Endodontic success is contingent upon meticulous debridement, shaping, and disinfection of the root canal system. Among the numerous factors influencing treatment outcomes, irrigation needle selection is an often-overlooked yet critical determinant of efficacy. The choice of needle gauge directly impacts the delivery of irrigants, ensuring optimal penetration, minimal apical extrusion, and maximal bacterial eradication. This article explores the scientific rationale behind needle gauge selection and its implications for clinical practice.
The Role of Needle Gauge in Endodontic Irrigation
Root canal irrigation serves multiple objectives: mechanical flushing of debris, dissolution of organic matter, microbial disinfection, and smear layer removal. The gauge of the irrigation needle determines the flow dynamics, pressure distribution, and depth of penetration within the canal. The ideal needle must navigate the complex anatomy of the root canal while facilitating efficient irrigant exchange without causing undue apical pressure.
Comparative Analysis of Commonly Used Needle Gauges
Gauge (G)
External Diameter (mm)
Clinical Considerations
21G
0.81
Rarely used due to excessive size and risk of irrigant extrusion
23G
0.64
Suitable for wide canals but limits depth of penetration
25G
0.51
Balances flow rate with controlled delivery
27G
0.39
Optimal for most cases; allows deeper penetration while minimizing extrusion
28G
0.36
Enhances precision for minimally invasive approaches
30G
0.30
Preferred for deep, narrow canals requiring delicate irrigation
Fluid Dynamics and Needle Design
The efficiency of irrigation is not solely dictated by gauge but also by the design of the needle tip. Side-vented needles, for example, reduce the risk of apical extrusion by directing flow laterally rather than apically. Additionally, advances in computational fluid dynamics have demonstrated that smaller gauge needles create more turbulent flow patterns, enhancing irrigant activation and biofilm disruption.
Advanced Irrigation Modalities: Beyond Traditional Needle Irrigation
While conventional needle irrigation remains the gold standard, emerging technologies aim to augment disinfection through enhanced fluid dynamics and activation mechanisms:
Ultrasonic and Sonic Activation: Agitates the irrigant to improve penetration into lateral canals and dentinal tubules.
Photoactivated Disinfection: Employs photosensitizers and light energy to generate reactive oxygen species for microbial eradication.
Electrochemically Activated Solutions (e.g., Sterilox): Generates hypochlorous acid and free chlorine radicals, enhancing antimicrobial efficacy while maintaining biocompatibility.
IntraLight UV Disinfection: Uses a 254 nm UV intracanal illuminator to eliminate residual microbial biofilms.
Clinical Implications and Future Directions
The evolution of endodontic irrigation strategies underscores the growing emphasis on precision-driven, minimally invasive techniques. While the 27-gauge needle remains the most widely adopted due to its balance of penetration and safety, ongoing research into fluid dynamics, antimicrobial solutions, and activation methods promises to redefine the standard of care.
As endodontic irrigation techniques continue to advance, the selection of an appropriate needle gauge must be guided by both anatomical considerations and the latest evidence-based protocols. A nuanced understanding of irrigation dynamics will not only improve disinfection efficacy but also contribute to superior long-term treatment outcomes.
Conclusion
Endodontics is no longer just about mechanical instrumentation; it is an interdisciplinary science integrating fluid mechanics, microbiology, and material science. The seemingly simple decision of needle gauge selection is, in reality, a critical component of treatment success. By refining our approach to irrigation, we can elevate endodontic outcomes, ensuring that root canal therapy is not only effective but also biologically sound.
Orthodontic treatment often requires space creation to align teeth properly. One effective way to achieve this is through molar distalization—moving the upper first molars backward to make room for crowding or to correct bite discrepancies. Traditionally, orthodontists have relied on headgear, Class II elastics, and removable appliances, all of which require patient compliance (and we all know how reliable that is! 🙄).
But what if there was a more predictable, fixed alternative?
Enter the Jones Jig Appliance—a fixed, non-compliance-based distalizing appliance designed to move molars efficiently without relying on patient effort.
How Does the Jones Jig Work?
✔ Palatal Button – A 0.5-inch diameter acrylic button, anchored to the maxillary second premolars using a 0.036-inch stainless steel wire for stability. ✔ Jones Jig Arms – One arm fits into the 0.045-inch headgear tube, while the other fits into the slot of the first molar band. ✔ Nickel-Titanium Spring – A 0.040-inch coil spring delivers a controlled force of 70-75 g to push the molars backward.
Once the Jones Jig is cemented, it is activated by tying the activation loop with a 0.010-inch ligature off the bracket of the anchoring tooth. This ensures continuous force application.
The coils are then reactivated every 4 to 5 weeks until the desired molar movement is achieved.
Once activated, the appliance applies a gentle but continuous distal force on the upper first molars, moving them backward over time. The best part? Since it’s fixed, patients don’t have to remember to wear it, making treatment more reliable.
Advantages of the Jones Jig
✅ No Patient Compliance Needed – Unlike headgear, patients don’t have to wear or adjust it. ✅ Continuous Force Application – The coil spring ensures a steady force for predictable movement. ✅ Faster Treatment Time – Studies show that molars can be distalized in 4-6 months.
While the Jones Jig is highly effective, it does come with some considerations: 🔹 Molar Tipping – Instead of bodily movement, molars may tip distally, requiring additional mechanics for uprighting. 🔹 Anchorage Loss – The anterior teeth may shift forward slightly, which may need to be controlled with TADs (temporary anchorage devices) or a transpalatal arch (TPA).
Does the Eruption of Second Molars Affect Treatment?
When using the Jones Jig Appliance for molar distalization, orthodontists must consider various factors that can influence treatment outcomes. One key question is: Does the eruption of second molars impact molar movement and anchorage loss?
A study evaluating 72 patients explored this question by comparing cases with erupted vs. unerupted maxillary second molars to determine how they affected the type and amount of molar movement and anchorage loss.
Study Findings: Second Molar Eruption and Its Effects
Researchers divided the patients into two groups:
Group
Condition of Second Molars
Key Observations
Group 1 (28 patients)
Unerupted second molars (below the cementoenamel junction of the first molar)
Less anchorage loss in premolars and incisors, potentially more controlled molar movement.
Group 2 (44 patients)
Erupted second molars (not banded or bonded)
More anchorage loss observed, possibly due to resistance from the second molars.
The presence or absence of second molars plays a significant role in the effectiveness of molar distalization. Patients with unerupted second molars may experience better molar movement with less anchorage loss, while those with erupted second molars may require additional anchorage support. In cases with erupted second molars, additional anchorage reinforcement (e.g., TADs or a transpalatal arch) may be necessary to prevent undesired movement.
Study Findings: How Far Did Those Molars Go?
A retrospective study of 72 patients using the Jones Jig showed:
Tooth Movement
Mean Change
Tipping Angle
Comparison to Other Appliances
Maxillary First Molar
2.51 mm distal movement
7.53° distal tipping (meaning they didn’t just move—they leaned back like someone dodging responsibility. 😅)
Similar to Herbst, Wilson Mechanics, and Pendulum Appliance 📏
Maxillary Second Molar
1.79 mm distal movement (Not as much as the first molar, but still making progress! 🔄)
8.03° distal tipping (tipped even more than first molars)
0.71 mm extrusion observed 📉 (suggests that second molars are like that one friend who always stands out in group photos. 📸)
Overjet
Increased 0.45 mm
If necessary, J-hook headgear or Class II elastics can help maintain anchorage.
2.21° incisor proclination
(much less than the 6° seen in other studies. So, while there’s some flaring, it’s not enough to make your patient look like Bugs Bunny. 🐰)
Less flaring than with Pendulum & Repelling Magnets 😎
Less than the 1.30 mm increase seen with the Pendulum appliance and the 1.60 mm increase with repelling magnets.
Overbite
Decreased 1.28 mm
—
Improved vertical control compared to other appliances 📊
Anchorage Control: Because We Don’t Want Molar Tipping Running the Show
Distalizing molars is great, but uncontrolled tipping? Not so much. Here’s where anchorage control steps in like a responsible chaperone at a high school dance.
✅ Use a Nance holding arch, utility archwire, or stopped archwire to keep those molars in check. ✅ Short Class II elastics can help move the premolars and incisors back once the molars are in position. ✅ J-hook headgear can reinforce anchorage (for the brave souls who still prescribe it).
Molar Extrusion: Is It a Big Deal?
One concern with distalization is molar extrusion—but does the Jones Jig make teeth “float away”? Not really.
🔹 Jones Jig Patients:
Males:3.17 ± 1.79 mm of extrusion
Females:1.33 ± 1.38 mm of extrusion
🔹 Untreated Class I Patients (for comparison):
Males:4.1 ± 3.1 mm
Females:1.9 ± 2.2 mm
📌 Takeaway? The extrusion in Jones Jig patients is within normal growth changes. So, unless your patient is trying to float their molars into the stratosphere, this isn’t a major concern. 🚀
Jones Jig vs. Headgear: Any Real Difference?
The study found no statistically significant differences between the Jones Jig group and a matched Headgear groupwhen evaluating:
✅ Maxillary first molar position ✅ Maxillary central incisor angulation ✅ Linear position of incisors ✅ Overjet & Overbite changes
So, if you’re an orthodontist who loves avoiding unnecessary patient lectures about compliance, the Jones Jig might be your new best friend. 🎉
Treatment Comparison: Who Wins?
Treatment Modality
Patient Compliance Needed?
Molar Distalization (mm)
Overjet Change (mm)
Overbite Change (mm)
Jones Jig Appliance
❌ No compliance needed
2.51 mm
+0.45 mm
-1.28 mm
Cervical Headgear
✅ Requires compliance 😬
2.50 mm
+0.40 mm
-1.30 mm
Class II Elastics
✅ Requires compliance 🙄
Varies (depends on use)
Greater risk of overjet increase
Less predictable molar control
📌 Takeaway? The Jones Jig does everything headgear does—without the compliance drama. It’s like getting straight A’s without ever studying (if only life worked that way 😆).
Final Verdict: Is the Jones Jig Worth It?
✔ YES! If you want a fixed, predictable, non-compliance-dependent way to correct Class II malocclusions, the Jones Jig is a great choice.
✔ Same results as headgear—without the teenage rebellion.
✔ Minimal anchorage loss compared to other distalization appliances (no crazy overjet increase).
✔ Less annoying for patients = less annoying for you. 😆
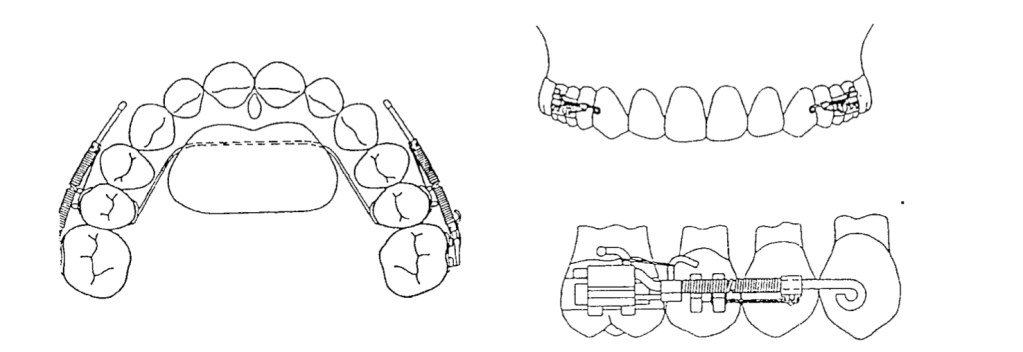
Orthodontics has long relied on mechanical devices to refine tooth movement and optimize jaw alignment. Among these, the face-bow remains an essential tool for controlled force application. Recent experimental and theoretical studies have focused on enhancing face-bow designs to achieve unilateral distal forces more efficiently. This post synthesizes key findings regarding the efficacy of various face-bow configurations, addressing their theoretical underpinnings and practical implications for advanced orthodontic care.
Comparative Analysis of Face-Bow Designs
Face-Bow Type
Key Features
Force Distribution
Resulting Forces
Swivel-Offset Face-Bow
– Outer bow attached eccentrically via a swivel joint.- Allows lateral movement of the outer-bow tips.
– Delivers unilateral force with predictable lateral forces.- Effective for asymmetric treatment.
Symmetrical Face-Bow
– Outer bow symmetrically aligned.- Balanced force application.
– Even force distribution on both sides.- No lateral force generated.- Ineffective for unilateral force delivery.
– No unilateral or lateral forces delivered.
Soldered-Offset Face-Bow
– Rigid attachment of outer bow on one side.- Appears asymmetrical but does not deliver unilateral forces.
– Symmetrical force distribution.- No lateral force generated.
– No unilateral force delivered.
Spring-Attachment Face-Bow
– Spring on one terminal of the inner bow.- Symmetrical outer-bow tips.
– Equal force on both sides.- No lateral force generated.
– No unilateral force delivered.
Which Face-Bow Designs Effectively Deliver Unilateral Distal Forces?
Not all face-bow designs are capable of delivering sufficient unilateral distal forces, an essential factor for treating conditions such as unilateral posterior crossbites or asymmetrical dental arch development. The following analysis highlights the effectiveness of different face-bow configurations:
Ineffective Designs:
Bilaterally Symmetrical Face-Bows: These designs maintain equal force distribution on both sides, making them unsuitable for unilateral force application.
Spring-Attachment Face-Bows: Despite their versatility, these face-bows fail to concentrate force on a single side, limiting their application in unilateral treatments.
Soldered-Offset Face-Bows: While superficially asymmetrical, the rigid attachment of the outer bow does not result in the necessary unilateral force distribution.
These designs consistently failed to generate a mean unilateral distal force exceeding 60%, thereby limiting their clinical utility for unilateral orthodontic applications.
Effective Designs:
Power-Arm Face-Bows: These designs effectively direct unilateral forces, achieving greater than 60% of the force distribution to one side, which aligns with clinical requirements for unilateral force application.
Swivel-Offset Face-Bows: By incorporating a swivel mechanism, these face-bows create asymmetry, allowing for targeted distal force delivery to one side.
Both of these designs surpass the 60% threshold for unilateral force distribution, thus meeting the criteria for effective treatment.
Theoretical Framework for Unilateral Force Delivery
The key to effective unilateral force application lies in the asymmetry of the face-bow’s design. When the outer-bow tips are positioned asymmetrically relative to the midsagittal plane of the inner bow, it allows for the focused application of force on one side:
Asymmetrical Designs: These designs facilitate targeted force delivery by creating a mechanical advantage that directs the force to one side. This results in the efficient application of unilateral distal forces, which is essential for treating asymmetric dental and skeletal issues.
Symmetrical Designs: These configurations fail to produce unilateral forces because the force is evenly distributed, thus making them ineffective for unilateral applications.
The swivel-offset face-bow achieves this asymmetry through a lateral swing of the outer-bow terminals, while power-arm face-bows, when constructed with comparable geometric patterns, similarly exhibit the necessary force distribution for unilateral applications.
Characterization of Lateral Forces in Unilateral Face-Bows
Unilateral face-bows not only generate distal forces but also produce lateral forces that contribute to the overall mechanical effect. These lateral forces are characterized by the following:
Directionality: The lateral force is directed from the side receiving the greater distal force toward the opposite side, ensuring balanced correction of dental and skeletal asymmetries.
Magnitude: The magnitude of the lateral force increases with the unilateral effectiveness of the face-bow, making it a predictable variable in effective designs.
Predictability: Experimental studies demonstrate that lateral forces are highly predictable in effective designs, such as the power-arm and swivel-offset face-bows, whereas they are erratic and difficult to control in symmetrical, ineffective designs.
Practical Considerations for Clinicians: Which Face-Bow Design is Optimal?
While both the power-arm and swivel-offset face-bows are effective in delivering unilateral distal forces, the power-arm design stands out in terms of practicality and clinical efficiency:
Ease of Fabrication: The power-arm face-bow can be easily modified chairside from a conventional face-bow, offering flexibility and reduced chair time for both clinicians and patients.
Predictable Performance: Experimental data show that the power-arm design provides a force distribution that closely matches that of the swivel-offset face-bow, with less than a 5% difference in performance.
Patient Comfort: The power-arm design ensures more consistent force application, contributing to better patient comfort and compliance during treatment.
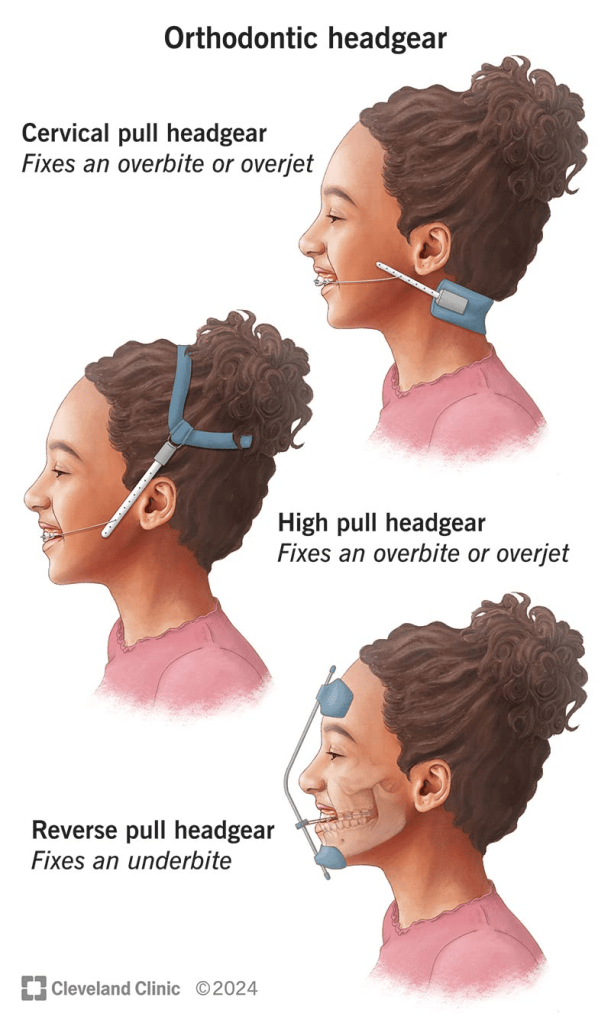
Class II malocclusions are a common orthodontic challenge, often requiring precise management of maxillary dentition to achieve ideal outcomes. Extraoral forces, such as those applied via headgear, have long been used to either distalize upper molars or restrict their forward migration. Understanding the physics behind these forces and their application is key to maximizing treatment efficacy and minimizing undesirable side effects.
Orthodontic forces can be represented as vectors, which help visualize the direction and magnitude of applied forces. When multiple forces converge on a tooth, a resultant vector can be calculated. This resultant vector can then be resolved into components parallel and perpendicular to the tooth axis, allowing for precise analysis of force magnitudes in these directions. This fundamental principle of physics underpins the design and application of combined headgear, which uses cervical and high-pull vectors to achieve targeted outcomes.
One of the critical considerations in orthodontic treatment is the direction of applied forces. Studies show that molars tipped back during distalization tend to relapse quickly unless occlusal forces act to upright them. For bodily movement of upper molars, force must be applied through the center of resistance. Cervical headgear, which applies forces below the center of resistance, can cause extrusion of upper molars and an undesirable opening of the mandible. Conversely, occipital traction—preferred for patients with open bite tendencies—is less effective in altering maxillary structures anteroposteriorly.
Addressing Challenges with Combined Headgear
The limitations of traditional cervical and high-pull headgear in treating Class II malocclusions with high mandibular plane angles necessitate alternative approaches. Combined headgear, which integrates forces from both cervical and high-pull vectors, offers a promising solution. By optimizing the resultant force vector, combined headgear can:
Minimize molar extrusion.
Reduce the likelihood of mandibular plane angle alterations.
Improve anteroposterior control of maxillary structures.
Evidence Supporting Combined Headgear
Research highlights the potential of combined headgear to address the shortcomings of single-vector approaches. For instance, bending the outer arms of cervical headgear downward by 15° has been shown to reduce extrusion. Moreover, studies by Baumrind and colleagues suggest that mandibular plane angle remains stable when combined headgear is used, likely due to the balanced application of forces.
This study examined three treatment groups, each using a different force ratio: 1:1, 2:1, and 1:2.
Treatment Group
Force Adjustment (High-Pull : Cervical)
Inner Bow Expansion
Wear Time
Treatment Duration
1:1
150 gm per side : 150 gm per side
Not expanded
20 hours/day
2 to 9 months
2:1
200 gm per side : 100 gm per side
Not expanded
20 hours/day
3 to 7 months
1:2
100 gm per side : 200 gm per side
Not expanded
20 hours/day
2 to 7 months
The goal? To understand how these variations impact the displacement of the maxilla and mandible, molar positioning, and even occlusal plane inclination. Here’s what they found.
Changes Through the Treatment
Parameter
1:1 Treatment Group
2:1 Treatment Group
1:2 Treatment Group
ANB Angle
Significant decrease
Significant decrease
Significant decrease
SNB Angle
Significant increase
Significant increase
No significant change
SN/GoGn
No significant change
Significant decrease
No significant change
SN/OP
No significant change
Significant increase
Significant decrease
Upper Molar/ANS-PNS (Angle)
No significant change
No significant change
Significant decrease
Upper Molar/ANS-PNS (mm)
Significant decrease
Significant decrease
Significant increase
Lower Molar MP (mm)
Significant increase
No significant change
No significant change
Maxillary and Mandibular Displacement
In the third treatment group, with a 1:2 force ratio, the maxilla was displaced backward. Interestingly, this aligns with findings from previous studies by O’Reilly and Boecler, who observed similar effects with cervical headgear. However, the mandible’s forward growth remained consistent across all groups, resulting in no significant differences in the ANB angle. This reinforces the idea that headgear’s primary role is in influencing the maxilla rather than the mandible.
Upper Molar Movement
Now, let’s talk molars. Superimposition analyses showed that the upper first molar was distalized by 3.6 to 4.0 millimeters across all groups. This distalization played a significant role in correcting molar relationships. However, the type of headgear affected how these molars moved. For example, high-pull headgear resulted in greater horizontal displacement, as noted by Baumrind et al., while cervical headgear tended to cause more vertical changes.
Occlusal Plane Inclination
One fascinating finding was the tipping of the upper molars. In the third group, there was a significant decrease in angulation and a mesial displacement of the molar apex. This aligns with Baumrind’s observations and highlights how force direction can influence tooth movement. Meanwhile, Badell’s study on combined headgear treatments showed a notable distal tipping, which was less pronounced in other groups.
Vertical changes were also noteworthy. In the 1:2 group, the downward force component caused molar extrusion, a pattern commonly seen with cervical headgear. Conversely, the 1:1 and 2:1 groups showed molar intrusion, consistent with high-pull headgear studies. This difference in vertical displacement also impacted the occlusal plane. The second group, with a 2:1 force ratio, showed a significant increase in occlusal plane inclination, mirroring findings from Badell and Watson.
Mandibular Plane Angle (MP)
Beyond the teeth, headgear also influences skeletal structures. The mandibular plane angle—a key indicator of vertical facial growth—remained largely unchanged in the 1:2 group, likely due to a modest increase in ramus height. However, the second group showed a significant decrease in the SN/Go-Gn angle, suggesting a more pronounced impact on vertical growth patterns.hames et al. and Badell, highlighting the interplay between force systems and vertical growth patterns.
Intercanine Width
And finally, let’s touch on intercanine width. Mitani and Brodie’s research showed an increase in this variable with cervical headgear, and this study confirmed those findings. The third group, with the greatest distalization, exhibited the most significant increase in intercanine width, highlighting the interplay between molar movement and arch expansion.
So, what’s the takeaway? Headgear therapy is a versatile and effective tool, but its outcomes depend heavily on the force system used. From molar distalization to occlusal plane changes, every detail matters. This study not only builds on decades of research but also underscores the importance of tailoring treatment to individual patient needs.
Orthodontic philosophies, much like those in medicine, tend to swing with the pendulum of trends and innovations. In the medical field, we’ve seen treatments rise and fall in popularity—antihistamines were once heralded as a cure-all, and antibiotics became the go-to for nearly every ailment. Similarly, in orthodontics, we’ve witnessed an evolving landscape of treatments and tools: non-extraction versus extraction approaches, debates over which teeth to extract, and a constant shift between fixed and removable appliances. Each innovation, from square tubes to round tubes and from labial to lingual appliances, has had its moment in the spotlight.
In this article we will explore: What is the role of the extra-oral appliance? Where does it find use? What are its limitations? How valid are the multiplicity of claims made for it?
The use of extraoral appliances isn’t new. As early as 1887, Dr. Edward Angle, a pioneer in orthodontics said “The value of the occipital bandage is, I believe, becoming more and more appreciated, and is especially applicable in this class of cases [meaning maxillary protrusions]. I am using the appliance . . . in my 16th case, and I consider it much more satisfactory than any of the few devices described in our literature on the subject.”
Investigating the Facts: A Study of 150 Cases
In a detailed study of 150 Class II, Division 1 malocclusions, headplates and plaster casts were analyzed to assess the role of extraoral force. Among these cases, 107 exhibited normal mandibular arch form, tooth size, and basal bone relationships. These findings suggest that in many cases, the mandibular arch is not the primary culprit in malocclusion; rather, the anteroposterior discrepancy lies in the maxilla. This raises an important question: Should orthodontic therapy target the maxilla while leaving the mandibular arch undisturbed?
The clinical reality supports this approach. Prolonged Class II therapy directed at the mandibular arch often results in unwanted tipping or forward sliding of the lower teeth. By focusing forces on the maxilla, we may achieve better results, including improved tooth interdigitation, reduced overbite and overjet, and restored muscle function and facial aesthetics.
The Debate Around Extraoral Force
The literature on extraoral force is filled with conflicting claims. Some argue that it restricts maxillary growth, while others suggest it only affects alveolar growth. There are debates about whether it moves teeth bodily or merely tips them, and whether it allows the mandible to grow forward or simply frees occlusal interferences. Even the choice of appliance—headgear versus cervical bands—sparks disagreement.
To bring order to the conflicting claims about extraoral appliances, we must approach the topic with objectivity. What truly happens in a controlled group of cases? Which cases benefit most from extraoral force, and where does it fall short? By critically evaluating both successes and failures, we can better understand the indications, contraindications, and unanswered questions surrounding this treatment modality.
The appliance used consisted of molar bands, an .045 stainless steel labial arch wire with vertical spring loops at the molars, and continuous loops at the lateral canine embrasures to receive the cervical gear. The cervical gear featured a metal tube with a continuous internal spring to provide distal motivating force. In select cases, incisors were banded at certain stages of therapy.
Patients were categorized into three age groups to analyze outcomes based on developmental stages:
Deciduous dentition: 3 to 6 years
Mixed dentition: 7 to 10 years
Permanent dentition: 11 to 19 years
This stratification allowed for a nuanced understanding of how age and dentition stage influenced treatment outcomes.
The study revealed several key insights, supplemented by observations from routine practice where extraoral anchorage was employed in diverse scenarios. These included:
Bolstering anchorage during full edgewise therapy
Closing spaces created by distal movement of anterior teeth
Uprighting individual teeth
Serving as an active retainer
The study confirmed that Class II, Division 1 cases vary significantly, even when focusing on three core characteristics:
Maxillomandibular basal relationship
Overjet
Overbite
The severity of discrepancies across these factors, combined with patient-specific variables such as morphogenetic patterns, motivation, cooperation, and growth during therapy, made the prognosis unpredictable. Success or failure was influenced by the degree of deviation from the norm in each factor and the interplay between them.
Can extraoral force alone, directed against the maxilla, correct Class II, Division 1 malocclusions?
The goal of establishing normal tooth interdigitation, eliminating excessive overbite and overjet, and restoring muscle function and appearance is ambitious. Achieving these outcomes universally is contingent on numerous factors:
Hereditary patterns
Age and sex of the patient
Presence or absence of third molars
Growth increments during treatment
Patient cooperation
Deciduous Dentition Group (3 to 6 years)
Sample Size: 14 cases, all selected for their severity, characterized by significant basal dysplasias.
Residual Class II relationship: Persisted in over half the cases, though to a lesser degree.
Basal adjustment: Anteroposterior basal adjustment was observed in 11 out of 14 cases.
Muscle function: Most patients exhibited improved muscle tone and function, along with a reduction in abnormal muscle habits.
Overjet correction: Often led to excessive lingual tipping of maxillary incisors, especially in cases without pre-existing spacing.
Overbite correction: The least satisfactory aspect of treatment.
Mixed Dentition Group (7 to 10 years)
Sample Size: 50 cases (34 girls, 16 boys).
Outcomes:
Normal molar relationship: Achieved in 29 cases, though not always accompanied by normal canine relationships.
Overjet correction: Similar to the deciduous group, excessive lingual inclination of maxillary incisors was noted in some cases.
Vertical correction: More pronounced and successful compared to the deciduous group.
Severe discrepancies: Cases with the greatest deviation from normal in basal relationship, overbite, and overjet showed the least favorable results.
Case Examples
Patient A.L.
Presented with severe basal malrelationship, marked overjet, and normal overbite.
Outcome: Immediate and gratifying response due to anterior spacing and lack of excessive overbite.
Patient J.K.
Presented with a similar profile but without anterior spacing.
Outcome: Removal of maxillary second molars facilitated mesiodistal adjustment, resulting in successful correction across all parameters.
Permanent Dentition Cases
Sample Size: 36 cases (19 boys, 17 girls)
Growth Correlation: A clear link was observed between the pubertal growth spurt and positive response to mechanotherapy.
Outcomes:
25 patients responded well enough to eliminate Class II characteristics, achieving normal interdigitation and improved aesthetics.
Success was highly dependent on a combination of favorable growth, patient cooperation, and other individual factors.
Can Extraoral Force Achieve Bodily Distal Movement of Maxillary Teeth?
The ability of extraoral force to influence maxillary growth, move teeth bodily distal, or merely tip them distally has been a subject of debate.
Maxillary Growth
Observation: There is no evidence that maxillary growth, as governed by sutures, is significantly affected by extraoral force. Claims of growth inhibition require substantiation, which is currently lacking.
Alveolar Growth: However, maxillary alveolar growth can be influenced. Changes in the anteroposterior apical base relationship are among the most significant findings, as demonstrated by cases like Patient A.M.
Distal Movement of Maxillary First Molars
Controversy: The possibility of bodily distal movement of maxillary first molars remains contentious. While some authorities categorically deny this, evidence from the study suggests otherwise:
Cases Supporting Movement:
Bodily distal movement has been observed in some cases, though it is not the norm.
Occasionally, this movement occurs unpredictably or can be facilitated by the removal of maxillary second molars during active treatment (Figs. 8 and 9).
Normal Path Restriction: In most cases, extraoral force restrains the maxillary first molar from moving forward along its natural path or tips it distally.
Challenges with Tipping
Excessive Distal Tipping: One drawback of extraoral appliances is the tendency for excessive distal tipping of maxillary first molars.
Mitigation Strategies:
Allowing maxillary second molars to erupt before treatment.
Removing maxillary second molars during treatment.
Using bands or Rocky Mountain-type crowns on second deciduous molars instead of first permanent molars in the mixed dentition stage.
Employing a headcap instead of cervical gear, as the headcap is associated with reduced tipping tendencies.
Does Extraoral Force Tip Maxillary Incisors Lingually, Moving Apices Labially?
Yes, extraoral force can cause lingual tipping of the maxillary incisors, with their apices potentially moving labially. This effect is a notable concern in orthodontic treatment, particularly in cases with significant basal discrepancies.
Lingual Tipping of Maxillary Incisors:
Lingual tipping is a frequent outcome when extraoral force is applied, especially in attempts to correct overjet in cases with marked maxillomandibular basal dysplasia.
This tipping often results from the inability to fully eliminate the basal malrelationship.
Overjet Correction Challenges:
Correcting overjet in the presence of basal discrepancies often necessitates:
Excessive lingual inclination of maxillary incisors.
Excessive labial inclination of mandibular incisors.
A combination of both adjustments.
These compromises are sometimes unavoidable to achieve acceptable occlusal and esthetic outcomes.
Between the two options, lingual tipping of maxillary incisors is considered the lesser compromise compared to labial tipping of mandibular incisors.
Does Extraoral Force, Directed Against the Maxillary First Molar, Impact Maxillary Second or Third Molars?
The impact of extraoral force on the maxillary second and third molars cannot be definitively answered with a simple “yes” or “no.” However, clinical observations and studies provide insights into potential effects:
Temporary Impact on Second Molars:
Excessive distal tipping of the maxillary first molars due to extraoral force can temporarily affect the eruption path of the maxillary second molars.
Once the distal force is removed, the first molars typically upright themselves, allowing the second molars to erupt.
Crossbite and Eruption Issues:
In some cases, maxillary second molars have been observed to erupt buccally, resulting in crossbite.
While it is not definitively proven that this is caused by extraoral force, there is a strong likelihood of a connection.
Non-Eruption Cases:
Four documented cases showed non-eruption of maxillary second molars following extraoral mechanotherapy.
This suggests that extraoral force may sometimes inhibit the eruption of the second molars, likely due to changes in the eruption path or space limitations.
Impact on Third Molars:
The diversion of the second molar’s eruption path could also influence the eruption of the maxillary third molars, though this requires further investigation.
Space Limitation in the Alveolar Trough:
Observations indicate that the alveolar trough may have limited capacity. If space is consumed by distal movement or tipping of the first molars, it may affect the eruption and alignment of second and third molars.
Growth and Timing in Class II Correction
Importance of Growth:
Growth is a critical factor in addressing Class II discrepancies. Successful treatment often relies on leveraging the pubertal growth spurt to maximize skeletal and dental changes.
The maxillary alveolodental complex can be restrained during growth, allowing for a more favorable adjustment of the anteroposterior relationship with minimal reliance on tooth movement.
Optimal Age for Treatment:
Girls: Best results observed between 10 to 13 years.
Boys: Optimal outcomes seen between 12 to 17 years.
Exceptional cases, such as a 19-year-old boy with significant mandibular growth during a late growth spurt, demonstrate the variability of growth potential.
Uncertainty of Growth:
While growth is pivotal, its predictability remains a challenge. The degree of mandibular growth and its impact on correcting Class II malocclusions vary significantly between individuals.
Unilateral Response to Extraoral Force
Observation of Unilateral Effects:
In some cases, unilateral response to extraoral force was noted, particularly in the canine region. This posed challenges in achieving bilateral symmetry.
Contributing Factors:
Sleeping Position: Patients reported consistently sleeping on one side, which appeared to correlate with reduced movement on that side.
Chewing Habits: Favoring one side during eating may also contribute to unilateral response, though this remains inconclusive.
Management Strategies:
In some cases, a lower lingual appliance was used to provide additional elastic traction, helping address asymmetry. However, unilateral response persisted in certain cases.
Challenges in Achieving Complete Correction
Residual Discrepancies:
Even with significant improvement in overjet and molar relationships, Class II characteristics in some segments, particularly the buccal region, may remain unresolved
Future Considerations:
The causes of unilateral response and incomplete correction remain areas for further research and clinical focus. Factors such as patient compliance, growth variability, and appliance design must be studied in greater detail.
Does Extraoral Force Free Occlusal Interferences, Stimulate Forward Mandibular Positioning, or Promote Mandibular Growth?
The effects of extraoral force on occlusal interferences, mandibular positioning, and growth remain a topic of debate. The current evidence provides insights but lacks conclusive proof for some claims.
Freeing Occlusal Interferences:
Extraoral force can alter inclined plane relationships between maxillary and mandibular teeth.
In cases of mandibular overclosure caused by occlusal interference, combined extraoral force and bite plate therapy can effectively eliminate functional retrusion.
However, functional retrusions are less frequent and less severe than previously believed.
Stimulating Forward Mandibular Positioning:
Claims that extraoral force promotes forward mandibular positioning via a neurogenic reflex posture mechanism lack robust evidence.
While such repositioning cannot be categorically dismissed, it has not been consistently demonstrated under controlled, biometric conditions.
Stimulating Mandibular Growth:
There is no conclusive evidence that extraoral force or any orthodontic appliance can stimulate mandibular growth beyond the individual’s inherent morphogenetic pattern.
Apparent acceleration or increased growth rates reported in some studies (e.g., guide planes) have not been reliably duplicated in controlled experiments, such as those conducted at Northwestern University.
Class II to Class I Transformation:
Eliminating distal displacement through extraoral force does not result in the transformation of a Class II malocclusion into a Class I malocclusion.
The role of growth and morphogenetic patterns remains the primary determinant of mandibular development.
Challenges and Limitations
Need for Controlled Studies:
Many claims regarding mandibular growth stimulation and repositioning remain anecdotal or based on uncontrolled studies. Rigorous biometric analyses are necessary to substantiate such claims.
Physiological Variability:
Individual growth patterns, genetic predispositions, and environmental factors contribute to the variability in response to orthodontic treatment.
Role of Functional Appliances:
While functional appliances may influence mandibular posture temporarily, their long-term impact on growth remains uncertain.
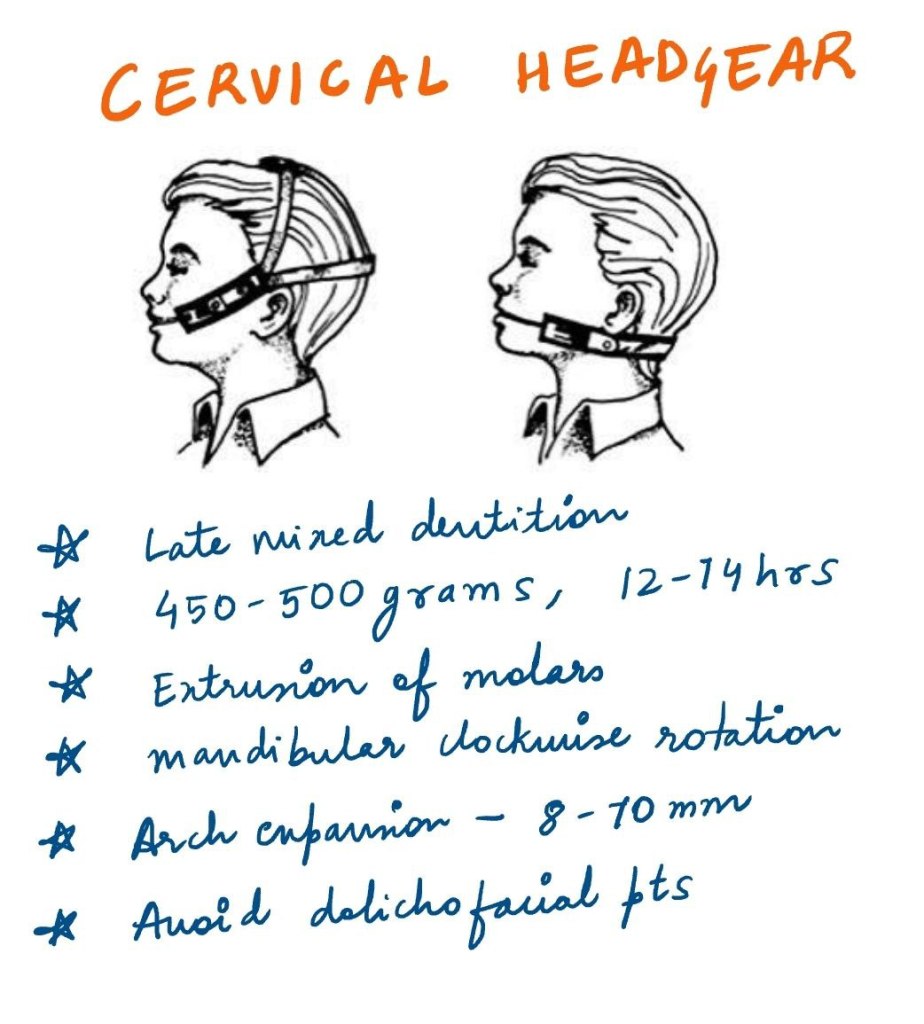
Treating Class II malocclusion can be a challenging endeavor due to the diverse range of appliances available and the complexity of dental and skeletal relationships between the maxilla and mandible. To simplify the analysis and ensure consistent outcomes, studies focusing exclusively on cervical headgear have provided valuable insights.
Why Cervical Headgear?
Cervical headgear is like the Swiss Army knife of Class II malocclusion treatment. Its efficacy, however, depends significantly on when you start using it. Research suggests that the late mixed dentition or the onset of permanent dentition is the orthodontic equivalent of “prime time.” With a force of 450 to 500 grams on each side—basically the weight of a small apple—the appliance works best when worn for 12 to 14 hours daily. Yes, that’s half a day, so patients need to be as committed as a coffee addict to their morning brew.
Effects of Cervical Headgear on Molar Position and Bite
One notable effect observed in studies is the extrusion of maxillary first molars, a phenomenon first described in the 1970s. Think of it as the molars getting a little too excited and rising up—like bread dough, but less tasty. This leads to bite opening and an increase in vertical parameters, which can be a problem for dolichofacial patients with long faces. Adding height to an already tall face is like putting a top hat on a giraffe—probably not the best idea. However, with careful management, even vertical growers can benefit from this appliance.
Mandibular Rotation and Vertical Changes
Molar extrusion also causes mandibular clockwise rotation, leading to an increase in the mandibular plane angle. This backward rotation is well-documented, and while it’s not ideal, it’s not the end of the world either. After all, even the best orthodontic plans can sometimes feel like trying to herd cats—challenging but ultimately rewarding.
Arch Expansion and Alignment
Cervical headgear also moonlights as a gentle expander of the upper arch, introducing an 8 to 10 mm expansion in the inner bow. This expansion helps align maxillary teeth and the mandibular arch to follow suit. It’s like getting a BOGO deal on alignment—who doesn’t love that? These changes create excellent conditions for the mandible to grow to its full potential, making Class II correction a reality.
Maxillary Repositioning and Overjet Correction
Another party trick of cervical headgear is improving the maxillomandibular relationship. By restricting forward and downward maxillary displacement, it lets the mandible grow normally, compensating for the initial overjet. It’s like giving the mandible a chance to shine on the orthodontic stage—finally, the underdog gets its moment.
Key Takeaways for Orthodontic Students
Timing Matters: Initiate treatment during late mixed dentition or early permanent dentition for optimal results.
Patient Selection: Avoid using cervical headgear in dolichofacial patients with extreme vertical growth patterns.
Appliance Effects: Understand the implications of molar extrusion, mandibular rotation, and vertical parameter changes.
Comprehensive Benefits: Leverage the appliance’s ability to expand arches, improve alignment, and enhance the maxillomandibular relationship.
Cervical headgear remains a cornerstone in the treatment of Class II malocclusion. By mastering its application and understanding its effects, orthodontic students can achieve predictable and effective outcomes in their clinical practice.
Understanding the growth patterns of the maxillary and mandibular lips is essential for effective orthodontic treatment planning. As orthodontic students, recognizing the interplay between facial soft tissues and the underlying hard tissues, particularly during the critical growth period from 8 to 18 years, can significantly influence treatment outcomes. This blog post delves into a lip growth and its implications for orthodontic therapy, providing data-driven insights and clinical guidelines.
Key Findings on Lip Growth
1. Maxillary Lip Length
Maxillary Lip Length Growth (mm)
Age 8
Age 18
Percentage Increase
Largest growth occurred between
Males
17.73
21.53
21.43%
Ages 10 and 16.
Females
17.73
19.88
12.11%
Ages 10 and 14.
2. Maxillary Lip Thickness
Maxillary Lip Thickness Growth (mm)
Age 8
Age 18
Percentage Increase
Males
10.77
15.76
46.33%
Growth was continuous, with the largest increase between ages 12 and 16.
Females
10.90
12.50
14.68%
Growth occurred primarily between ages 10 and 14.
3. Mandibular Lip Length
Mandibular Lip Length Growth (mm)
Age 8
Age 18
Percentage Increase
Males
19.14
26.53
38.56%
Largest increase occurred between ages 12 and 16.
Females
19.14
22.73
18.65%
Growth occurred primarily between ages 10 and 16.
4. Mandibular Lip Thickness
Males: Increased steadily from ages 8 to 16, with a plateau between ages 16 and 18.
Largest increases occurred between ages 14 and 16.
Females: Growth was less pronounced, with significant increases only between ages 10 and 14.
Clinical Implications for Orthodontic Treatment
1. Sexual Dimorphism in Lip Growth
Males experience greater increases in both lip length and thickness compared to females.
Females show more limited growth, particularly in lip thickness during puberty.
2. Extraction Therapy Considerations
Female Patients: Limited lip thickening during puberty makes the effects of extraction therapy more noticeable, especially in patients with straight or concave profiles. Treatment plans should be approached with caution to avoid adverse effects on facial esthetics.
Male Patients: Greater lip thickening provides more flexibility for extractions without significantly impacting facial profile fullness.
Maxillary Lip Thickness Growth Rates
Males:
0.5 mm/year (ages 8–12).
0.7 mm/year (ages 12–16).
Females:
0.5 mm/year (ages 10–12).
0.3 mm/year (ages 12–14).
Conclusion
Understanding the growth patterns of maxillary and mandibular lips is essential for predicting soft-tissue responses and planning effective orthodontic treatments. Sexual dimorphism plays a significant role, with males experiencing greater growth in both lip length and thickness compared to females. These differences must be factored into treatment decisions, particularly for extraction therapy, to ensure optimal esthetic and functional outcomes. As orthodontic students, incorporating these insights into clinical practice will enhance your ability to deliver patient-centered care.
Orthodontic care primarily focuses on dental esthetics and masticatory function, but its impact on sound production is often overlooked. Sound production involves a dynamic interaction with the oral cavity, requiring orthodontists to recognize how dental anomalies and treatments influence speech. Enhanced patient care can be achieved through better treatment planning and referrals to speech pathologists for patients whose malocclusions affect speech production. This is particularly relevant for adults requiring proper speech for professional purposes.
Definition of Sound and Speech Mechanism
Sound is mechanical vibration energy requiring the coordination of neural, muscular, mechanical, aerodynamic, acoustic, and visual elements. Speech production involves four processes:
Language processing in the brain.
Motor command generation to vocal organs.
Articulatory movements of the oral cavity.
Air emission from the lungs.
Speech sounds are classified into:
Vowels: Produced without obstruction to airflow.
Consonants: Produced with varying obstructions in oral or nasal cavities.
Classification
Ingram’s Classification:
Dysphonia: Disorders of vocalization.
Dysrhythmia: Respiratory coordination issues.
Dysarthria:
Due to neurological abnormalities (e.g., motor neuron lesions).
Due to local abnormalities (e.g., jaws, teeth, palate).
Non-Structural Disorders: Mental, hearing, or environmental factors.
Developmental Disorders: Abnormal or delayed speech development.
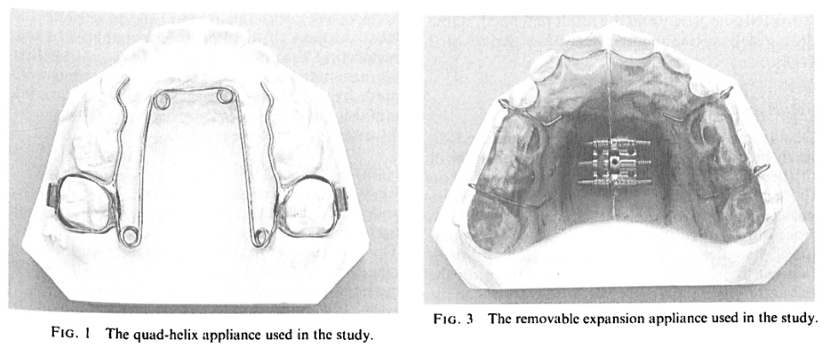
Palatal expansion has been a cornerstone of orthodontic treatment for over a century. Despite its proven efficacy, this technique has sparked debates within the orthodontic community. Is rapid expansion the best approach, or do slower methods offer greater stability? Let’s dive into the history, mechanics, and clinical applications of maxillary expansion, with a special focus on the quad-helix appliance.
The primary goal of palatal expansion is to coordinate the maxillary and mandibular denture bases, addressing narrow or collapsed arches. This can be achieved through:
Orthodontic Movement (tooth-focused)
Orthopedic Movement (bone-focused)
Combination Therapy
A variety of appliances—fixed, semi-fixed, and removable—are employed to achieve these goals.
Method
Advantages
Challenges
Rapid Palatal Expansion
Quick skeletal changes
Potential for relapse and sutural strain
Slow Expansion
Greater histologic integrity of sutures
Requires longer treatment time
HISTORY
Coffin Loop Appliance:
Incorporated in a vulcanite plate for upper arch expansion.
Produces continuous force due to the configuration of the palatal compound loop.
Martin Schwarz Appliance:
Popular in Europe.
Utilizes tissue-borne anchorage with wire components for tooth movement.
Expansion force is intermittent due to the jackscrew mechanism.
Haas and Wertz Fixed Appliance:
Designed for rapid expansion of the midpalatal suture in narrow maxillary arches.
Cemented to maxillary first premolars and first permanent molars.
Includes a palatal jackscrew and acrylic extensions.
Produces lateral orthopedic movement of the maxilla due to high force magnitude.
Load-Activation Characteristics:
Chaconas and Caputo found differences in stress transmission through craniofacial bones with various fixed expansion appliances.
Impact on craniofacial sutures varies depending on the appliance.
Rickett’s “W” Expansion Appliance:
Initially used for cleft palate conditions with collapsed dental arches.
Acts continuously over time until activation force dissipates.
What Makes the Quad-Helix Appliance Unique?
Helical Loops for Increased Flexibility:
Initially added to the posterior segment of the palatal arch
Further modification introduced four loops (two anterior and two posterior), creating the quad-helix appliance.
Construction Details:
Made of 0.038-inch (0.975 mm) wire.
Soldered to bands cemented to maxillary first permanent molars or deciduous second molars, depending on the patient’s age.
Initial Activation and Effects:
Appliance is activated before cementation.
Results in expansion of buccal segments and rotation of banded teeth
Force Magnitude:
Chaconas and Caputo reported that 8 mm of expansion before cementation generates approximately 14 ounces of force
Effectiveness in Different Age Groups:
Effective in orthopedically widening the maxilla in children, helping to establish a normal maxillomandibular relationship.
Force is sufficient for tooth movement but insufficient for orthopedic effects in adults with closed midpalatal sutures.
In children, particularly in the deciduous or early mixed dentition stages, the resistance of the patent suture is lower than the dentoalveolar area.
Clinical Case: A Pediatric Success Story
Patient History: Prolonged thumb-sucking led to a narrow maxilla due to lowered tongue position and buccinator muscle forces.
Treatment: Quad-helix appliance activated ~8 mm, sufficient for maxillary expansion.
Outcome: Successful expansion and resolution of thumb-sucking habit. The appliance’s palatal position ensured comfort and minimal impact on speech.
Maxillary Molar Width: Increased by an average of 5.88 mm, reflecting significant dental expansion.
Average Frontal Molar Relation: Improved by 2.95 mm, indicating better occlusal alignment.
Maxillary Intercanine Width: Expanded by 2.74 mm, enhancing anterior dental arch form.
Orthopedic Changes (T₁ to Tₚ)
Maxillary Width: Increased by 0.92 mm, with five cases showing expansions exceeding 2.7 mm.
Maxillomandibular Width: Increased by 0.89 mm, with notable cases surpassing 1.4 mm.
Palatal Changes: The anterior palate moved downward, increasing maxillary height.
Relapse and Stability (Tₚ to T₂)
Minimal Relapse: Dental expansions remained stable over 42 months.
Orthopedic Effects: Demonstrated high stability, contrasting with the relapse often seen in rapid palatal expansion.
Palatal Plane and Maxillary Height: Slight decreases observed, indicating no net parallel downward movement.
Slow vs. Rapid Expansion
Slow expansion using the quad-helix appliance demonstrated superior stability and less relapse compared to rapid palatal expansion. The gradual physiologic movement allowed the facial skeleton to adapt, ensuring long-term stability.
Bite Opening
Active Expansion (T₁ to Tₚ): Slight bite opening occurred due to occlusal interferences.
Post-Expansion (Tₚ to T₂): Additional bite opening was attributed to orthodontic treatment rather than the expansion appliance.
Facial Skeletal Considerations
Stability was influenced by initial nasal and maxillary widths:
Narrow Maxilla + Normal/Wide Nasal Width: High stability.
Narrow Nasal Width + Normal Maxilla: Lower stability.
Facial Type
The sample skewed toward brachyfacial types, limiting conclusions about expansion outcomes across facial types.
Promote beneficial dentoskeletal changes during growth periods (Bell, 1982).
Posterior cross-bites develop early and are not self-correcting (Moyers & Jay, 1959; Thilander et al., 1984).
Orthodontic Response to Expansion
Initial response completed within a week (Storey, 1973; Cotton, 1978; Hicks, 1978).
Subsequent movements occur as compressed buccal alveolar plate resorbs at the root-periodontal interface due to continued force (Storey, 1973).
Orthopaedic Effects of Expansion
Sufficient transverse forces can overcome bioelastic strength of sutural elements, causing:
Orthopaedic separation of maxillary segments (Storey, 1973; Chaconas & de Alba y Levy, 1977; Cotton, 1978; Hicks, 1978).
Palatal segment repositioning continues until force is reduced below sutural tensile strength.
Stabilization involves reorganization and remodeling of sutural connective and osseous tissues (Storey, 1973; Ekstrom et al., 1977).
Increased Maxillary Arch Width
Linked to orthodontic and/or orthopaedic effects of expansion (Ficarelli, 1978; Moyers, 1984).
Initial changes involve lateral tipping of posterior maxillary teeth due to compression and stretching of periodontal and palatal soft tissues.
Midpalatal Sutural Opening and Maxillary Displacement
Expansion leads to:
Downward and forward displacement of the maxilla with bite opening (Haas, 1961).
Downward and backward rotation of the mandible, increasing the vertical dimension of the lower face (Haas, 1970).
Subsequent recovery of mandibular posture noted in most cases (Wertz, 1970).
Rate of Expansion and Dental Arch Width Increase
Rapid Maxillary Expansion (Krebs, 1959, 1964):
Subjects aged 8–19 years showed an average dental arch increase of 6.0 mm (range: 0.5–10.3 mm).
Skeletal changes accounted for:
~50% of the arch width increase in 8–12-year-olds.
~33% of the increase in 13–19-year-olds.
Slow Maxillary Expansion (Hicks, 1978):
Subjects aged 10–15 years showed a dental arch width increase of 3.8–8.7 mm.
Skeletal response ranged from 16–30%, with lower skeletal response in older patients.
Buccal tipping of molars and skeletal segments contributed to arch width increase.
Asymmetrical angular changes between left and right molars and maxillary segments were observed.
Removable Plates and Sutural Growth (Skieller, 1964):
In subjects aged 6–14 years:
20% of dental arch widening was attributed to sutural growth.
Sutural growth rate during expansion was significantly greater than during follow-up, indicating stimulated growth during expansion.
Removable Plates and Sutural Growth (Skieller, 1964):
Study on 20 subjects aged 6–14 years:
20% of dental arch widening was attributed to sutural growth.
Growth rate at the mid-palatal suture was significantly higher during expansion compared to the follow-up period.
Suggests that sutural growth is stimulated during the expansion period.
Histologic Findings in Slow Expansion Procedures:
Sutural separation occurs at a controlled rate, maintaining tissue integrity during maxillary repositioning and remodeling (Storey, 1973; Ekstrom et al., 1977; Cotton, 1978).
Relapse Tendency During Post-Retention Period:
Relapse potential is reduced in slow expansion procedures due to: