Crohn’s disease is an inflammatory bowel disease of unknown aetiology. However, it shares many features with the autoinflammatory diseases,and some cases are known to be associated with mutations in the gene NOD2 that controls inflammatory responses to bacteria. Mutations cause failure of the formation of the mucin and antimicrobial barrier lining the bowel and may also inhibit degradation of bacteria. Changes in bowel flora are probably also important. Granulomatous inflammation affects the ileocaecal region, causing thickening and ulceration. Symptoms vary with the severity of the disease, but effects can include abdominal pain, variable constipation or diarrhoea and, sometimes, obstruction and malabsorption. Repeated bowel resections may ultimately be needed. Many other sites can be affected including any part of the bowel, joints and skin. Treatment controls symptoms but is not curative. Dietary adjustment, corticosteroids, antibiotics, sulfasalazine or mesalazine, immunosuppressants and tumour necrosis factor (TNF)-alpha blockers (e.g. infliximab) are used.
Oral effects 1)Most patients have no oral signs, although aphthous ulcers and candidosis may be associated with anaemia.
2)When the disease process itself affects the mouth, the signs and symptoms are the same as those in orofacial granulomatosis.
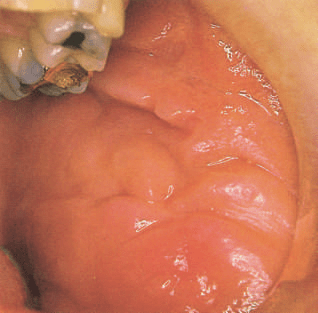
3)Non-caseating granulomas resembling those in the intestine develop in the oral mucosa. The common sites of involvement are lips and buccal mucosa. These show prominent oedema with folds tethered to the underlying deeper tissues, producing the characteristic cobblestone mucosa appearance.
4)Linear ulcers often run along the buccal sulci, particularly the lower sulci, and have hyperplastic folds of inflamed mucosa along their margins. The gingiva show an erythematous nodular gingivitis with hyperplastic tags.
5)The granulomas are typically small, loose and contain few multinucleate giant cells and are often sited deeply in underlying muscle. They may be few in number, and a biopsy needs to extend unusually deeply to increase the chance of finding them because only by identifying granulomas can the diagnosis be made. The granulomas are associated with vascular dilatation and tissue swelling in early disease. Later, there is dense fibrosis that fixes the tissues in their distorted shape.
These features can be the presenting features of Crohn’s disease, and occasionally oral lesions precede gastrointestinal symptoms by a long period. Oral disease is much more likely to progress to bowel disease in children than when diagnosed in an adult.
Typical orofacial features of Crohn’s disease: • Diffuse soft or tense swelling of the lips, or mucosal thickening • Cobblestone thickening of the buccal mucosa, with fissuring and hyperplastic folds • Gingivae may be erythematous and swollen • Sometimes, painful mucosal ulcers, linear in sulci or resembling aphthae • Mucosal tags in sulcuses • Glossitis due to iron, folate or vitamin B12 deficiency can result from malabsorption • Orofacial granulomatosis shares many features
Management
Oral lesions may lessen in severity with treatment of systemic disease. Aggressive treatment is merited in the early stages to prevent fibrosis and permanent disfigurement. The same drugs as are used for bowel disease are required, together with steroid injections of swollen mucosa.
Dr. Iswarya V, BDS
REFERENCE: Cawson’s Essentials of Oral Pathology and Oral Medicine – E. W. Odell
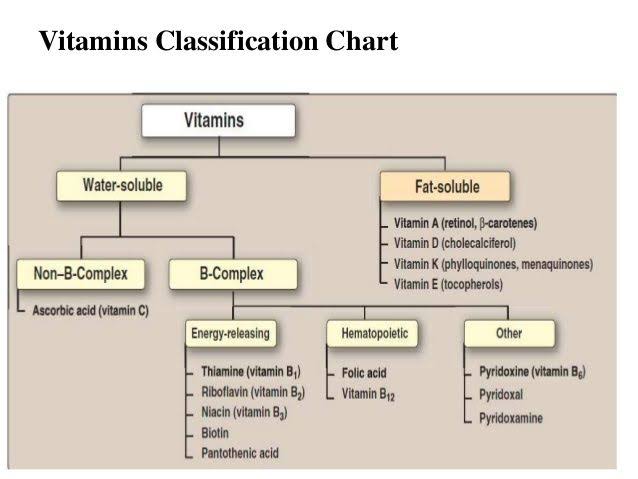
Vitamin A deficiency is one of the most common vitamin deficiency syndrome.
It is fat soluble vitamin.
It is common cause of blindness.
Clinical features :-
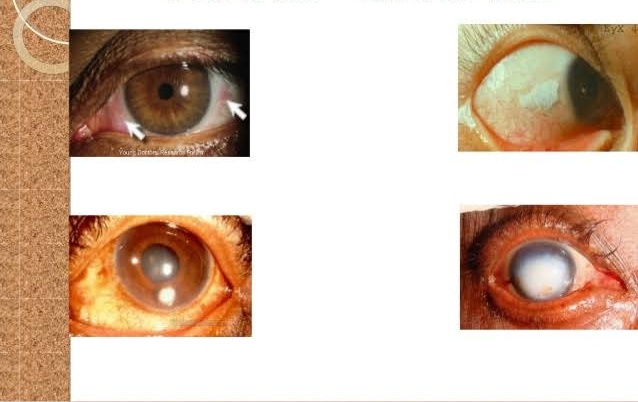
A. OCULAR FEATURES :-
Night blindness.
Bitot’spot.
Corneal ulceration.
Blindness.
Xerophthalmia
B. EXTRAOCULAR FEATURES :-
Hyperkeratotic skin lesions
Anorexia
Growth retardation
Decreased SalivarySecretion.
Hyperplastic gingiva.
Periodontal disease.
Defective formation of enamel in teeth
Treatment :-
A. Consumption of vitamin A–rich foods, such as liver, beef, chicken, eggs, fortified milk, carrots, mangoes, sweet potatoes, and leafy green vegetables.
B. Daily oral usage as supplements are as follows :-
Children aged 3 years or younger – 600 mcg (2000 IU)
Children aged 4-8 years – 900 mcg (3000 IU)
Children aged 9-13 years – 1700 mcg (5665 IU)
Children aged 14-18 years – 2800 mcg (9335 IU)
All adults – 3000 mcg (10,000 IU)
Consumption of multivitamins as supplements.
Reference :-
Image :- Google Writing :- notes made from mastering bds , Dr S N chugh and Sanjay Kumar Purkait books
The following fundamental rules apply to every surgical procedure, concerning the incision and flap:
1) The incision must be carried out with a firm, continuous stroke, not interrupted strokes. During the incision, the scalpel should be in constant contact with bone. Repeated strokes at the same place,many times, impair wound healing.
2) Flap design and incision should be carried out in such a way that injury of anatomic structures is avoided, such as: the mental neurovascular bundle, palatal vessels emerging from the greater palatine foramen and incisive foramen, infraorbital nerve, lingual nerve, submandibular duct, parotid duct, hypoglossal venous plexus, buccal artery (of concern when incision of an abscess of the pterygomandibular space is to be performed), facial nerve and facial artery and vein, which are of concern basically for the drainage of abscesses performed with extraoral incisions.
3)Vertical releasing incisions should begin approximately at the buccal vestibule and end at the interdental papillae of the gingiva.
4) Envelope incisions and semilunar incisions, which are used in apicoectomies and removal of root tips, must be at least 0.5 cm from the gingival sulcus.
5) The elliptic incision, which is used for the excision of various soft tissue lesions, comprises two convex incisions joined at an acute angle at each end, while the depth of the incision is such that there is no tension when the wound margins are sutured.
6) The width of the flap must be adequate, so that the operative field is easily accessible, without creating tension and trauma during manipulation.
7) The base of the flap must be broader than the free gingival margin, to ensure adequate blood supply and to promote healing.
8) The flap itself must be larger than the bone deficit so that the flap margins, when sutured, are resting on intact, healthy bone and not over missing or unhealthy bone, thus preventing flap dehiscence and tearing.
9) The mucosa and periosteum must be reflected together. This is achieved (after a deep incision)when the elevator is continuously kept and pressed firmly against the bone.
10) When the incision is not made along the gingival sulcus, for esthetic reasons, and especially in people with broad smiles, the scar that will result must be taken into consideration, particularly on the labial surface of the front teeth.
11) During the surgical procedure, excessive pulling and crushing or folding of the flap must be avoided, because the blood supply is compromised and healing is delayed.
Types of Flaps Various types of flaps have been described in oral surgery, whose name is based mainly upon shape. The basic flap types are: trapezoidal, triangular, envelope, semilunar, flaps created by and incisions, and pedicle flaps.
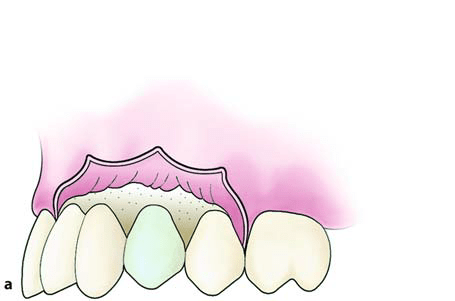
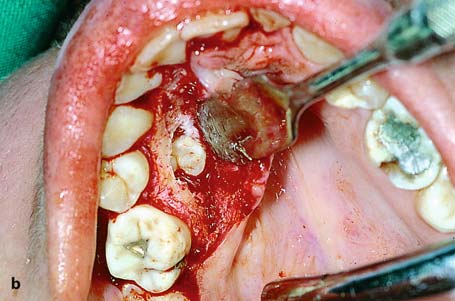
Trapezoidal Flap The trapezoidal flap is created after an incision, which is formed by a horizontal incision along the gingivae, and two oblique vertical releasing incisions extending to the buccal vestibule. The vertical releasing incisions always extend to the interdental papilla and never to the center of the labial or buccal surface of the tooth. This ensures the integrity of the gingiva proper, because if the incision were to begin at the center of the tooth, contraction after healing would leave the cervical area of the tooth exposed. A satisfactory surgical field is ensured when the incision extends at least one or two teeth on either side of the area of bone removal. The fact that the base of the resulting flap is broader than its free gingival margin ensures the necessary adequate blood supply for the healing process. The trapezoidal flap is suitable for extensive surgical procedures, especially when the triangular flap would not provide adequate access.
Advantages. Provides excellent access, allows surgery to be performed on more than one or two teeth, produces no tension in the tissues, allows easy reapproximation of the flap to its original position and hastens the healing process. Disadvantages. Produces a defect in the attached gingiva (recession of gingiva).
Triangular Flap This flap is the result of an L-shaped incision, with a horizontal incision made along the gingival sulcus and a vertical or oblique incision. The vertical incision begins approximately at the vestibular fold and extends to the interdental papilla of the gingiva. The triangular flap is performed labially or buccally on both jaws and is indicated in the surgical removal of root tips, small cysts, and apicoectomies.
Advantages. Ensures an adequate blood supply, satisfactory visualization, very good stability and reapproximation; it is easily modified with a small releasing incision, or an additional vertical incision, or even lengthening of the horizontal incision. Disadvantages. Limited access to long roots, tension is created when the flap is held with a retractor, and it causes a defect in the attached gingiva.
Envelope Flap This type of flap is the result of an extended horizontal incision along the cervical lines of the teeth. The incision is made in the gingival sulcus and extends along four or five teeth. The tissue connected to the cervical lines of these teeth and the interdental papillae is thus freed. The envelope flap is used for surgery of incisors, premolars and molars, on the labial or buccal and palatal or lingual surface, and is usually indicated when the surgical procedure involves the cervical lines of the teeth labially (or buccally) and palatally (or lingually), apicoectomy (palatal root), removal of impacted teeth, cysts, etc.
Advantages. Avoidance of vertical incision and easy reapproximation to original position. Disadvantages. Difficult reflection (mainly palatally), great tension with a risk of the ends tearing, limited visualization in apicoectomies, limited access, possibility of injury of palatal vessels and nerves, defect of attached gingiva.
Semilunar Flap This flap is the result of a curved incision, which begins just beneath the vestibular fold and has a bowshaped course with the convex part towards the attached gingiva. The lowest point of the incision must be at least 0.5cm from the gingival margin, so that the blood supply is not compromised. Each end of the incision must extend at least one tooth over on each side of the area of bone removal. The semilunar flap is used in apicoectomies and removal of small cysts and root tips.
Advantages. Small incision and easy reflection, no recession of gingivae around the prosthetic restoration, no intervention at the periodontium, easier oral hygiene compared to other types of flaps. Disadvantages. Possibility of the incision being performed right over the bone lesion due to miscalculation, scarring mainly in the anterior area, difficulty of reapproximation and suturing due to absence of specific reference points, limited access and visualization, tendency to tear.
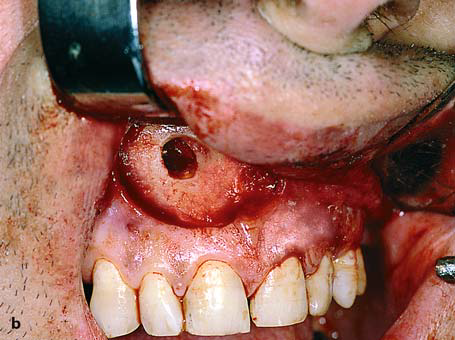
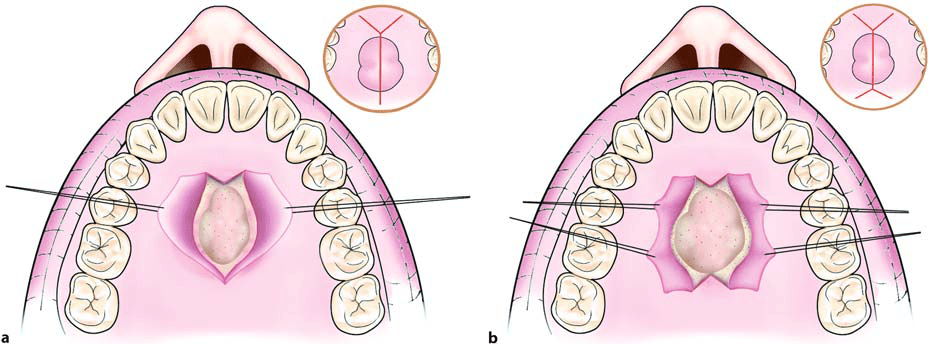
Flap Resulting from Y-shaped Incision.An incision is made along the midline of the palate, as well as two anterolateral incisions, which are anterior to the canines. This type of flap is indicated in surgical procedures involving the removal of small exostoses.
Flap Resulting from X-shaped Incision. This type of flap is used in larger exostoses, and is basically an extension of the -shaped incision. The difference is that two more posterolateral incisions are made, which are necessary for adequate access to the surgical field. This flap is designed such that major branches of the greater palatine artery are not severed.
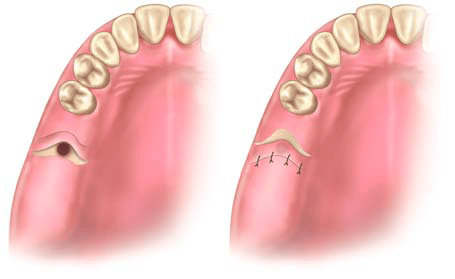
Pedicle Flaps The three main types of pedicle flaps used for closure of an oroantral communication are: buccal, palatal, and bridge flaps.
Buccal Flap. This is a typical trapezoidal flap created buccally, corresponding to the area which is to be covered, and is usually used on dentulous patients. It is the result of two oblique incisions that diverge upwards, and extend as far as the tooth socket. After creating the flap, the periosteum is incised transversally, making it more elastic so that it may cover the orifice that results from the tooth extraction. The oblique buccal flap is a variation of the buccal flap. It is the result of an anteroposterior incision, so that its base is perpendicular to the buccal area, posterior to the wound. The flap is rotated about 70°-80° and is placed over the socket. Both cases require that, before placing the flap, the wound margins must be debrided.
Palatal Flap. This type of flap is used in edentulous patients so that the vestibular depth is maintained. The resulting palatal mucoperiosteal flap is rotated posteriorly and buccally, always including the vessels that emerge from the corresponding greater palatine foramen. After rotation, the flap is placed over the orifice of the socket, the wound margins are debrided, and the flap is sutured with the buccal tissues. A gingival dressing is applied for a few days at the void created and healing is achieved by secondary intention.
Pedicle Bridge Flap. This flap is palatobuccal and is perpendicular to the alveolar ridge. After creation, the flap is rotated posteriorly or anteriorly, to cover the orifice of the oroantral communication, without compromising the vestibular fold. This type of flap is used only on edentulous parts of the alveolar ridge.
Dental caries is caused by bacteria, and as ozone will kill certain bacteria,many studies have investigated whether ozone is effective in arresting the progression of caries. No serious side effects to the treatment have been reported.
Advocates of this treatment modality recommend ozone as a disinfectant gas to eliminate bacteria from occlusal caries (up to 2mm in depth), root carious lesions, and pit and fissure lesions, often with the absence of further operative treatment. The carious lesion is encouraged to remineralize over 4 weeks using fluoride and mineral mouthwashes, toothpaste, and sprays.
Baysan and Lynch (2004) found that ozone application for 10–20s eliminated most of the microorganisms found in primary root caries lesions. Ozone can reduce the numbers of S. mutans and S. sobrinus on saliva-coated glass beads in vitro (Baysan et al. 2000). However, the role that this disinfection process can play in the long-term reversal of previously active carious lesions is controversial.
Rickard et al. (2004) analyzed the available published literature and concluded that “given the high risk of bias in the available studies and lack of consistency between different outcome measures, there is no reliable evidence that application of ozone gas to the surface of decayed teeth stops or reverses the decay process.” Further research is necessary
With the HealOzone system (KaVo Dental, Biberach, Germany), ozone gas is delivered via a special handpiece that fits over and bathes the tooth. HealOzone (KaVo Dental, Biberach, Germany) delivers ozone gas, which disinfects the tooth. The minimally carious lesion is encouraged to remineralize over a period of 4 weeks using fluoride and mineral mouthwashes, toothpaste and sprays.