• Granuloma is defined as a circumscribed tiny lesion and it’s about 1 mm in diameter. Granuloma is derived from word granule means granule like lesion and oma suffix generally refers to tumour but here it refers to collection of macrophages.
• Granuloma is type 4 hypersensitivity reaction. It’s protective but sometimes leads to tissue destruction because of poorly digestible antigen.
Pathogenesis :-
• Macrophages and monocyte engulf the antigen and tries to destroy it since the antigen is poorly degradable these cells fail to destroy antigen and macrophages undergoes morphological changes and transform into epitheloid cells.
• As macrophages have failed to destroy antigen they present it to CD 4 T lymphocytes. Lymphocytes get activated and releases interleukin 1 and interleukin 2 that stimulate more T cells, interferon gamma activates macrophages.
• And also TNF alpha that promotes proliferation of fibroblasts and activates the endothelium to secrete prostaglandin and growth factors which stimulate fibroblast growth.
Composition of granuloma
• Epitheloid cells are nothing but modified macrophages these are elongated cells and have slipper shaped nucleus . Nuclear chromatin is vesicular and lightly stained and cytoplasm is abundant and pale staining with hazy outlines.
• Multinucleate giant cells formed by the fusion of adjacent epitheloid cells containing more than 20 nuclei. The nuclei may be arranged like horseshoe or ring or may be clustered at 2 poles ( langhans gaint cell seen in tuberculosis ) or may be present centrally ( foreign body giant cell seen in foreign body tissue reaction).
• lymphoid cells as response to cell mediated immunity to antigen lymphocytes are the integral composition of granuloma. In some granulomas presence of plasma cells is indicative of humoral immune response.
• Necrosis is a feature of some granulomataous conditions like TB.
• Fibrosis is a feature of healing formed by fibroblast at the periphery.
So, Granuloma is having epitheloid cells at centre with interspersed gaint cells , surrounded peripherally lymphocytes and healing by fibroblast. Granuloma is a microscopic finding and it indicates chronic inflammation.
• Glass ceramics are the material that are initially formed as glass, and then transformed into ceramic usually by a controlled heat treatment.
• The heat induces partial devitrification which increases the strength as well as improves aesthetics by making it less transparent and more teeth like.
• The two glass ceramics used in dentistry are Castable glass ceramics and pressable glass ceramics.
• Advantages :- Ease of fabrication, Good aesthetics, improved strength and fracture toughness, Good marginal fit, very low processing shrinkage, low abrasion of opposing teeth.
• Disadvantages :- Inadequate strength for posterior teeth.
Castable glass ceramics
•It’s properties are more closer to that of glass and it’s construction is quite different. This is only porcelain restoration that is made by centrifuging casting technique.
• The subsequent Ceramming process is also quite unique to this porcelain Ceramming will enhance the growth of mica crystals within the ceramic.
• It is first commercially available glass ceramic for dental use was Dicor.
• features :- The dicor glass ceramic crowns are very aesthetic. This is because of greater translucency (unlike the other porcelain which have more opaque core). It also picks up some of the color from adjacent teeth (chaemelon effect) as well as from underlying cement.
Uses:- inlays , onlays , veneers
Fabrication of a dicor crown:-
• wax pattern is constructed first and then invested with a refractory material.
• After burnout of the wax ,nuggets of the dicor glass are melted and cast into the mould in centrifuging casting machine.
• The glass casting is carefully recovered from the investment by sandblasting and the sprues are gently cut away.
•The glass restoration is then covered with embedment material to prepare it for next stage that is Ceramming.
• Ceramming is the heat treatment process by which the glass is strengthened. Ceramming results in the development of microscopic crystals of mica which
– improves the strength and toughness of glass
– improves the aesthetics of the restoration ( it reduces the transparency of the glass making it more opaque and less glass like)
• The cerammed glass can be built up with special veneering porcelain and fired to complete the restoration. Surface stains may be applied to improve the aesthetics.
Reference :- Manapalil text book of dental materials
A 72 – year – old Caucasian female presents with a chief complaint of: “ I need new partial dentures and a new crown, so I can chew better. ”
She is partially edentulous in the maxilla and the mandible and has multiple fixed partial dentures.
LEARNING GOALS AND OBJECTIVES – Sequence treatment of a patient requiring a combination of fixed and removable prostheses.
– Discuss critical design elements for/removable partial dentures. – Use a surveying instrument. – Understand parameters for abutment selection for removable partial dentures. – Recognize and treat common postinsertion sequelae.
Odontogenic infection is an infection that originates within a tooth or in the closely surrounding tissues. The term is derived from Greek words “odonto” meaning “tooth” and “genic” meaning “birth”.
Odontogenic infection has plagued human kkind for as long as the human species has existed. Generally, in the orofacial region, most bacterial infections involve either a disturbance of normal flora or a displacement of the normal organisms to the site, where they are usually not seen.
Routes of odontogenic infection :
By direct continuity through tissues
By lymphatics to the regional nodes
By bloodstream
Causes of odontogenic infection :
Dental caries : plaque on tooth surface above the gingival margin consists of acidogenic and aciduric bacteria which cause dental caries and may invade the pulp, infection eventually spreading to the alveolar process.
Deep fillings : if the seal between the tooth enamel and the filling breaks down, food particles and decay causing bacteria can work their way under the filling. Additional decay develops in the tooth. Decay that is left untreated can progress to infect the dental pulp and may cause an abscessed tooth.
Failed root canal treatment : if there is an extended delay between root canal procedure and crown placement, bacteria can re-enter the tooth. Additionally, a crown can suffer a crack or other damage long after the procedure is complete. This damage allows new bacteria to enter the tooth and create decay.
Pericoronitis and periodontal diseases
Odontogenic infections are usually polymicrobial involving both strict anaerobes and facultative bacteria within unique ecosystems of the dental plaque and gingival crevice.
The most prevalent anaerobic bacteria include gram positive cocci such as Peptostreptococcus sp., and gram negative rods such as Bacterioids sp., Fusobacterium sp. The most prevalent aerobes are facultative gram positive such as Streptococcus mutans and Streptococcus viridans. Facultative gram negative bacilli and Staphylococcus aureus are uncommon in immunocompetent hosts but may be more important in immunocompromised patients.
Major symptoms of odontogenic infections :
Antecedent toothache
Facial swelling and pain
Fever and chill
Halitosis
Bleeding gums with minor trauma
Prominent physical findings include :
Dental plaques, tooth decay, gingivitis or periodontal pockets
Facial or neck swelling and tenderness
Inability to open the jaw
Difficulty in swallowing
Dyspnea with inspiratory stridor (high pitched wheezing sound caused by disrupted airflow)
Imaging studies :
Orthopantomogram or AP radiograph of teeth to assess periapical abscess or advanced periodontal disease
CT of face and neck to assess source and extension of orofacial space infection
Complications :
Deep facial space infections
Osteomyelitis of the jaws
Cavernous sinus thrombosis
Hematogenous dissemination
Association of poor health with cardiovascular diseases
Clinical manifestations of specific odontogenic orofacial space infections :
If pus perforates through either the maxillary or mandibular buccal plate inside the attachment of the buccinator muscle, infection will be intraoral; if the perforation is outside this muscle attachment, infection will be extraoral
When a mandibular infection perforates lingually, it presents in the sublingual space if the apices of the involved teeth lie above the attachment of the mylohyoid muscle.
Other superficial odontogenic orofacial space infection include the buccal, submental, masticator, canine and infratemporal spaces.
Treatment :
In normal host :
Penicillin G + metronidazole
Ampicillin – sulbactam
Clindamycin
Doxycycline
Moxifloxacin
In immunocompromised host :
Cefotaxime or ceftrioxime or cefepime each + metronidazole
•Our denture base is hard not flexible.So polyamide is added in flexible dentures to make them flexible and enhance the properties.
• Allergic reaction with conventional denture bases is because of free monomer and due to polymethyl methacrylate.
• Main properties of using flexible denture bases over the conventional ones are to avoid allergies to acrylic and metal and to improve retention.
• To improve aesthetic and make them more acceptable to patient.
• Flexible dentures help to avoid some kind of pain associated with old style denture models.
• Flexible denture bases helps to achieve greater stability and comfort.
• In addition to these benefits flexible denture are also designed to be porous and to breathe better.
• This helps to prevent the build up of bacteria on the denture.
• Nowadays it has become selective treatment of option. No more ugly metal wires.No more broken dentures.
• It is indicated in full dentures , partial dentures. Unique features of flexible denture Base are flexibility, strength, transparency, high impact resistance and high solvent resistance.
• Commercial names of flexible denture base are valplast, proflex, sunflex, unbreakable flexit plus dentures.
*Brief Summary* – Patient has come with complaint of loose RPD on left side which is due to little retention. Dental History of mutliple extractions, endodontic therapy, FPD and RPD.
*What may be the reason for compromised RPD?* READ THE PDF. Nicely Explained
*Treatment Options:* Extractions and CD Conventional RPD Implant retained RPD
Since Patient has expressed the desire to maintain his remaining teeth. We go with Implant retained RPD
Early detection and diagnosis of dental caries reduces irreversible loss of tooth structure, the treatment costs and the time needed for restoration of the teeth. Dental caries often initiates at the fissures in the occlusal surface of the tooth. Conventional examination for caries detection is primarily done using visual inspection, tactile sensation and radiographs. While these methods give satisfactory results in detection of cavitated lesions, they are usually inadequate for the detection of initial lesions. Because of these deficiencies, new detection methods have been developed to aid better diagnosis.
Conventional Methods Used in Diagnosis of Dental Caries
It is one of the most common diagnosis methods implemented by dentists. In order to make an accurate assessment, the teeth should be clean, dry and examined under a light source. In visual examination, changes in tooth structure such as; enamel dissolution, white spot lesions, discoloration, surface roughness and presence of cavitation are assessed. When illuminated, the carious tissues scatter the light and make enamel look whiter and opaque. This is due to increased porosity caused by demineralization. Similarly, when dentin undergoes demineralization, a shadow is observed under the intact enamel. When caries progress, the surface breaks down and a cavitation is formed.
The explorer and the dental floss are used for tactile examination but the use of an explorer is not preferred because:
Sharp tip of the explorer can produce traumatic defects on the enamel surface,
The cariogenic bacteria may be transferred from one tooth surface to another,
Probing may cause cavitation and fracture in the incipient lesions,
Explorers have low sensitivity resulting in undetected lesions.
If the explorer catches or resists removal when moderate pressure is applied, and when this is accompanied by one of the following;
Softness at the base of the lesion,
Opacity adjacent to the pit or fissure,
The enamel is softened adjacent to the pit and fissure, we can conclude that the area is carious.
Pickard, proposed the use of dental floss for the detection of caries. When there is food packing between the teeth and the floss is frayed when passed through the contact area, this might be the indication of caries.
Clinically “sound” and apparently intact occlusal surfaces, however, may develop lesions which penetrate into the dentin, which can be observed only through radiographic examination
Radiographic examination has great value in detecting caries lesions especially when they are not clinically visible. In low caries population, as a result of fluoride use, the surface of enamel does not break down, making the caries detection harder. In recent years, the incidence of such lesions has increased dramatically. According to studies, bitewing radiography has been proven to be an effective method in the detection of proximal caries and hidden caries. Besides its advantages, radiographs also have some limitations too. For this reason, it is advisable to use clinical evaluation along with radiographic imaging. The disadvantages of radiography are as follows: • Proximal contacts are overlapped, • The lesion depth may appear to be increased due to angulation and this may lead to false diagnosis, • Occlusal lesions may not be detected because of the superposition of the buccal and lingual cusps, • The real cause of the radiolucency can’t be determined whether it is due to caries, resorption or wear, • The superficial demineralization of the buccal and lingual surfaces may seem like proximal caries, • Active and arrested caries can’t be distinguished in the radiographs. • Radiographs may give false positive results due to a phenomenon called “Mach band effect”. In this perceptual phenomenon, the contrast between the dark and lighter areas has increased, resulting in a dark demarcation band. This effect causes formation of a radiolucent area in dentin enamel junction.
• Cervical burn out is another optical phenomenon where a wedge shaped radiolucent area is seen between the bone and the cemento-enamel junction. This effect is due to tissue density and the low penetration of X-rays at the cervical region.
Despite the disadvantages, radiographs are the most commonly used diagnosis tool and with the development of new techniques many of the problems are solved.
There are two layers of decalcification in carious dentin. The first one is the soft and infected layer which doesn’t have the capacity of remineralization. The second one is hard, intermediately decalcified and has the ability of remineralization. Many studies were carried out to differentiate these layers. Although there are opinions stating the benefit of caries detection dyes, there are also opinions that dyes can lead to over-reduction in the dentin.
Most clinical investigations have concluded that, caries detection dyes don’t stain bacteria but stain the less mineralized organic matrix. In a study of Demarco et al. they suggested that dye remnants that remained on the walls of the cavity may cause a decrease in the shear bond strength between the composite restorations and the enamel.
In the upcoming blog post we will learn about the Novel Methods for Caries Detection..
Happy Reading😊
References: Meandros Med Dent J 2018;19:1-8, Image source: Google
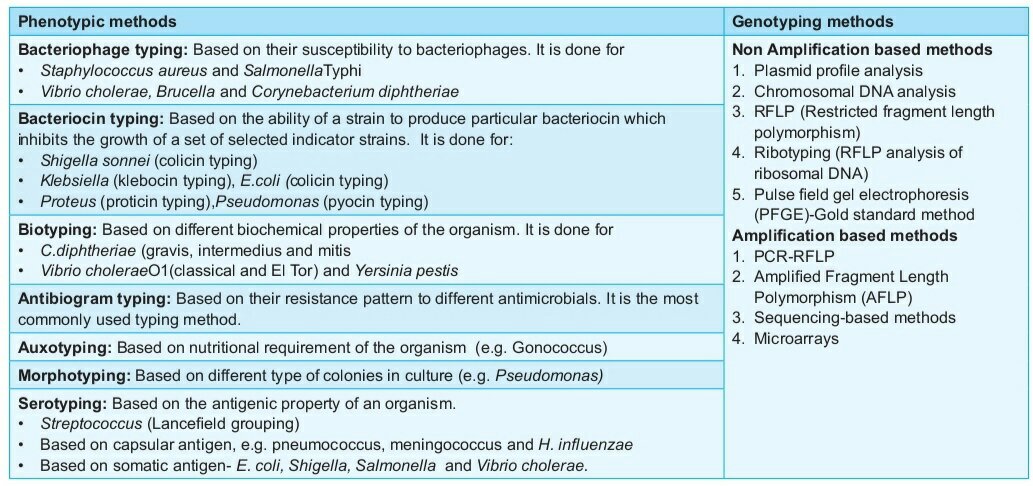
• In microbiology we often come across this word typing in simplest words means classification of microorganisms
• Typing is broadly classified as
– Phenotypic methods
– Genotypic methods
• Genotypic methods are the ones which analyse the kind of genes present on chromosomes and plasmids of microorganisms. They are used to know whether the genes are homologous or heterologous
• And also to know certain specific genes whether they are present or absent and similar other attributes of the genes . They are way more complicated to do and interpret the results as these are expensive methods , hence they are not used in routine diagnostic purpose.
• phenotypic methods are the commonly used methods. These methods are used for diagnostic purpose. These methods are based on observable characters or physical characters of microorganism like shape, size, results from biochemical reaction, susceptibility or resistance to antibiotics or other certain viruses.
• Common type of phenotypic methods is serotyping. Serotyping refers to sero means surface and typing means classification. Serotyping is based on differences in the different structures decorated on the surface of microorganism.
• Serotyping is based on the surface structures such as lipopolysaccharides,membrane proteins, capsular polysaccharide, fimbriae and flagella.