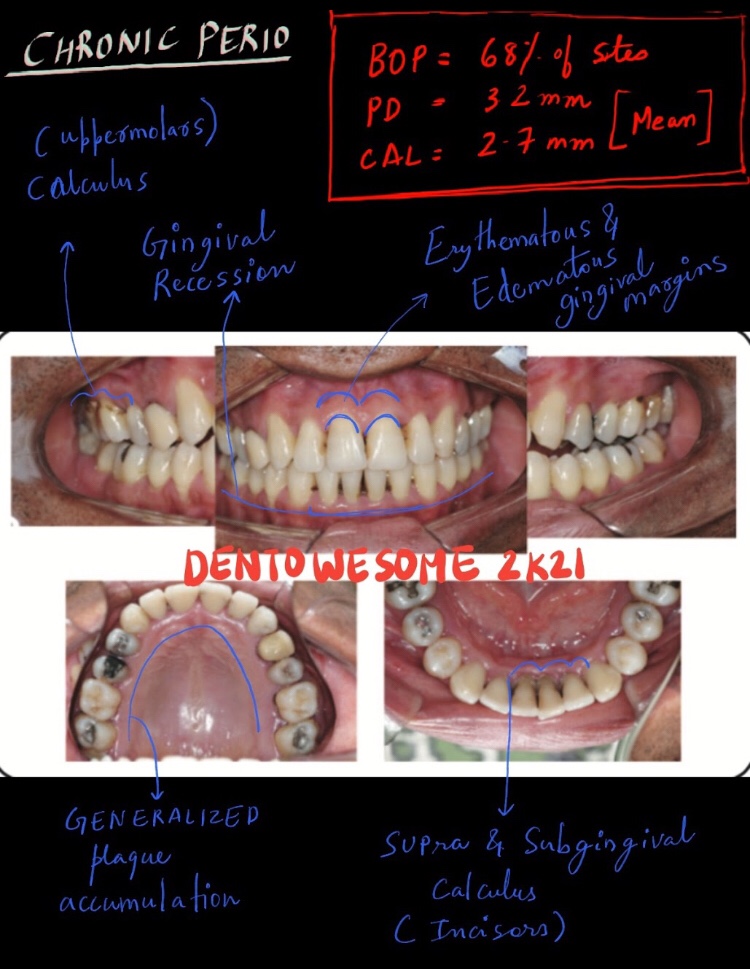
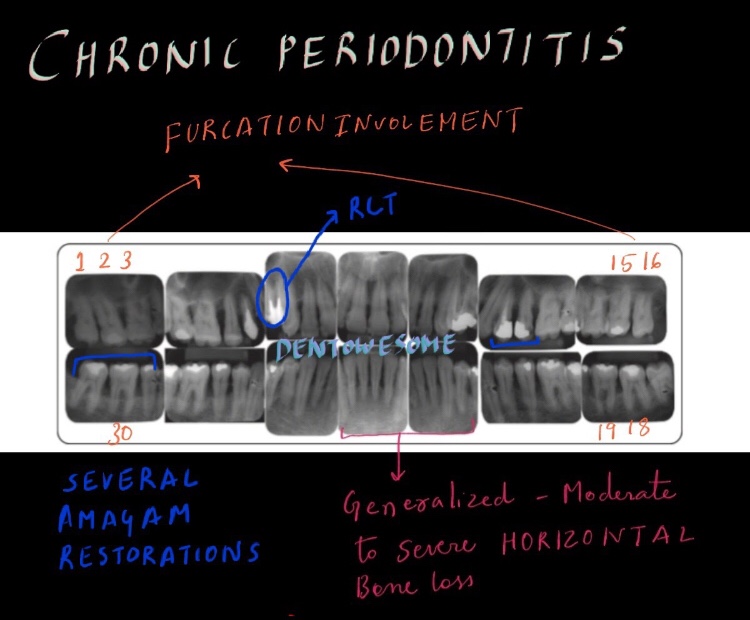
LEARNING GOALS AND OBJECTIVES To be able to identify the clinical features and overall characteristics of chronic periodontitis To be able to list difficulties in the proper diagnosis of early chronic periodontitis To understand possible overlaps with the diagnosis of aggressive periodontitis
To know what clinical changes can be anticipated in the response of chronic periodontitis to anti-infective therapy
A swelling is a value term that denotes only enlargement or protuberance in body due to any cause.
According to the cause a swelling may be congenital, traumatic, inflammatory, Neoplastic or miscellaneous.
Examination of a swelling should be accompanied by a complete history of the patient. Following points should be noted:
• Duration: The clinician may ask ‘when was the swelling first noticed’? Swellings that are painful and of shorter duration are mostly inflammatory (acute), whereas those with longer duration and without pain are chronic, e.g. a chronic periapical abscess.
• Mode of onset: The clinician may ask ‘how did the swelling start’? The history of any injury or trauma or any inflammation may contribute to the diagnosis and nature of the swelling.
• Progression: The clinician should ask ‘has the lump changed in size since it was first noticed? Benign growths such as bony swellings grow in size very slowly and may remain static for a long period of time. If the swelling decreases in size, this suggests of an inflammatory lesion.
• Site of swelling: The original site where it started must be assessed.
• Other symptoms: Pain, fever, difficulty in swallowing, difficulty in respiration, disfigurement, bleeding or pus discharge are the common symptoms associated with swellings in the orofacial region.
• Recurrence of the swelling: many swellings do recur after removal of the tissue, indicating the presence of precipitating factor, e.g. ranula.
LOCAL EXAMINATION🔍
(A) Inspection
Situation: few swellings are peculiar in their position
Color: Black – Naevus/Melanoma; Red/purple: Hematoma; Bluish: Ranula
Shape: Ovoid, pear shaped, kidney shaped, spherical or irregular
Size: Mention in cms. – the vertical horizontal dimension
Surface: Cauliflower as in Squamous Cell Carcinoma; Filliform – Papilloma
Edge: Sessile/pedunculated/indistinct
Number: Multiple/diaphyseal
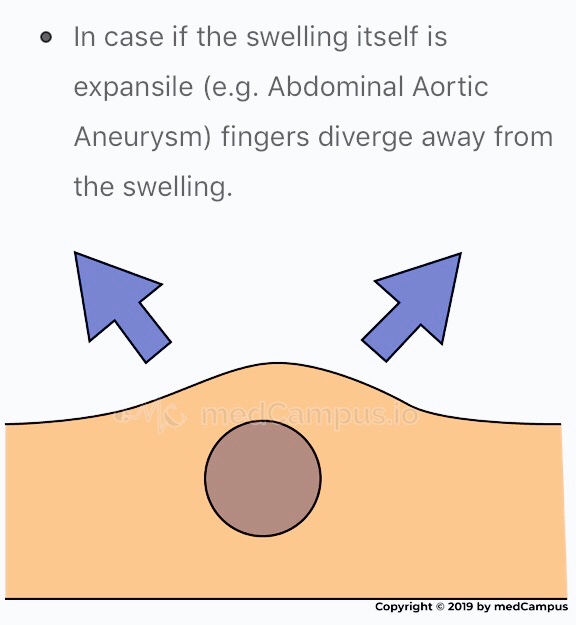
Pulsation: The swelling which is superficial to artery, in close relation with it will be pulsatile. Pulsatile nature of swelling is assessed with 2 fingers on mass.
Mnemonic: SETTLE
Skin: Red & edematous. Pigmentation of skin is seen in moles or after repeated exposure to X-rays. Skin over a growth looks like the peel of an orange.
(B) Palpation
Temperature: Local temperature is raised due to extensive vascularity of the swelling; best felt with back of fingers.
Tenderness: Patient complains of pain due to pressure exerted by swelling.
Size, shape & extent: Mention in cms. – the vertical horizontal dimension
Fluctuation: If swelling contains liquid or gas it fluctuates.
Fluctuation test is positive if the two digits are pushed away in both directions.
Translucency: contains clear fluid
Compressibility: When pressure is applied to a swelling it decreases in size and when pressure is released swelling regains its size itself. Characteristic sign of VASCULAR HEMANGIOMA
Reducibility: Swelling reduces and ultimately disappears when pressed upon.
• Well defined & regular-Benign Neoplasms • Well defined & irregular-Malignant Neoplasms • Ill defined & diffuse - Inflammatory swellings
Consistency: 👇🏻
• Soft - lipoma • Cystic - Cyst or chronic abscesses • Firm - Fibroma • Hard - Chondroma • Bony hard - Osteoma • Stony hard - Carcinoma • Variable consistency - Malignancy
EXAMINATION OF ULCER:
An ulcer is break in continuity of epithelium, skin or mucous membrane. A proper history must be taken in case of an ulcer:
• Mode of onset: The clinician may ask ‘how has the ulcer developed’? The patient may provide significant information about the nature and etiology of the ulcer such as any trauma or spontaneously.
• Duration: The clinician may ask ‘how long is the ulcer present here’? It determines the chronicity of the ulcer. For example, traumatic ulcers in oral cavity are acute (occurring for a short period), but if the agent persists; it may become a chronic ulcer.
• Pain: The clinician may ask ‘is the ulcer painful’? Most of the ulcers, being inflammatory in nature, produce pain. Painless ulcers usually suggest nerve diseases (such as peripheral neuritis, syphilis, etc).
• Discharge: Any blood, pus or serum discharge must be noted.
• Associated disease: Any associated generalized systemic problem may be associated with the ulcers of oral cavity (such as tuberculosis, squamous cell carcinoma, etc).
Number: Tuberculous, inflammatory ulcer may be more than one in number
Position:
• Arterial ulcer: Tip of the toes, dorsum of the foot • Varicose ulcer: lower limb • Perforating ulcers: over the sole at pressure points • Non-healing ulcers: over the shin • Rodent ulcer: upper part of face
Edge: An area between margin & floor. In spreading ulcer, edge is inflamed. Undermined edges destroy subcutaneous tissue faster than skin.
Beaded: As seen in rodent ulcer
Floor: This is the part of the ulcer which is exposed or seen.
Tenderness: Characteristic of infected ulcers and arterial ulcers.
Induration: The edge, base and the surrounding area should be examined for induration
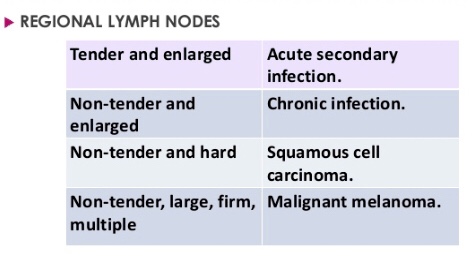
• Maximum induration - Squamous cell carcinoma • Minimal induration - Malignant melanoma • Brawny induration - Abscess • Cyanotic induration - Chronic venous congestion as in varicose ulcer
Mobility: Malignant ulcers are usually fixed, benign ulcers are not.
Bleeding: Malignant ulcer is friable like a cauliflower. On gentle palpation, it bleeds. Granulation tissue as in a healing ulcer also causes bleeding.
Surrounding Area:
Thickening and induration is found in squamous cell carcinoma.
Tenderness and pitting on pressure indicates spreading inflammation surrounding the ulcer.
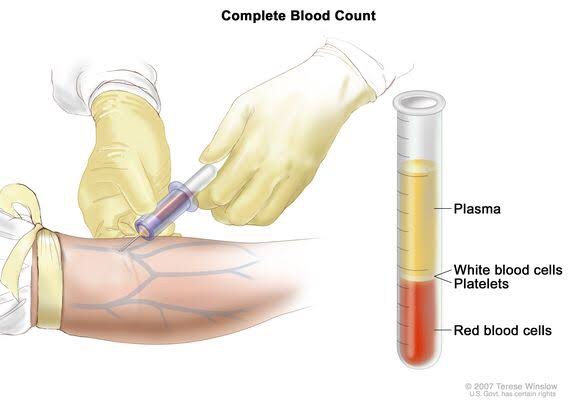
A blood sample drawn from a vein in your arm or a fingerstick or heelstick (newborns)
• Test Preparation Needed?
None
• Why get tested?
To determine your general health status; to screen for, diagnose or monitor any one of a variety of diseases and conditions that affect blood cells, such as anemia, infection, inflammation, bleeding disorder or cancer.
• Also known as: Hgb; Hb; H and H (Hemoglobin and Hematocrit)
• Sample Required?
A blood sample drawn from a vein in your arm or a fingerstick or heelstick (newborns)
• Test Preparation Needed?
None
• Why get tested?
To evaluate the hemoglobin content of your blood as part of a general health check-up; to screen for and help diagnose conditions that affect red blood cells (RBCs); If you have anemia (low hemoglobin) or polycythemia (high hemoglobin), to assess the severity of these conditions and to monitor response to treatment
• When to get tested?
With a hematocrit or as part of a complete blood count (CBC), which may be ordered as a component of a general health screen; when you have signs and symptoms of anemia (weakness, fatique) or polycythemia (dizziness, headache); at regular intervals to monitor these conditions or response to treatment
• Also known as: Thrombocyte count; PLT; Platelet distribution width; PDW; Mean Platelet volume; MPV.
• Sample Required?
A blood sample drawn from a vein in your arm or a fingerstick or heelstick (newborns)
• Test Preparation Needed?
None
• Why get tested?
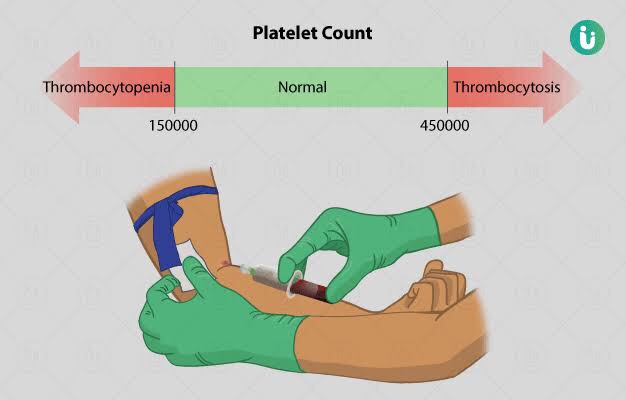
To determine the number of platelets in a sample of your blood as part of a health exam; to screen for, diagnose, or monitor conditions that affect the number of platelets, such as a bleeding disorder, a bone marrow disease, or other underlying condition.
• When to get tested?
As part of a routine complete blood count (CBC); when you have episodes of unexplained or prolonged bleeding or other symptoms that may be due to a platelet disorder
• What is being tested?
Platelets, also called thrombocytes, are tiny fragments of cells that are essential for normal blood clotting. They are formed from very large cells called megakaryocytes in the bone marrow and are released into the blood to circulate. The platelet count is a test that determines the number of platelets in a person’s sample of blood. When there is an injury to a blood vessel or tissue and bleeding begins, platelets help stop bleeding.
• Also known as: Leukocyte differential count; Peripheral differential; WBC count differential; Diff; blood differential; Differential Blood Count
• Formal name: White blood cell differential
• Why get tested?
To help determine the cause of abnormal results on a WBC count; to help diagnose or monitor an illness affecting your immune system, such as an infection or inflammatory condition, or cancers that affect your white blood cells, such as leukemia.
• When to get tested?
As part of a CBC; when you have a routine health examination; when results of a CBC fall outside the reference range; when you have any number of signs and symptoms that may be related to a condition affecting white blood cells, such as infection, inflammation, or cancer, when you are receiving treatment that is known to affect WBCs, such as chemotherapy.
• What is being tested?
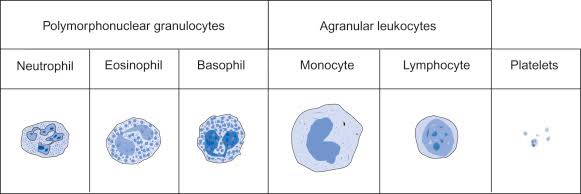
WBCs, also called leukocytes, are cells that circulate in the blood and the lymphatic system that help protect the body against infections. They are an important part of the body’s immune system and also have a role in inflammation, allergic responses, and protection against cancer. A WBC differential totals the number of each of the different types of WBCs in a person’s sample of blood.
There are five types of white blood cells, each with different functions.
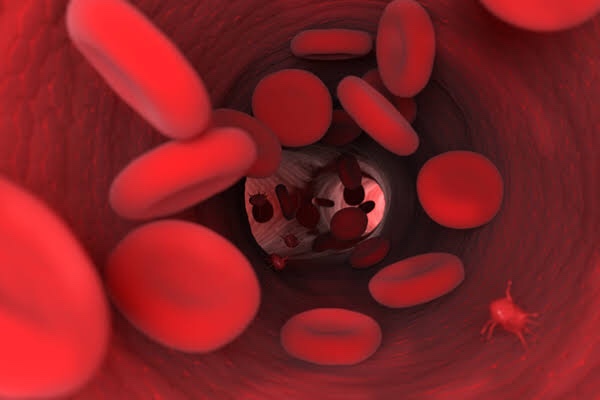
Red blood cells, also known as erythrocytes, make up thecellular part of blood, giving it its red color and also the ability to bind and carry oxygen to all parts of the body. Under a microscope, they appear to be circular and biconcave in shape.
Gives us the number of erythrocytes per cubic mm in circulating blood & Hb in blood.
Procedure done by office or chairside method and also automated procedure.
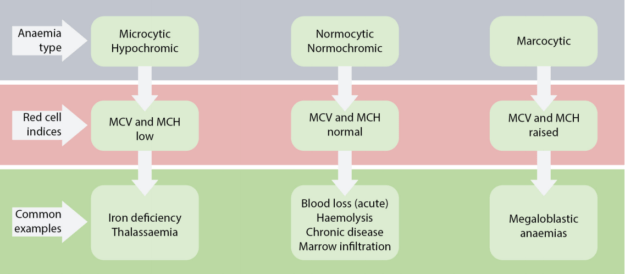
Hematological diseases of RBCs are anemia & polycythemia.
Categorized by mean corpuscular volume, anemia can be differentiated into microcytic, macrocytic and normocytic anemias. Normocytic anemia can be further divided into intrinsic and extrinsic RBC defect and blood loss.
MCV – Mean corpuscular volume is the average volume of red blood cells and is reflective of RBC size. When RBCs increase or decrease in size, the mean corpuscular volume changes; this helps physicians determine the type of anemia and its causes. Normal MCV is 80–96 µm³.
MCH stands for “mean corpuscular hemoglobin.” An MCH value refers to the average quantity of hemoglobin present in a single red blood cell.
MCHC is short for mean corpuscular hemoglobin concentration. MCHC refers to the average amount of hemoglobin inside a single red blood cell.
Hematocrit is the measure of the total volume % of red blood cells in the blood. The normal value for hematocrit is 45% for men and 40% for women. It is an important component of a patient’s complete blood profile.
• Swellings at the angle of Mandible include: ✍🏻👇🏻
🔅Congenital disease
• Branchial Cleft Cyst
🔅Neoplasm
(i) Benign
Hemangioma
Lymphangioma, Cystic hygroma
Pleomorphic adenoma (mixed tumor)
Warthin tumor
Neurofibroma
Angiolipoma
Adenoma
Hamartoma
Lipoma
Oncocytoma
(ii) Malignant
Mucoepidermoid carcinoma
Squamous cell carcinoma
Adenoid cystic carcinoma
Acinic cell carcinoma
Adenocarcinoma
Rhabdomyosarcoma
Lymphoma, leukemia
Metastatic adenopathy
🔅Inflammation/Infection
Parotitis
Parotid Abscess
Tuberculosis
Sarcoidosis
Sjögren disease
HIV
Detailed View🔍
1) Branchial Cleft Cyst:
Failure of involution of clefts and pouches lead to cysts, fistulas or sinus tracts.
Its a painless fluctuant swelling
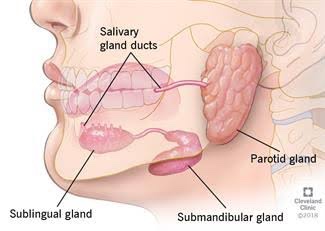
First branchial cleft cysts are rare usually located at parotid gland or periparotid region.
Second branchial cleft cyst – Type II are the most common
Typically, second branchial cleft cysts present as a rounded swelling just below the angle of mandible, anterior to the sternocleidomastoid
2) Hemangiomas:
They are the most common benign salivary gland mass. Capillary hemangiomas involve parotids
3) Lymphangiomas
They are congenital malformations of the lymphatic system that may involve the parotid gland (Soft asymptomatic neck mass associated with facial asymmetry)
4) Pleomorphic Adenoma:
Hard painless slow growing mass
5) Warthin Tumor:
Incorporation of heterotopic salivary gland ductal epithelium within intraparotid & periparotid nodes
6) Parotitis & Parotid Abscess:
Most common in children
Mumps is the most common viral cause of parotitis
The condition manifests tender swelling at the angle of Mandible
Sialadenitis is most commonly due to bacterial infections caused by Staphylococcus aureus.
Premature neonates and immunosuppressed individuals are affected.
• Swellings in the floor of Mouth: 👇🏻✍🏻
Ranula presents as a translucent blue, dome-shaped fluctuant swelling & contains viscid, glairy jelly like fluid
Ranula – a type of mucocele found on the floor of the mouth. Present as a swelling of connective tissue consisting of collected Mucin from a ruptured salivary gland by local trauma.
Swellings in the floor of the mouth are more likely to arise from structures above the Mylohyoid muscle. The commonest swellings in the floor of the mouth are denture induced hyperplasia & salivary calculus.
Swellings in the floor of the mouth may inhibit swallowing & speech.
Mandibular tori produce bony hard swelling lingual to the lower premolars.
Torus palatinus is an intrinsic bone lesion whereas a dental abscess pointing on the palate (usually from the palatal roots of the 1st & 2nd maxillary molars or from upper lateral incisors) is extrinsic.
Salivary neoplasms
Invasive carcinoma from the maxillary sinus may produce a palatal swelling.
Kaposi’s sarcoma, typical of HIV/AIDS may also present as lump on palate.
Colour : the colour of dental restorative materials is most commonly measured in reflected light using a colour measuring instrument or a visual method.
Colour measuring instruments
Spectrophotometers are amongst the most accurate, useful and flexible instruments for overall colour matching in dentistry. They measure the amount of light energy reflected from an object at 1-25 nm intervals along the visible spectrum
Colorimeters measure tristimulus (relating to values giving the amounts of the three colored lights red, green and blue that when combined additively produce a match for the colour being considered) values and filter light in red, green and blue areas of the visible spectrum.
Visual method : A popular system for the visual determination of colour is the Munsell colour system. A large set of colour tabs is used to determine the colour.
Value (lightness) is determined first by selection of a tab that most nearly corresponds with the lightness or darkness of the colour.
Chroma is determined next with tabs that are close to the measured value but are of increasing saturation of colour.
The hue of the colour is determined last by matching with colour tabs of the value and chroma already determined.
Transparence, translucence and opacity:
Opacity is the property of the materials that prevents the passage of light. Translucency is the property of substances that permits the passage of light but disperses the light, so objects cannot be seen through the material. Some translucent materials in dentistry are ceramics, resin composites and acrylics. Transparent materials allow the passage of light so little distortion takes place and objects may be clearly seen through them.
Teeth and oral tissue are translucent and allow passage of some of the incident light. In some individuals, the enamel may be translucent or in rare circumstances transparent.
Flourescence : It is the emission of luminous energy by a material when a beam of light is shone on it. The wavelength of the emitted light is usually longer than that of exciting radiation.
Generally, natural tooth structure also absorbs light of wavelengths which are too short to be visible to the human eye. The energy that the tooth absorbs is converted to light with larger wavelengths in which case the tooth actually becomes a light source. This phenomenon is called flourescence.
In UV light a natural tooth emits a weak whitish-blue flourescence. This should be taking into account when selecting restoratives. If restorative material do not offer this property, they will look dark in UV light and the restored tooth will stand out against the other teeth in the mouth eg. in some stage shows and discotheques.
Metamerism : The appearance of an object depends on the type of light by which the object is viewed. Objects that appear to be colour matched under one type of light may appear very different under another light source. This phenomenon is called metamerism. Hence, selecting a shade of tooth must be done under two different sources of light.
Radiological properties :
Radiopacity may be defined as the quality of a material to obstruct the passage of radiant energy, such as X rays. Thus the materials that inhibit the passage of electromagnetic radiation are called radiopaque. Those that allow radiation to pass more freely are called radiolucent.
Manufacturers add certain elements in many dental materials in order to make them radiopaque. Commonly used elements are heavy metal glasses and metal oxides (zirconium dioxide and ytterbium oxide). Pure polymers like acrylic resins and BISGMA are radiolucent. Composites, ceramics and metals are radiopaque, with metals showing the highest radiopacity. Within the tooth, enamel is more radiopaque than dentin. If the radiopacity of a material is too low, it will not be visible. Generally, a restorative material should have radiopacity slightly greater than that of enamel in order to present a contrast. Radiopacity increases with increase in thickness of a material. Aluminum is used as a standard to measure radiopacity.
Use of magnets in dentistry : they have been used for various applications in orthodontics and prosthodontics. They can be placed within prostheses without being obtrusive.
In orthodontics : their main use has been for tooth movement
In prosthodontics : they are primarily used as retentive aids in maxillofacial prosthesis and in tooth and implant supported.
source : craig’s and manapalli textbook of restorative materials
Provide an aesthetic result using contemporary restorative materials and techniques. Critical color matching Discussion of tooth whitening techniques Care and maintenance for all-ceramic, full- coverage restorations
LEARNING GOALS AND OBJECTIVES Provide an aesthetic result using minimally invasive techniques. Color matching Restore form, function, and aesthetics. Care and maintenance for a porcelain laminate veneer (PLV)
LEARNING GOALS AND OBJECTIVES Provide an aesthetic restoration using minimally invasive techniques. Discuss color matching Restore form, function, and aesthetics Care and maintenance for a porcelain laminate veneer (PLV) Medical Histo
It’s the interaction between the biological environment and the mechanical device that is fixed or removable prosthesis is called as biomechanics.
• They are 2 types of forces that is horizontal and vertical.
• The forces are directed in the vertical direction to the long axis of the tooth. Forces transferred by vertical direction are during mastication, clenching and swallowing.
• The forces transferred by the vertical direction is much more than the horizontal direction.
• The forces transferred by horizontal direction are mainly by the tongue and by perioral musculature.
• The factors for edentulism are trauma, patient’s oral hygiene, ageing , attitude of the patient , diet and financial status.
• If the forces are directed obliquely then the bone remodelling takes place and bone deposition will occur.
• In natural dentition , masticatory forces will be transferred through the periodontal ligament to the bone. The arrangement fibres in periodontal ligament also plays a major role.
• The periodontal ligament acts like a cushion and distributes the masticatory forces.
• The tooth is supported by the periodonium. Hard tissues supporting are cementum and bone and soft tissues are PDL and lamina propria of gingiva covered by the epithelium.
• The load taken up by the natural dentition is 20 kg and that in complete denture wearers is 8 kg.
• The major difference between the natural dentition is the compressibility of PDL and in the complete denture patient the oral mucous membrane has less compressibility to deliver forces.
• Normal mastication – 30 sec. Act of deglutution – 18 sec.
• We swallow about 500 times in a day and masticate about 17 minutes approximately in a day.