Artificial intelligence refers to the stimulation of human intelligence in machines that are programmed to think like humans and mimic their actions.
On the other hand, artificial general intelligence (AGI) is probably what we are thinking of when we hear AI. AGI isn’t quite developed yet. AI, however, is very much present and growing in every industry, from consumer technology to health care
How is AI currently used in dentistry?
In dentistry, AI is being used for different applications. First, AI is currently being used for voice commands, such as with DEXvoice by Simplifeye and DEXIS (software platforms).
Phrases such as “Alexa, show me the bitewings of number 19” will soon be uttered in dental practices around the country.
Through machine learning, MMG Fusion’s chairfill ( software designed to help dental practices fill holes in the schedule) retrieves data from a dentist’s record and analyzes it. Chairfill can find the most profitable dentistry not yet provided, communicate with patients directly, and even book patients appointments. It does all of this without human involvement.
Scientists are already using AI in caries detection. One company utilising AI in this way is Dentistry.ai. Its algorithm is designed to take a large data set of radiographs and recognise patterns within that data. As a result, it hepls practitioners more accurately to identify carious lesions.
The founders of Dentistry.ai predict that AI will be tightly woven into the fabric of how dentistry is done.
The primary llimitationsto AI are insufficient data and inaccurate data. This means that clinicians today should focus on collecting the data now to be able to use it fully in the future. If we can do that, we can continue to provide greater care to our patients.
Advancement in technology led to its usage in various fields and it helped build new devices that were not possible 10 or 20 years ago and made most of the jobs easier.
Such advancements include application of nanotechnology in dentistry, also known as nanodentistry, allows for treatment possibilities in restorative dentistry, orthodontics and periodontics.
Within restorative dentistry, nanorobots can be used in cavity preparation, restoration, and even dentition renaturalization.
Due to their size, nanobots work at the atomic, cellular, and molecular level to perform major tasks and help dentists in managing complicated cases at the microscopic level with ease and precision.
Bottom-up Approaches :
Local Nanoanaesthesia –
A colloidal suspension containing millions of anesthetic dental nanorobots would be used to induce local anaesthesia. Deposited on the gingival tissue, the nanorobots would reach the dentin and move toward the pulp via dentin tubules guided by a nanocomputer under the control of dentist. On reaching pulp, the analgesic robots may close down all sensation in tooth. When the treatment procedure is done, the nanorobots may be ordered to re-establish all sensations and to exit from the tooth
Tooth repositioning :
All the periodontal tissues, namely the gingiva, periodontal ligament, cementum and alveolar bone, may be directed by orthodontic nanorobots leading to Swift and pain-free corrective movements
Nanorobotic dentifrice (Dentifrobots):
Toothpastes or mouthwashes could contain the dentifrobots which would then survey all gingival surfaces regularly.
dentifrobots
Dental durability and cosmetics :
Nanostructured composites can be included with sapphire 12 or diamond to reduce their brittleness which are used to enhance the toughness and appearance of teeth.
Diagnosis of oral cancer :
Nanoscale cantilevers : elastic beams used to attach with cancer linked molecules
Nanopores : small holes that enable DNA passage one strand at a time, this making DNA sequencing highly efficient
Nanotubes : carbon rods that can detect affected genes and also localise their location
Quantum dots : these glow very brightly in UV light. They attach to proteins associated with cancer cells, this localizing tumours
A nanoshell is a tiny bead like structure with superficial metal layers which may imbibe selective wavelengths of radiations and lead to large amounts of heat production. This results in specific devastation of the tumour cells, sparing the normal cells.
Dental nanomaterials – anodentistry as top-down approach :
Nanocomposites :
Nanofillers are minute particles, igher proportions can be achieved, and result in distinctive physical, mechanical and optical properties.
One nanocomposite system has three different types of fillers : non agglomerated discrete silica nanoparticles, barium glass and prepolymerized filler
Nanosolutions are constituted by dispersible nanoparticles, which are then used as a component in bonding agents.
Advantages – higher dentin and enamel bond strength, high stress absorption, longer shelf life, durable marginal seal, flouride release
Impression materials :
Traditional vinylpolysiloxanes have incorporated Nanofillers which produce a distinctive material with improved flow, enhanced hydrophilic properties and superior detail precision.
Nano-composite denture teeth :
Porcelain teeth are highly wear resistant but are brittle, acrylic on the other hand undergo undue wear. Nanocomposite denture teeth are made of PMMA and homogenously distributed Nanofillers
Advantages – excellent polishing ability and stain resistant, superb esthetics, enhanced wear resistance and surface hardness
Dentifrices :
These are mainly made of nanosized hydroxyapatite molecules. They will result in protective shell on tooth surface and may even repair damaged areas. Microbrite dentifrice has microhydrin which breaks down the organic food particles
Prosthetic implants :
Nanotechnology would aid in the development of surfaces with definite topography and chemical composition leading to predicable tissue integration. Tissue differentiation into definite lineage will accurately determine the nature of peri implant tissues. Eg- nanotite, nano-coatef implant
Nano sterilizing solution :
A new sterilizing solution following nanoemulsion concept has been developed by Gandly Enterprises Inc Florida. Nanosized oil droplets attack and destroy the pathogens. Eg – eco tru disinfectant
Nanotechnology may utilize genetic engineering, tissue engineering and tissue regeneration initially, followed by growing whole new teeth in vitro and their iinstallation
Nanotechnology will bring enormous changes in the field of dentistry when few challenges such as precise manufacture of nanoscale parts, financing and tactical concerns, social issues have overcome.
Gigantism : it is a rare condition that causes abnormal growth in children.
Cause : a pituitary tumour is almost always the cause of gigantism. Gigantism is due to hypersecretion of GH in childhood or in the preadult life before the fusion of epiphysis of bone with shaft.
Other less common causes of gigantism include McCune-Albright syndrome causes abnormal growth in bone tissues, patches of light brown skin, and gland abnormalities
Carney complex is an inherited condition that causes non cancerous tumours on connective tissue, cancerous or non cancerous endocrine tumours
Signs of gigantism – very large hands and feet, thick toes and fingers, a prominent jaw and forehead, coarse facial features, excessive sweating, insomnia, delayed puberty, deafness
Treatment – surgery (removing the tumour), bromocriptine and cabergoline are drugs that can be used to lower growth hormones, Gamma knife radiosurgery
Acromegaly : it is the disorder characterized by enlargement, thickening and broadening of bones.
Cause : acromegaly is due to hypersecretion of GH in adults after the fusion of epiphysis with the shaft of the bone and a benign tumour affecting the pituitary called adenoma
Signs : vision loss, protrusion of supra orbital ridges, broadening of nose, thickening of lips, prognathism, carpal tunnel syndrome, uterine fibroids in women, arthritis, sleep apnea
Acromegalic Gigantism: it is a rare condition with symptoms of both acromegaly and gigantism.
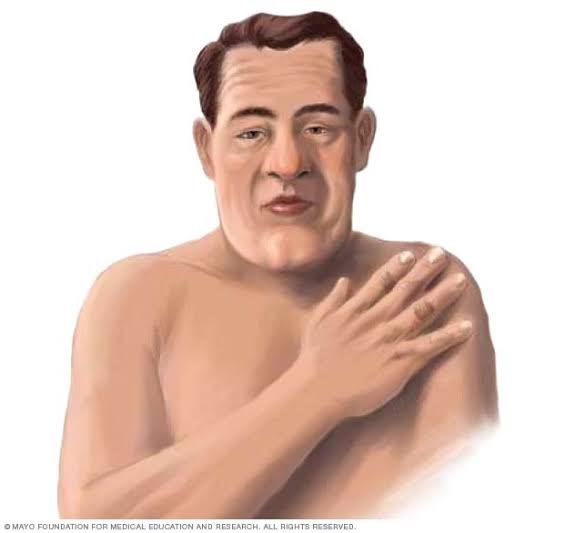
Cushing’s disease : it is a hormonal disorder caused by high levels of the hormone cortisol in your body. It’s also known as hypercortisolism.
Causes : most common cause is related to medications called glucocorticoids, one can also get the disease from injectable steroids, such as repeated shots for joint pain, bursitis, back pain
Symptoms – buffalo hump, rounded and rosy face, thinning skin, acne, being very tired, kidney stones, sleep problems
Treatment : surgery, hormone replacement medications, life style changes
Hypoactivity of anterior pituitary gland:
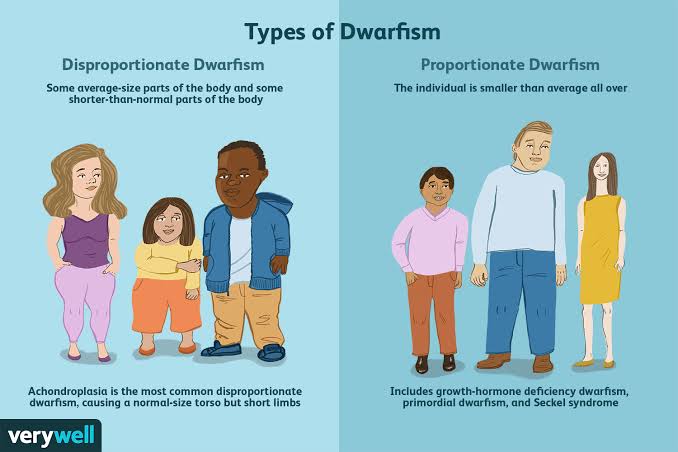
Dwarfism : it is a pituitary disorder in children characterized by stunted growth
Causes : reduction of GH secretion in infancy or early childhood due to deficiency of GHRH from hypothalamus or somatomedin C, atrophy or degeneration of acidophilic cells in the anterior pituitary, achondroplasia
Signs : stunted skeletal growth, head becomes slightly larger in relation to the body, reproductive function is not affected, mental activity is normal
treatment : corrective surgeries, surgery to widen spinal cord, extended limb lengthening
Acromicria : it is characterized by the atrophy of the extremities of the body
Causes : deficiency of GH releasing hormone from hypothalamus, tumour of chromophobes, panhypopituitarism (reduction in secretion of all hormones of anterior pituitary gland)
Signs : atrophy and thinning of extremities of body, hypothyroidism, person becomes lethargic and obese
Simmonds’ disease : it is also called pituitary cachexia
Cause : occurs mostly in panhypopituitarism
Symptoms : rapidly developing senile decay, loss of hair over body and loss of teeth, skin on face becomes dry and wrinkled
Hyperactivity of posterior pituitary gland:
Syndrome of inappropriate hypersecretion of antidiuretic hormone : it is characterized by loss of sodium through urine duebto hypersecretion of ADH
Cause : due to cerebral tumours, lung tumours and lung cancers
Signs and symptoms : loss of appetite, weight loss, nausea and vomiting, headache, muscle weakness, spasm, cramps
Hypoactivity of posterior pituitary gland:
Diabetes inspidus : it is characterized by excess excretion of water through urine
Cause : deficiency of ADH which occurs due to lesion or degeneration of supra optic and paraventricular nuclei of hypothalamus, atrophy of posterior pituitary
Signs : polyuria, polydypsia (intake of excess water) and dehydration
Toothbrushes have been in existence since thousands of years and have become an indispensable part of our life. Earlier it used to be in the form of chew stick format but over time, different formats of tooth brushes emerged such as tree twigs, bird feathers and porcupine quills.
Let us know about the different type of toothbrushes available in today’s market
Manual toothbrush
The most common form of toothbrush available in our homes is manual toothbrush.
Bristles available for this type of toothbrush are soft, medium or hard bristled. Most dentists advice soft bristled brush but other two help in removal of more plaque but that may wear away the enamel if brushed too hard
Round or square shaped headed toothbrushes are available but diamond shaped head is more convenient to rach the back and sides of molars
Toothbrush handle design includes straight, contra-angle, non-slip grip and flexible types.
Electric toothbrush
An electric toothbrush performs rotations of its bristles and cleans hard to reach places. Some even have timers to help you brush more effectively. It has been discovered that compared to a manual brush, the multi-directional power brush might reduce the incidence of gingivitis and plaque.
Electric toothbrushes are further divided into three types depending on speed of its movements – standard power toothbrushes
standard power toothbrush
Sonic toothbrush is powered toothbrush that is fast enough to produce a hum in the audible frequency
sonic electric toothbrush
Ultrasonic toothbrush is a powered toothbrush which is faster than the sonic toothbrush
ultrasonic toothbrush
Interdental toothbrush
Also called interproximal brush used for cleaning between teeth and between the wires and dental braces and teeth
interdental toothbrush
Sulcabrush
it is used specifically to clean along the gumline adjacent to the teeth.
A sulcabrush is ideal for cleaning specific difficult-to-reach areas, such as between crowns, bridgework and crowded teeth.
sulcusbrush
End-tuft brush
It is a small round brush head compromising of Seven tufts of tightly packed soft nylon bristles, trimmed so the bristles in the center can reach deeper into small spaces.
gum end-tuft brush
Chewable toothbrush
It is a miniature plastic molded toothbrush which can be placed inside the mouth.
They are generally used by travellers
It is usually available in different flavours such as mint or bubble gum
chewable toothbrush
Ecological toothbrush
These are toothbrushes made out of biodegradable substances such as wooden handles, bristles of bamboo or pig bristles and replaceable heads
Group 1- Cleft of soft palate only Group 2 – Cleft of hard and soft palate extending no further extending than involving incisive foramen, (secondary palate only) Group 3 – Complete unilateral cleft, extending from uvula to incisive foramen in the midline, then deviating the one side and usually extending through the alevolus at the position of the future lateral incisor Group 4- Complete bilateral cleft, extending forward through incisive foramen to alevolus. Premaxilla, suspended from the nasal septum . Asian population have highest frequency often
CLINICAL FEATURES:-
Incidence- 1in 500,With african population the lowest at 1in 250. Cleft lip alone more common in males. Isolated Cleft palate more common in female. 50% are syndromic, and are born with other congenital abnormalities.Cleft lip appear as unilateral / bi lateral. Line of cleft start on lateral part of upper lip and continues through philtrum of alveolus between lateral incisor and canine. When cleft lip continues from incisive foramen through palatal suture middle in palate,cleft lip with palate (unilateral/bilateral) present . . Cleft palate appears with involving soft palate only, involving uvula (bifid uvula),isolated cleft palate also. .Patient have significant physical and physiological effects like, difficulty in eating and drinking with regurgitation of food to nose. . Speech problem . Ear infection: Malposition of Eustachian tubes result in middle ear infection .Cosmetic deformities.
MANAGEMENT
Management of Cleft lip and palate require, multidisciplinary coordinated approach by specialist including maxillofacial surgeon, pediatric surgeon, anesthetist, Prosthodontist, Orthodontist, Speech pathologist, otolaryngology ,audiologist etc..
Management is aimed at closure and correction of lip and palate, secondary correction of palatal fistulae, orthodontic management of malocclusion, Orthognathic surgery, Rhinoplasty,and providing prosthesis for patients.
Pre operative criteria selected by physicians for surgery is Millards Rule of 10’s 1) 10lb weight 2) 10mg/l of haemoglobin 3) 10 weeks of age
SURGICAL MANAGEMENT 1) Primary : Closure of lip & palate 2) Secondary : Closure of palatal fistula, Pharygoplasty ,Bone grafting, orthodontic management Rhinoplasty and Scar revision.
Reference: Oral and Maxillofacial surgery, Balaaji. Textbook of general surgery for dental students, SRB
Cleft palate and Cleft lip comprises the complex of Orofacial clefts . Both comprises congenital malformations affecting oro-facial region. Failure of fusion of nasal and maxillary process leads to cleft of primary palate which can lead to unilateral and bilateral. Cleft of secondary palate is medial, Varies from bifid uvula to complete cleft palate up to incisive foramen.
Etiology:- Clinically, Isolated Cleft palate and Cleft lip with or without Cleft palate has been established.
Factors playing role in Development of Orofacial cleft comprises
1)Heredity (40%of cleft lip and 20% cleft lip appear genetically- single gene/polygenic mutation, Monozygotic twins far likely to get) 2)Nutritional disturbances (experimentally proved in rat fed on abnormal dietary regimen caused cleft palate) mostlty- Riboflavin,Folic Acid Deficiency.
3) Physiologic, Emotional stress, Traumatic also thought to cause 4) Circulating Alcohol ,Drugs ,toxins. 5)Environmental Factors– Teratogens (phenytoin, methotrexate, Corticosteroid, Sodium Valproate) 6)Syndromic Clefting Treacher collins syndrome Pierre Robin Syndrome Stickler syndrome Oro Facial Digital syndrome Trisomy of 13,18 Van Der Voude syndrome ( lip pit syndrome, autosomal dominant , deletion of 1q32 , clinically presenting with cleft lip and palate and medial pits on lower lips on vermillion border.Also include ankyloglossia,high arch palate ,maxillary hypodontia and sygnathia)
EMBRYOGENESIS AND CLEFTING
During sixth and seventh weeks of development upper lips forms when median nasal process merges each each other and fuses with maxillary process of 1st branchial arches. Mid portion of upper lip is derived from median nasal process, lateral derived from maxillary process. Lateral nasal process involved in ala of nose. Primary palate is formed from merging of median nasal process to form intermaxillary segment, which give rises to premaxilla (bone including 4 incisor teeth). Secondary palate make up 90% of palate formed from maxillary process of first branchial arches.Defective fusion of median nasal process with maxillary process forms cleft lip. Failure of palatal shelves to fuse result in cleft palate 45% are Cleft lip with palate 30% Cleft palate alone 25% with isolated cleft lip
Vander Woude syndrome with lower lip pits.Van der Woude Syndome with lip pits , Cleft lip and palate.
Reference:- Textbook of maxillofacial surgery- Balaji. Textbook of embryology- Inderbir Singh. Neville Oral pathology. Images credits : Image 1 – Internet medscape (https://emedicine.medscape.com/article/950823-overview
Wilson’s disease, also known as hepatolenticular degeneration and progressive lenticular degeneration, is a rare genetic disorder that causes copper overload in the body.
Common cause of liver cirrohsis in children.
Etiology:- A mutation in the ATP7B gene, which codes for copper transportation, causes Wilson’s disease
Characteristic clinical signs:- SUNFLOWER CATARACT AND KAYSER-FLEISCHER RINGS. KF rings are golden brown ring like discoloration of eyes due to copper deposition.
Lab investigation:- Altered Liver enzymes Elevated Serum copper level Increased urinary copper excretion. Low Serum ceruloplasmin level. Liver biopsy will reveal copper deposition. Imaging like MRI/CT for lenticular imaging.
Treatment:-. Copper chelating agents like d-penicillamine, Trientine etc.. can be used. Oral Zinz tetrathiomolybdate can be given ti reduce dietary absorption of Copper.
Atherosclerosis is characterized by intimal lesions called atheromas that protrude into vessel lumens.
An atheromatous plaque consists of a raised lesion with a soft, yellow, grumous core of lipid (mainly cholesterol and cholesterol esterscocered by a white fibrous cap.
Major risk factors for atherosclerosis:
Non modifiable factors –
Age : atherosclerosis is typically progressive, it does not usually manifest clinically until middle age or later
Gender : premenopausal women are relatively protected aginst atherosclerosis compared to age-matched men. After menopause, however, the incidence of atherosclerosis related diseases increases and at older ages actually exceeds that of men
Genetics : family history is theost significant independent risk factor for atherosclerosis. The well established familial predisposition to atherosclerosis is usually multifactorial, relating to inheritance of various genetic polymorphisms and hypertension or diabetes
Modifiable risk factors :
Hyperlipidemia : and more specifically hypercholesterolemia is a major risk factor for atherosclerosis, hypercholesterolemia is sufficient to stimulate lesion development. LDL cholesterol is the form of cholesterol that is delivered to peripheral tissues. In contrast, HDL mobilizes cholesterol from tissue and transports it to the liver for excretion in the bile.
Hypertension : it is the most important cause of left ventricular hypertrophy and hence the latter is also related to IHD
Cigarette smoking : the increased risk and severity of atherosclerosis in smokers is due to reduced level of HDL, deranged coagulation system and accumulation of carbon monoxide in the blood that produces carboxyhemoglobin and eventually hypoxia in arterial wall favouring atherosclerosis.
Diabetes mellitus : the incidence of atherosclerosis is twice as high in diabetics as in non diabetics. There is also an increased fold of strokes and a 100-fold increased risk of atherosclerosis induced gangrene of the lower extremities.
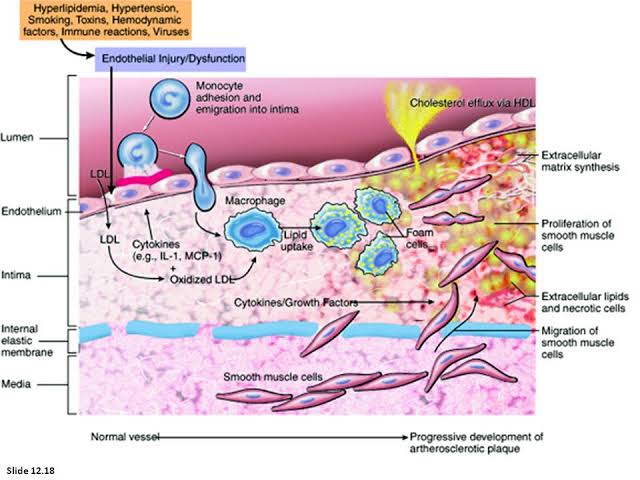
Pathogenesis of atherosclerosis :
Endothelial injury – endothelial loss due to any kind of injury results in intimal thickening.
The etiological culprits contributing to endothelial cell dysfunction in early atherosclerosis include hypertension, hyperlipidemia, toxins from cigarette smoke, homocysteine and even infectious agents
Hemodynamic disturbances – plaques tend to occur at Ostia of existing vessels, branch points, and along the posterior wall of the abdominal aorta, where there are disturbed flow patterns
Lipids – the dominant lipids in atheromatous plaques are cholesterol and cholesterol esters. Chronic hypercholesterolemia can directly impair endothelial cell function by increasing local oxygen free radical production; oxygen free radicals can injure tissues and accelerate nitric oxide decay, reducing its vasodulator activity
Inflammation – monocytes transform into macrophages and avidly engulf lipoproteins including oxidised LDL . Activated macrophages produce reactive oxygen species that aggrevate LDL oxidation and elaborate growth factors that drive smooth muscle cell proliferation
Infection – herpes virus, cytomegalovirus, Chlamydia pneumoniae have all been detected in Atherosclerotic plaques but not in normal arteries.
Smooth muscle cell proliferation – initial smooth muscle cell proliferation and ECM deposition convert a fatty streak, the earliest lesion into a mature atheroma and contribute to progressive growth of atherosclerotic lesions
Sequence of cellular interactions in atherosclerosis
Morphological features of atherosclerosis:
Fatty streaks and dots : they may be the precursor lesions of atheromatous plaques and are prominent in aorta and major arteries
Gelatinous lesions : they develop in the intima of the aorta and may also be the precursora of plaques
Atheromatous plaques : a fully developed atheromatous lesion is called atheromatous plaque. Most often and severely affected is the abdominal aorta. Grossly they are white to yellowish white lesions varying in diameter from 1-2 cm. Microscopically, superficial luminal part of fibrous cap is covered by endothelium, and is composed of smooth muscle xells; cellular area under the fibrous cap is composed of mixture of macrophages, foam cells, lymphocytes; deeper central soft core consists of extracellular lipid material, cholesterol clefts,fibrin; in oldrr and more advanced lesions, the collagen in the fibrous cap may be dense and hyalinised
Complicated plaques – various pathologic changes that occur in fully developed atheromatous plaques are called the complicated lesions. Calcification, ulceration, thrombosis, hemorrhage , aneurysm formation are the complications
evolution of lesions in atherosclerosis
Source : Robbins and Cotran’s book of pathology and Harsh Mohan’s textbook of pathology