the gum line
Mucoperiosteal flaps lifted (like dosa batter, gently and with care)
Two miniplates placed with:
7mm screws at the top
9mm screws at the bottom
1.5–2mm space between plate and mucosa (no one wants sore spots, okay?)
Sutures out on day 7, and boom—ready for action! 💥
Then, Forsus FRDs were attached like this:
Upper part: maxillary molar tubes
Lower part: miniplate long arms (anchorage of the gods, I tell you!) 🙏
📸 Records, Because Pics or It Didn’t Happen
A total of 90 lateral cephs were taken at 3 stages:
🕰️ T0 – Before treatment
📈 T1 – After leveling
🎯 T2 – After Forsus phase
Each ceph was analysed for 17 landmarks and 16 measurements (7 angular + 9 linear) using Dolphin Imaging 🐬💻 (Because nothing says science like measuring bones with a software named after a sea mammal!)
RESULTS
Aspect
Conventional Forsus (C-Forsus)
Miniplate-Anchored Forsus (MA-Forsus)
Comments
Maxillary Growth (SNA angle)
Significant decrease (maxilla growth restricted)
Significant decrease (same as conventional)
Both act like headgear — saying “Hey maxilla, don’t go forward!”
Effective Maxillary Length (Co-A)
Significant increase
Significant increase
Maxilla tries to grow a bit anyway — biology is tricky!
Mandibular Growth (SNB & Co-Gn)
Increase (~2.5 mm growth)
Greater increase (~3.69 mm growth)
Miniplate gives better anchorage — mandible grows more confidently, like a proud hero flexing muscles!
Mandibular Rotation (SN/GoGn angle)
No significant change
Significant posterior rotation
MA-Forsus pushes mandible down and back!
Face Height (Anterior & Posterior)
Significant increase
Significant increase
Face grows taller as mandible adjusts
Maxillary Incisor Position
Retrusion (moved backward)
Retrusion
Both cause upper front teeth to move backward — no more “bird beak” smile!
Mandibular Incisor Position
Proclination (tipped forward)
Retrusion (moved backward)
MA-Forsus stops unwanted forward flaring — very good news for patients!
Upper Lip Position
Retrusion (moves backward)
Retrusion
Upper lip follows upper incisors.
Lower Lip Position
Protrusion (moves forward)
No significant change
Lower lip behaves depending on incisor movement — with miniplate, it stays chill like a calm pond.