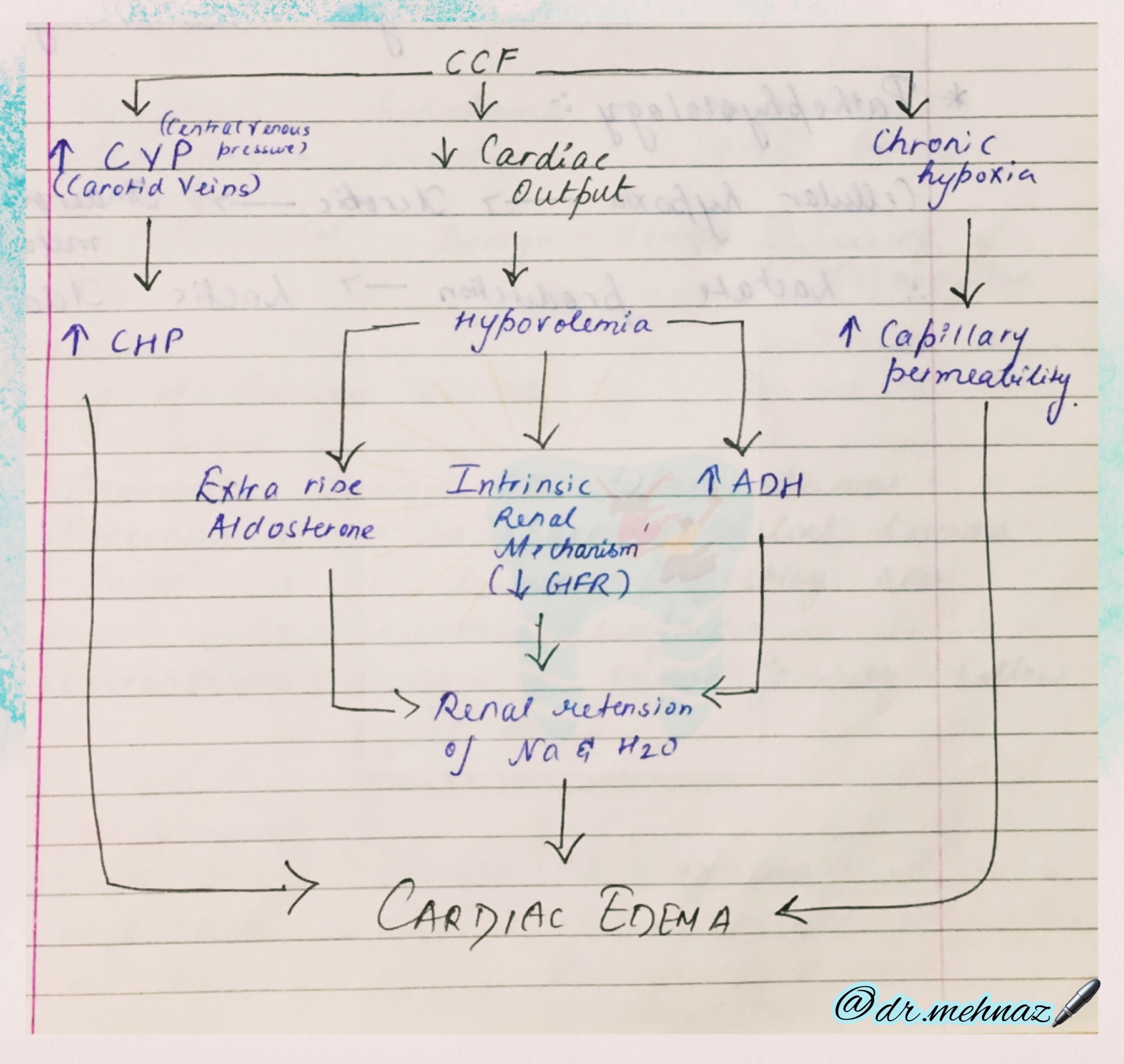
CCF: Congestive Cardiac Failure; CHP: Capillary hydrostatic pressure
CCF: Congestive Cardiac Failure; CHP: Capillary hydrostatic pressure
Link: https://drive.google.com/file/d/1UJ0ejZMn-KvpFL_Y5jmrx_hSel-acwlB/view?usp=drivesdk
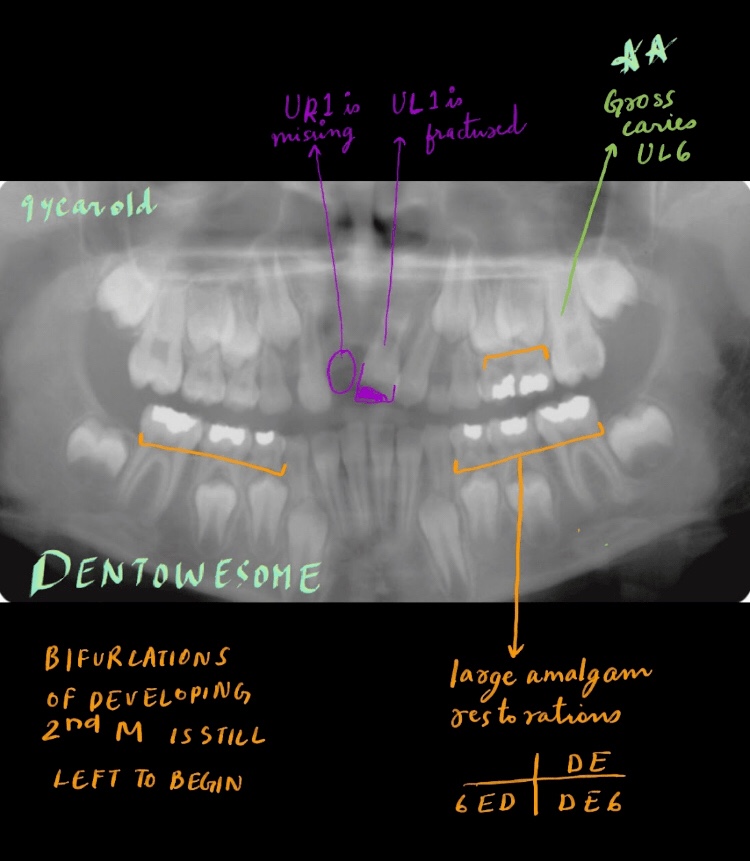
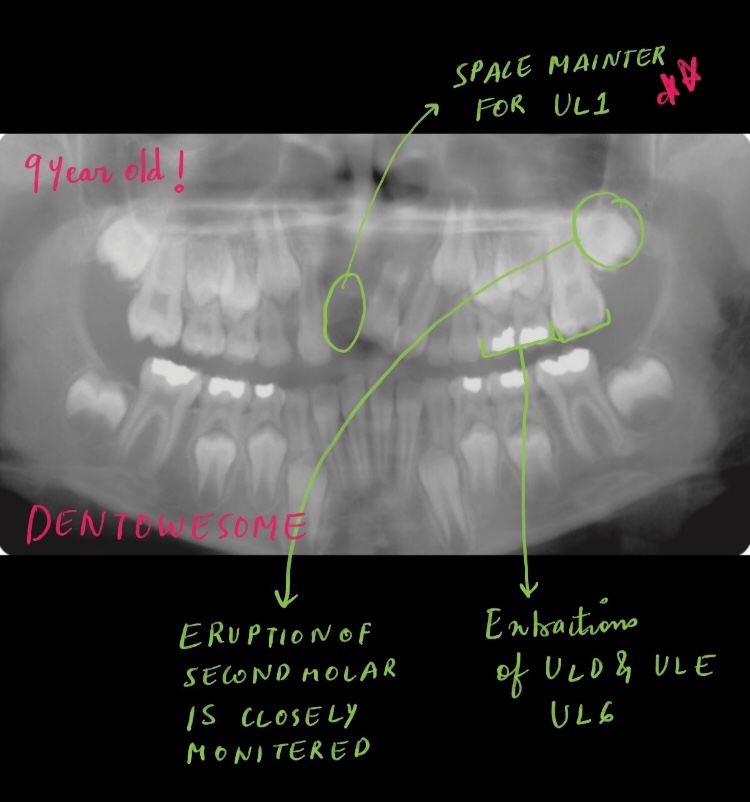
This child presented with significant pain in his upper left dental quadrant. He has an overjet of 8mm, a mild skeletal class II pattern and average vertical proportions, and is still sucking his thumb.
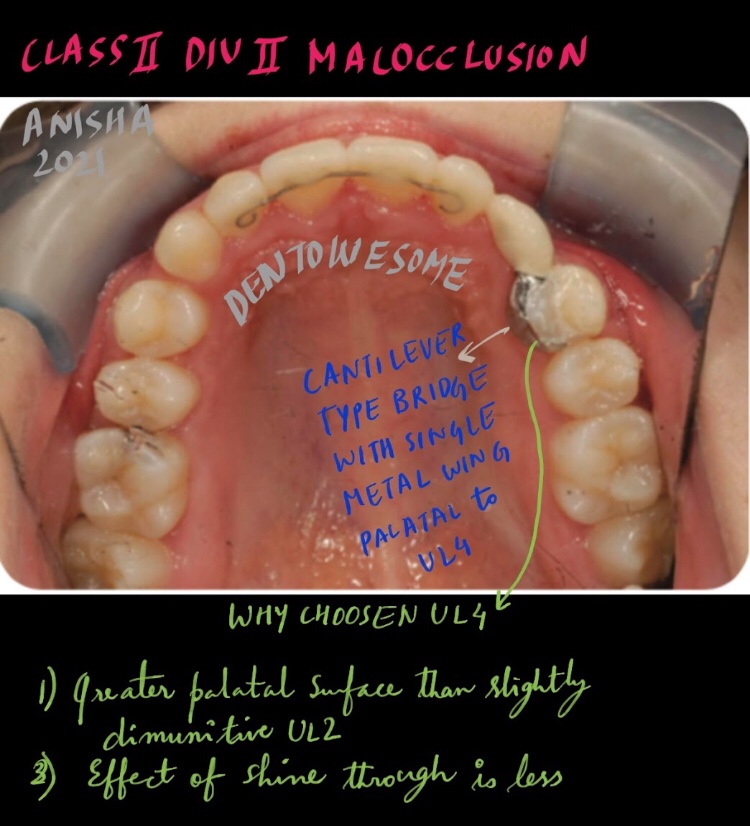
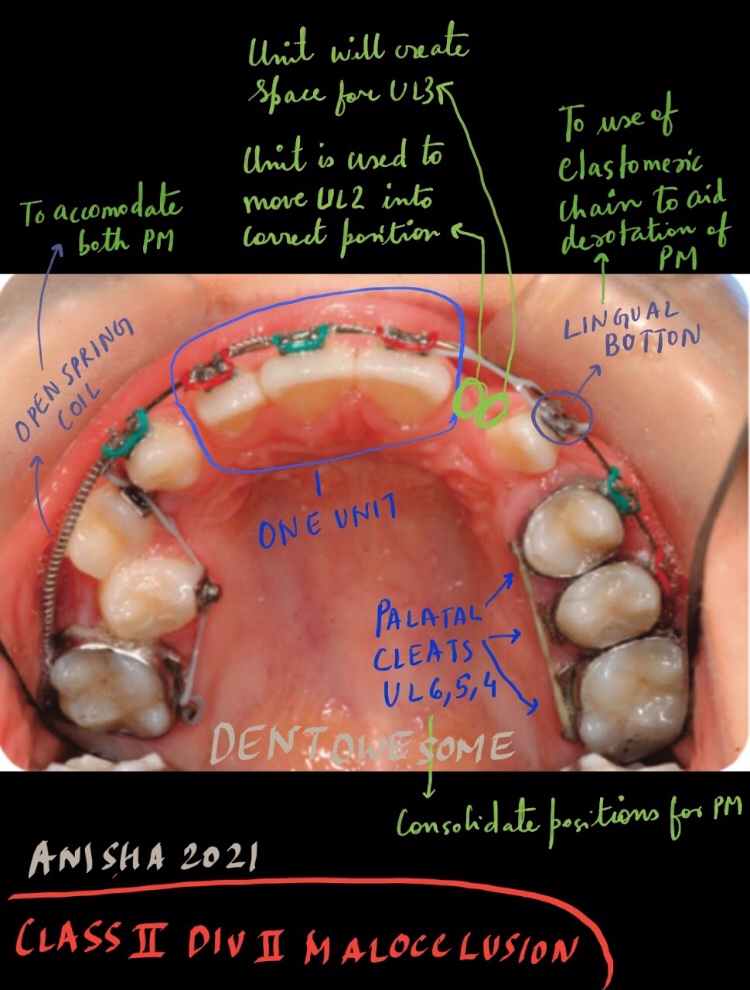
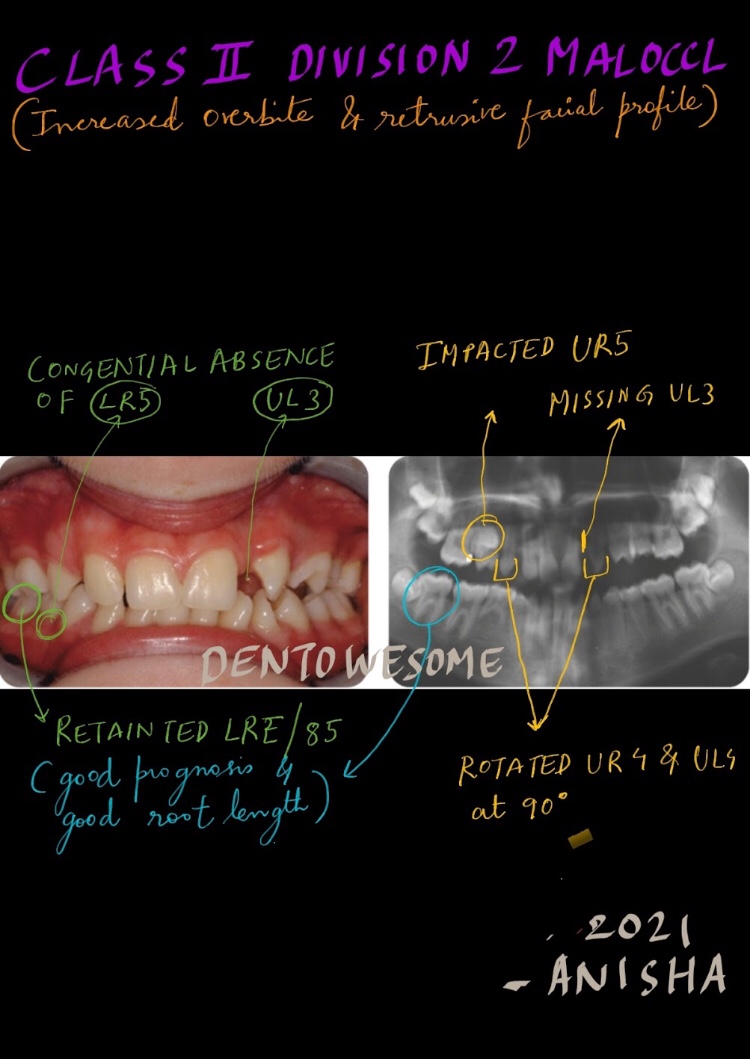
This 12-year-old female presented with a class II division 2 malocclusion on a moderate skeletal class II base with a retrusive profile and agenesis
Link: https://drive.google.com/file/d/1jzdkbvizdmQRovvsN2wBQ8KF42ePM9np/view?usp=drivesdk



PA radiolucencies identification made easy! Happy learning..😀📖
When formulating radiological differential diagnosis, features should be evaluated carefully, such as
• Location: With periapical inflammatory lesions, which are pathological conditions of the pulp, the epicenter typically is located at the apex of a tooth.
• Periphery: Ill defined
• Effects on surrounding structures: Periapical lesions cause widening of PDL space at apical region of the root.

PERIAPICAL RADIOLUCENCIES
Developmental
Lateral periodontal cyst

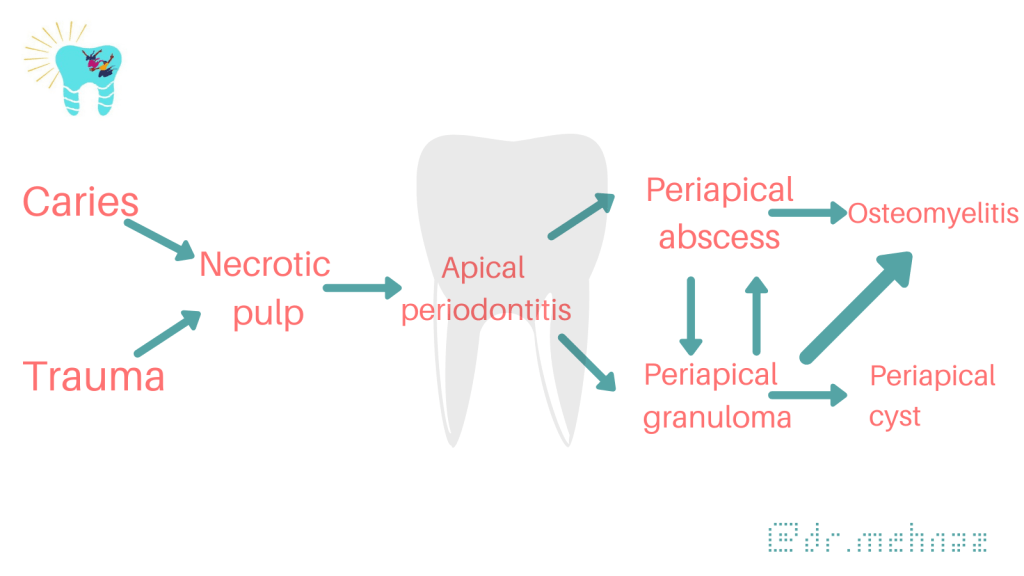
Inflammatory Lesions
Apical periodontitis, periapical abscess


Cystic Lesions
Periapical (radicular) cyst

Odontogenic keratocyst

Glandular odontogenic cyst
Benign Tumors
Ameloblastoma

Malignant Tumors
Ameloblastic carcinoma


Dentowesome|@drmehnaz🖊
References:
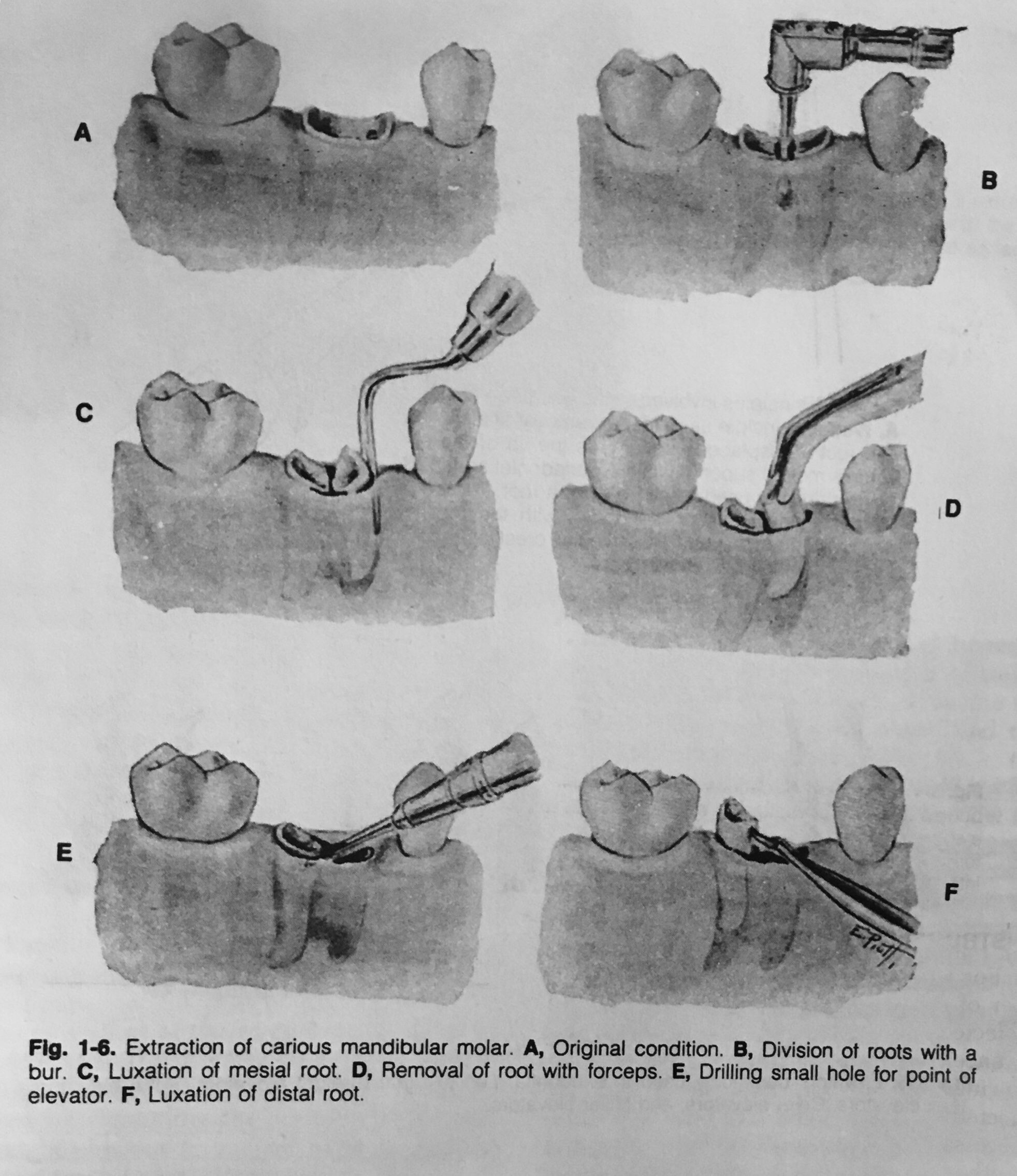
The extraction of a tooth requires the separation of its attachment to the alveolar bone via the crestal and principal fibers of the periodontal ligament. Also involved is a process of expanding the alveolar socket.
After the tooth has been removed, the form of alveolar process is restored by finger pressure. Bleeding is arrested by means of a pressure pack placed between the jaws, and the wound is allowed to fill with a blood clot.
The following techniques may be used for tooth removal:
Odontotomy can be used to facilitate any of these three procedures.

Dentowesome|@drmehnaz🖊
References: Textbook of Oral Surgery – Daniel M Laskin
1) https://pubmed.ncbi.nlm.nih.gov/8832476/
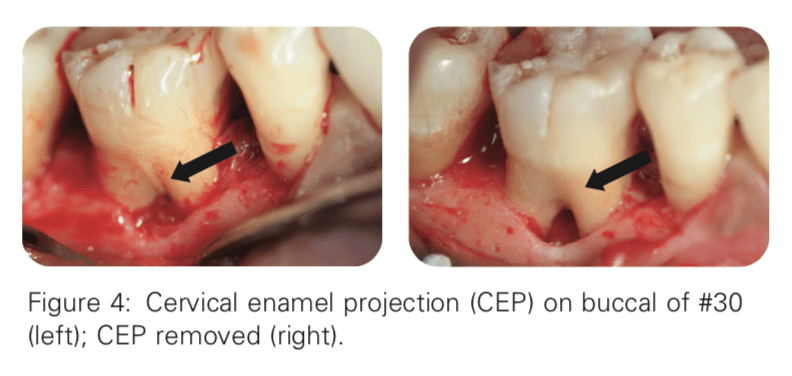
Masters and Hoskins reported that 90% of mandibular furcation invasions have CEPs
2) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2848791/
Bissada and Abdelmalek reported a 50% correlation between CEPs and furcation invasion
3) https://pubmed.ncbi.nlm.nih.gov/19518034/
The length of root trunk affects attachment loss The longer a given root trunk, the less likely a furcation will be predisposed to attachment loss. Teeth with Taurodontism usually have apically displaced furcation and longer root trunk length
4) https://pubmed.ncbi.nlm.nih.gov/13513891/
Intermediate bifurcation ridges are ridges spanning across the bifurcation of mandibular molars in the mesiodistal direction These ridges are present in 70–77% of the mandibular molars. Just like other anatomic structures, the presence of an intermediate bifurcation ridge may hinder effective plaque control and root preparation by both the patient and dentist
5) https://www.nature.com/articles/bdj.2007.1059
Buccal radicular grooves and palato-gingival grooves are developmental phenomena that affect mainly the maxillary anterior teeth. These grooves run on the roots in the coronal-apical direction Due to their anatomy, the grooves frequently provide a plaque-retentive area that is very difficult to instrument, making teeth with these developmental grooves more prone to attachment loss
A 47-year-old female presented with a chief complaint of: “My gums around one of the lower right teeth hurts.” The patient reported soreness and discomfort around tooth #30 from time to time, especially on the buccal side. On occasion, the patient experienced bleeding when brushing her teeth
LEARNING GOALS AND OBJECTIVES
To be able to identify local anatomic factors that may contribute to periodontal disease
To understand the anatomy of the furcation and root
To be able to diagnose a furcation invasion using a furcation classification system


LINK: https://drive.google.com/file/d/1R3qBKH78nqyZ-3Fe4YkvMJjsSbcG9EXw/view?usp=sharing
Sinus
Latin: Hollow (or) a bay
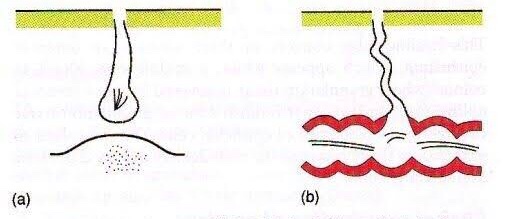
A sinus is a blind tract leading from the surface down to the tissue. There may be a cavity in the tissue which is connected to the surface through a sinus. The sinus is lined by granulation tissue which may be epithelized.
A sinus has one open draining end and the channel ends in a blind ending. An example would be a dental sinus draining from a dental abscess to either the inside of the mouth or the skin.

Fistula
Latin: flute(or) a pipe (or) a tube
It is a communicating tract between 2 epithelial surfaces commonly between hollow viscous & skin or between 2 hollow viscera. The tract is lined by granulation tissue which is subsequently epithelized. A fistula may be an abnormal communication between vessels.
An example would be from the mouth (oral cavity) to the skin surface, usually of the face or neck, and this specific type is called an orocutaneous fistula.


Fistulas and sinuses of the neck and face may be classified by cause.
Fistulas and sinuses due to developmental causes are usually present at birth.

Cysts are lumps in the skin containing fluctuant contents. They may have an opening to the skin surface.


In addition to careful history and examination, one or more of the following tests will usually be required to confirm the diagnosis and determine the cause:
Abscess
Collection of pus
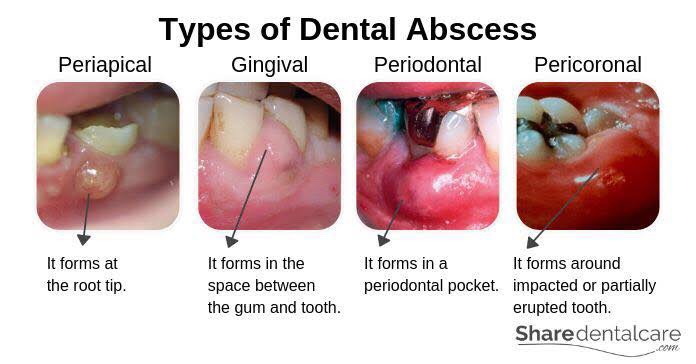
Features of acute inflammation; The four cardinal signs of inflammation are:
Diagnosis of Dental Abscess:
Dentowesome|@drmehnaz🖊
References:
