Link: https://drive.google.com/file/d/1AlKy20SM2P_xEjjtfEYtu_KoXKVPsa2D/view?usp=sharing
Between Portal and Systemic Veins. Sites are:
1. At the lower end of oesophagus – esophageal tributaries of left gastric vein ( portal) communicate with oesophageal tributaries of hemiazygous veins (systemic).
2. At the lower end of rectum and anal canal – superior rectal vein (portal) communicates with middle and inferior rectal veins (systemic).
3. Anterior abdominal (around umbilicus):
4. At bare area of liver – portal radicles of liver communicates with diaphragmatic veins (systemic)
5. At retroperitoneal site – the splenic and colic veins (portal) communicate with renal veins and other tributaries of IVC by small veins, called veins of Retzius.
6. At the fissure for ligamentum venosum, rarely, persistent ductus venosus establishes direct portocaval anastomosis (in fetal life, left branch of portal vein at the porta hepatitis communicates with IVC via ductus venosus. After birth, ductus venosus is fibrosed to form ligamentum venosum).
It consists of central arteriole from which numerous capillaries radiate, looks kike spider legs. Size varies from pinhead to 1-2 mm (sometimes cm). These are found along the area of SVC, commonly in neck, face, chest, and dorsum of hand and above nipple lines, cause of which is not known. It blanches on pressure, may pulsate if large. Better seen with glass slide or pinhead.
Causes of spider angioma:
1. Physiological:
2. Pathological:
Mechanism of spider angioma:
Differential diagnosis of spider angioma:
These are 2-3 cm lesions that occur on dorsum of foot, leg, back and lower chest. Caused by elevated venous pressure amd are usually found overlying the main tributary of large veins. Do not blanch on pressure and blood flow if from periphery to the center of lesion (opposite to spider angioma).
Redness in thenar and hypothenar eminence and pulp of fingers. Blanches of pressure. With glass slide, flushes synchronously with pulse. Causes of palmar erythema:
1. Physiological:
2. Pathological:
Mechanism of palmar erythema:
Reference: Clinical Medicine – ABM Abdullah
I hope you find the notes useful!
LINK: https://drive.google.com/file/d/1A-6UTN5TvHsDJtnkcDWz3aC1c-mNjsHM/view?usp=sharing

Hello friends, I hope you find these notes useful!
LINK: https://drive.google.com/file/d/19vBz6UBVOMA8vp3XMCkK8YAu9EtCgD8M/view?usp=sharing

Manjusha Madkaiker

Dental caries is a multifactorial irreversible microbial disease of the calcified tissues of the teeth, which is characterized by demineralization of the inorganic portion and destruction of the organic substance of the tooth, which often leads to cavitation. Dental caries is one of mankind’s ancient and longest disease associated with the oral profession. Everyday around 2.3 billion people are affected by dental caries.
But since the late 20th century with new advancement in technologies there is slow but gradual progress in the development of the vaccine .1972, a caries vaccine was said to be in animal testing in England.
DISEASE ETIOLOGY- A CHANGING TREND

1. Acidogenic theory – this theory was proposed by WD Miller in the year 1881 which states the combined effect of acid and oral microbes leads to the decalcification of tooth structure .This theory was incidentally evolved, and according to this theory the microbes in the oral cavity metabolize the dietary starch and lead to production of organic acids that hence dissolves the tooth structure .
2.Proteolytic Theory – Proposed by Pincus in the year 1949 which states that the proteolytic breakdown of dental cuticle is the first step in the various process. He proposed that Nasmyth’s membrane and enamel proteins are mucoprotein which are acted upon by the sulphates enzyme of the bacilli and yield sulphuric acid, this acid combines with the calcium of hydroxyapatite crystals and thus destroy the inorganic components of the enamel.
3.Protelysis-Chelation theory – Proposed by Schatz in the year 1955. Chelation is the process which leads to the formation of covalent bonds which leads to poorly dissociated and/or weakly ionised compound .Therefore dental caries are considered as the bacterial destruction of organic components of enamel and the breakdown products of these organic components to have chelating properties and thus dissolving the minerals in the enamel even at the neutral/alkaline pH.
HYPOTHESIS ON THE DEVELOPMENT OF DENTAL CARIES
1. Nonspecific plaque hypothesis
In the end of 19th century the cause of dental infection was said to be due to non-specific overgrowth of all bacteria in dental plaque this was called as the nonspecific plaque hypothesis given by Black in 1884 and Miller 1890. This hypothesis was proposed irrespective of the virulence of the bacteria.
So, the best way of disease prevention in the 19th century was non-specific mechanical removal of as much plaque as possible by e.g., tooth brushing or tooth picking.
The new advancements in the 20th century lead to to isolate and identify bacteria led which resulted in the abandoning of the NSPH. But mechanical plaque removal remained the most efficient way of preventing disease.
2.Specific plaque hypothesis
This hypothesis proposed by that the use of antibiotics against specific bacterial species could cure and prevent caries. However, results even today, are not very promising, the antibiotics reduced the abundance of cariogenic bacteria but failed to eliminate them thus as soon as the treatment was stopped, abundance increased while a long period of treatment leads to antibiotic resistance.
3.Ecological plaque hypothesis
4.Keystone pathogen hypothesis.
CARIES ICEBERG
1. On top i.e. the floating iceberg represents the clinical cases.
2. The submerged portion represents the carriers.
3. The part in the waterline represents the apparent and unapparent cases.
4. And at the tip are the ones with multiple health problems.
THE VACCINE
Vaccines are an immunobiological substance designed to produce specific protection against a given disease. It stimulates the production of a protective antibody and other immune mechanisms. Vaccines are prepared from live, inactivated or killed organisms, and toxoids.
Immune response is divided Into
1. Primary response
2. Secondary response (booster response)
Although development of a vaccine for started around 30 years back, but no success was achieved due various reasons.
But the formation of dental caries can be prevented or the progression can be slowed by the use of fluoride, use of sugarless products and sealants, and increased access to dental care have had a significant impact on the amount of disease in people. Many of these approaches can be broadly effective. Hence the dental caries can be reversible to a certain extend. However, economic, behavioural, or cultural barriers have continued the epidemic of dental disease.
Integrating the caries vaccine after its development into public health programs could be beneficial in bring dental caries to a minimal level.
It is an uninterrupted circle of protective lymphoid tissue at the upper ends of the respiratory and alimentary tracts.



Boundaries-
The pharynx is divided into 3 parts-
1.) Nasopharynx
2.) Oropharynx
3.) Laryngopharynx

Muscles of the pharynx-
1.) Longitudinal Muscles
2.) Circular Muscles

The space between the base of the skull and the superior constrictor is called as the pharyngobasilar fascia or the SINUS OF MORGAGNI.

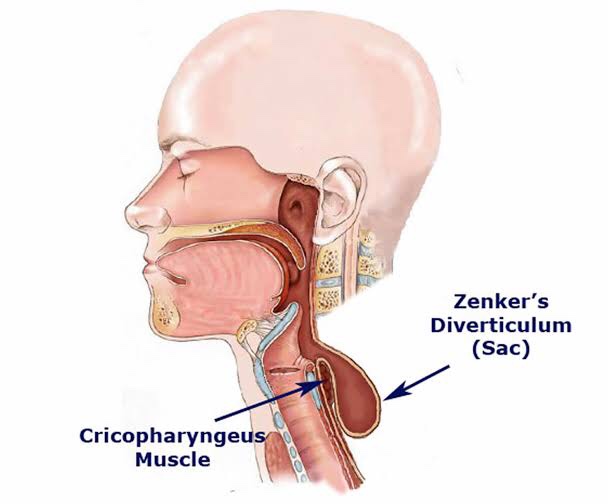
Killian’s dehiscence-
The inferior constrictor muscle splits into two- the stylopharyngeus and the cricopharyngeus.
The potential space between these two is called as the Killian’s dehiscence.

Incoordination in the area will lead to – ZENKER’S DIVERTICULUM.


GINGIVECTOMY
Gingivectomy means excision of the gingiva. By removing the pocket wall, gingivectomy provides visibility and accessibility for complete calculus removal and thorough smoothing of the roots, creating a favorable enviornment for gingival healing and restoration of a physiologic gingival contour.
Armamentarium:
Surgical Technique Steps:
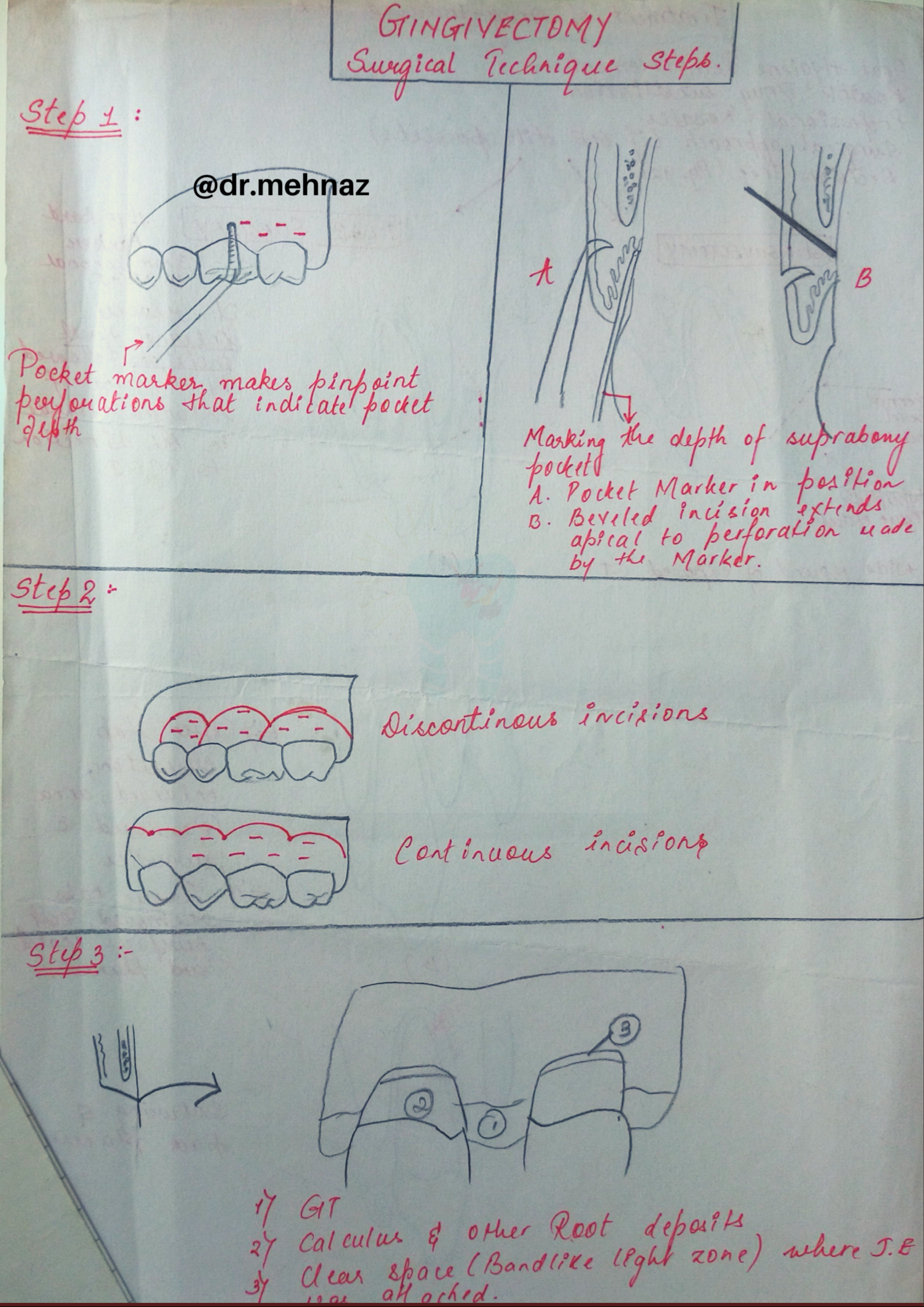
Step 1: The pockets on each surface are explored with a periodontal probe and marked with a pocket marker.
Step 2: The incision is started apical to the points marking the course of the pockets and is directed coronally to a point between the base of the pocket and the crest of the bone.
Step 3: Remove the excised pocket wall, clean the area, and closely examine the root surface.
Step 4: Carefully curette the granulation tissue, and remove any remaining calculus and necrotic cementum so as to leave a smooth & clean surface.
Step 5: Cover the area with a surgical pack.
Dentowesome|@drmehnaz🖊
Source: Carranza’s Clinical Periodontolgy, 10th Ed