Headgear—an iconic yet often dreaded orthodontic appliance—has been around for decades, serving as a non-surgical method to control maxillary growth and molar positioning. Despite its reputation among patients, orthodontists continue to rely on it for effective anchorage and skeletal modifications
🔹 Cervical Pull Headgear – The “Easygoing” One 😌
- Simple to make, patients tolerate it better.
- But… it can be a drama queen! 😵
- Moves molars backward but also tips them, roots going mesially (oops!).
- Can extrude molars, making the face longer—hello, gummy smile? 🙃
- Stability? Meh. Too much tipping, not enough translation.
🔹 High-Pull Headgear – The “Disciplined” One 🎯
- Distal movement? ✅
- Intrusion instead of extrusion? ✅
- More control over force direction? ✅
- Basically, it’s like telling molars, “We’re going back AND staying put.” 🚀
Science Says… But How Much Force? 🤔
Studies show high-pull headgear can move molars distally and tweak vertical growth, possibly even making skeletal changes. 🦴 But here’s the catch—how much force is just right? Some say a lot, some say less is more. Even animal studies couldn’t agree. 🐭🐶🐷
So, the mission (if you choose to accept it) is to figure out the ideal force system—gentle but effective—because we’re in the business of moving teeth, not wrecking them. 🦷💀
Let’s dissect the MATERIALS & METHODS section of this study—because numbers, wires, and ceph tracings are what we live for! 🧐💀
🧑⚕️ Patient Selection: Who Got to Wear This Fashion Statement?
✅ 24 adolescent patients (all Caucasian, because diversity in ortho studies is still a work in progress 🤦♂️)
✅ Molar occlusion: Between 3.0 to 7.0 mm Class II at the start of treatment
✅ Skeletal age: 9.5 to 12.5 years (determined from hand-wrist films 📸)
✅ Interlabial gap ≥ 2.0 mm + Increased lower facial height (classic hyperdivergent cases!)
✅ Treatment duration: 6 months
✅ Groups:
🔹 12 patients = High-Pull Headgear Group 🦷🔧
🔹 12 patients = Control Group (No headgear, lucky them? 🤔)
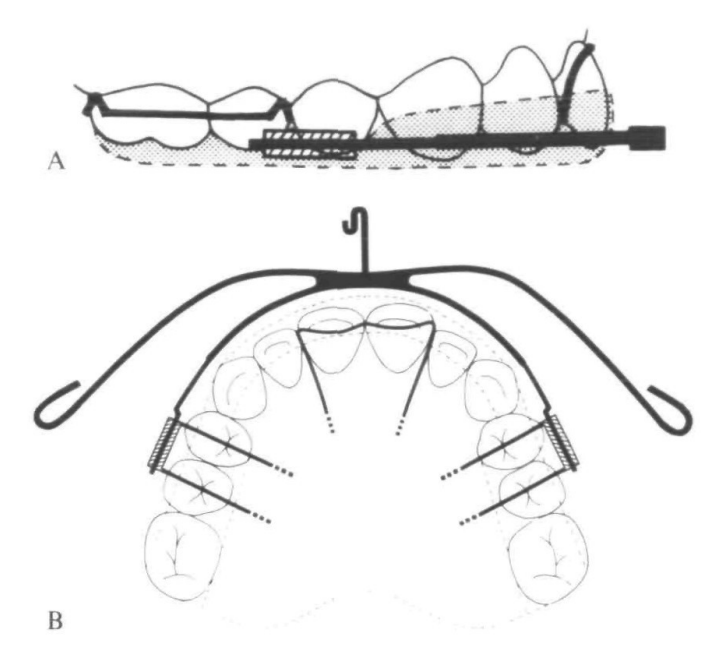
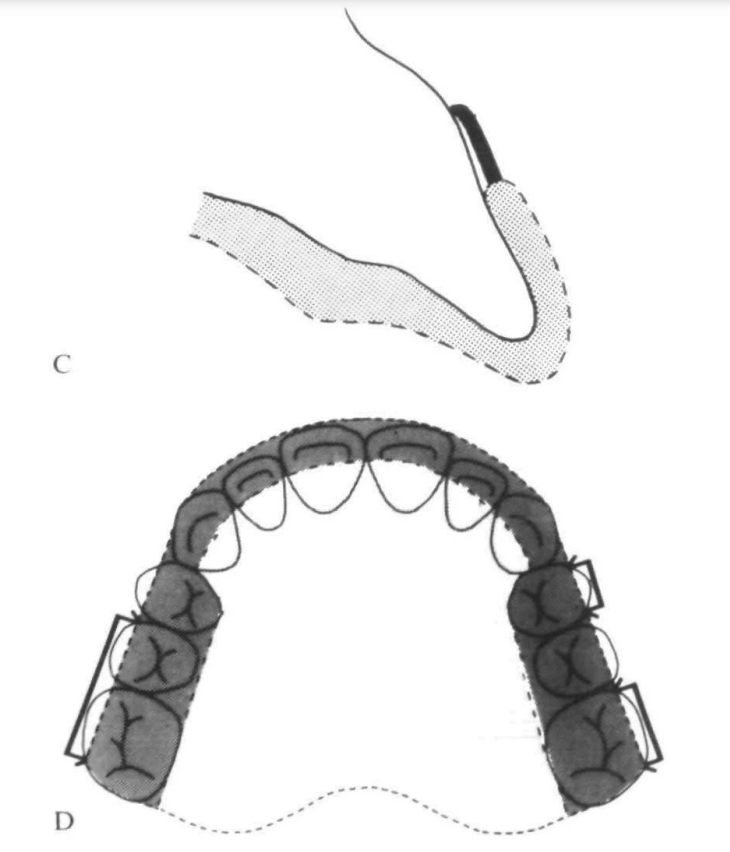
⚙️ Appliance Design: The Ortho Engineering Behind It
🎯 Interlandi Type High-Pull Headgear (fancy name, simple purpose)
🔹 Force Application:
- Connected to the head straps using ¼-inch latex elastics
- Elastic attachment points were adjustable to control force direction 🎛️
- Force directed through the buccal trifurcation of maxillary first molars (approx. center of resistance 📍)
🔹 Key Specs:
- Inner bow: Parallel to occlusal plane
- Outer bow: Shortened so it didn’t extend past the maxillary first molars
- Force applied: 500g per side (measured with a force gauge ⚖️)
- Effects aimed for: Distalization + Intrusion (not just tipping like cervical pull!)
💡 Bonus Feature: 0.032 x 0.032 Stainless Steel Transpalatal Arch
- Purpose? 🧐
✅ Maintained arch symmetry
✅ Prevented molar rotation (because we don’t want them spinning like a Beyblade! 🌀)
🧐 Elastic Force Decay?
- Measured over 15 hours – result? Minimal loss, so clinically insignificant (phew! 😅)
- Reminder: Patients had to change elastics daily (because worn-out elastics = wasted treatment time ⏳)
📝 Patient Cooperation: Did They Even Wear the Headgear?
Let’s be honest—compliance is our biggest enemy in headgear treatment. 😤 Here’s how they kept track:
1️⃣ Daily diary 📖 – Parents checked if their kids were actually wearing it.
2️⃣ Molar mobility check 🦷 – If the teeth were moving, the headgear was doing its job!
3️⃣ Ease of insertion 🔄 – If the bow slipped in too easily, it probably wasn’t worn enough.
4️⃣ Physical wear signs 🧐 – Scratches, bent wires = proof of usage!
5️⃣ Ceph changes 📊 – Measured interdental spacing, overjet reduction, and buccal occlusion improvement.
🎬 Molar Action: The Great Escape! 🦷💨
| Molar Movement 🦷 | Treatment Group (Headgear Warriors) | Control Group (Lazy Lords 😴) |
|---|---|---|
| Distal movement | 2.56 mm 🔙 (SIGNIFICANT) | 0.23 mm 🔜 (Minimal) |
| Vertical movement (Intrusion/Eruption) | 0.54 mm Intrusion ⬇️ | 0.23 mm Eruption ⬆️ |
| Overall Motion | DISTAL + INTRUSION 📉 | MESIAL + ERUPTION 📈 |
📢 Translation: The molars in the treatment group took a step back (distalized) and went slightly underground (intruded). Meanwhile, the control group molars were partying and moving forward & upwards! 🥳
🏛️ Maxilla: Growth on a Diet! 🍽️
The maxilla in the treatment group experienced a growth restriction thanks to the headgear’s orthopedic effect! 🚫🏗️
| Maxillary Growth (Anteroposterior & Vertical) | Treatment Group (Headgear Effect) | Control Group (Free Growth) |
| A-point movement (Horizontal) | 0.33 mm backward ⏪ | 0.5 mm forward ⏩ |
| ANS & PNS movement (Vertical Growth) | ↓ by ~0.5 mm 📉 | Normal downward growth 📈 |
📢 Translation:
- Headgear applied the brakes on maxillary forward growth.
- Maxillary vertical growth was reduced by half.
🔬 Skeletal & Soft Tissue: The “No Drama” Zone!
Unlike the molars, some skeletal parameters remained unchanged. 📏
| Measurement | Change in Treatment Group? |
| Nasal floor | No difference 😴 |
| Mandibular plane | No difference 😴 |
| Skeletal convexity | No difference 😴 |
| Soft tissue convexity | No difference 😴 |
📢 Translation: The headgear worked on the maxilla and molars but didn’t mess with soft tissues or overall facial profile. No major aesthetic changes. (Ortho-approved!) 😌
⌛ 24-Hour Headgear vs. Intermittent Wear: The Big Debate! 🤔
Some orthodontic gurus like Armstrong & Badel believe that wearing headgear 24/7 is the ultimate “Satyam Shivam Sundaram” of orthodontics! 🎭 But guess what? This study proves that intermittent wear (12 hours/day) still packs a punch! 🥊
✅ Correction of Class II molar relation? ✅
✅ Distal molar movement? ✅
✅ Maxillary growth restriction? ✅
🎉 And all that in just 6 months!
💡 Takeaway: Patients don’t have to be headgear hermits 24/7—a balanced, realistic 12-hour wear can still yield significant results!
💪 The Power of Force: 500 gm & The Maxillary Game Changer! ⚡
🔬 The Recipe for Maxillary Control:
- Armstrong, Watson, Badel, & Graber recommended going all out with 400–1000 gm of force if rapid orthopedics was the goal! 🚀
- This study? A sweet spot of 500 gm did the trick! Less drama, great results! 🎯
💡 Key Finding:
- A-point movement was restricted—a major win! The maxilla stayed in check instead of running wild like a Bollywood hero in a chase scene! 🏃💨
- Forward growth of ANS was significantly reduced, meaning the headgear truly controlled skeletal development! 🏗️
💡 Comparison with Other Studies
| Researcher 👨🏫 | Molar Distalization (mm) 📉 | Treatment Duration ⏳ | Force Level 🎯 |
|---|---|---|---|
| This Study 🎯 | 2.56 mm | 6 months | Lighter Forces 💨 |
| Badel (118) | 2.3 mm | 4 months | Full-time wear |
| Weislander (S) | ~3.0 mm | 2–3 years | Similar Force |
| Watson (12) | 3.0 mm | 5–16 months | Higher Force 🔥 |
📢 Translation for Real Life:
- Short-term wear (6 months) achieved similar results as years of treatment in older studies!
- Less force, same or better results! 🤯
- Weislander (300–400 gm) = A-point & ANS moved 2 mm distally over 3 years!
- Watson (600–1000 gm) = A-point & ANS shifted 4 mm distally in under a year!
- Baumrind = Mandibular growth slowed down in treatment groups compared to controls.
📢 This study adds to the evidence that:
✔️ Even with moderate force, skeletal changes occur.
✔️ Maxillary growth restriction is real—it’s not just an ortho myth!
✔️ Mandibular growth showed a mild reduction, but not enough to worry
🎯 Angle of Attack: 20° & The Power of Sin(θ)!
Ever wondered how headgear force actually works? It’s not just “wear it and hope for the best!” 😆 There’s physics involved!
💡 Key Point:
- In our study, the force of the appliance was directed at ~20° to the occlusal plane.
- This means the intrusive force on maxillary molars = 500 gm × sin(20°).
📢 Translation for the non-math lovers:
🔹 Headgear isn’t just pulling back molars—it’s also subtly pushing them upwards (intrusion).
🔹 This changes the maxilla’s growth dynamics, and we’ve got numbers to prove it! 📊
🔬 ANS & PNS: No More “Bollywood Slow-Motion Growth” 🎭
📚 What Happens Normally?
- The ANS (Anterior Nasal Spine) moves down during natural growth.
- The PNS (Posterior Nasal Spine) follows suit, leading to an increase in the palatal plane angle.
📚 What Happened in Our Study?
✅ Headgear stopped ANS & PNS downward movement 📉
✅ No significant changes in nasal floor angulation
✅ Palatal plane angle remained stable
💡 Takeaway:
- Headgear isn’t just about molars moving back—it’s controlling vertical growth too!
- Watson (1.04°/year) & Baumrind (1.1°/year) reported slight changes in palatal plane angle, but our headgear kept it locked in place! 🎯
🦷 Maxillary Molar Intrusion: The Power of High-Pull Headgear!
| Group 🎭 | Maxillary Molar Movement 📉 |
|---|---|
| Headgear Group 🏹 | 0.54 mm Intrusion ⬇️ |
| Control Group 😴 | 0.42 mm Eruption ⬆️ |
📢 Translation:
- Headgear warriors saw molars being pushed slightly up (~0.54 mm).
- Control group molars went rogue and erupted (~0.42 mm).
- Why does this matter? Because it helps control vertical facial growth!
💡 But did it shorten the face?
Nope! Lower facial height didn’t decrease significantly. Meaning, no unwanted “face shrinkage” occurred. 🚀
🤔 What About Lower Molars & Occlusion?
📚 Common Concern: If maxillary molars are intruded, will lower molars erupt to compensate and mess up occlusion?
✅ Good news! No significant compensatory eruption of the lower molars was found! 🎉
✅ The functional occlusal plane remained stable throughout the 6-month period.
💡 Takeaway:
- Headgear didn’t throw the bite into chaos. Everything stayed balanced! ⚖️
🔮 Future Predictions: “What If We Went Longer?” 🕰️
- What if we kept headgear for another year?
📢 Watson (600–1000 gm force) showed 4.0 mm of molar intrusion over a longer period! - What does that mean for our study?
✔️ More skeletal changes would likely become statistically significant.
💡 Ortho Wisdom:
- Short-term wear (6 months) already made a difference!
- Longer wear = more pronounced skeletal effects!
📚 Common Ortho Fear: “What if only the crown moves, leaving the roots behind?” 😱
✅ Good news! Our study found translation—meaning:
🔹 Both crowns AND roots moved distally! ✅
🔹 Roots actually moved 2.5° further than crowns! 🤯
💡 Why?
- Normal mesial tipping of maxillary molars is always present.
- The force was applied at the trifurcation area (right below the furcation).
- This led to a small moment that helped move the roots backward too! 🔄
💡 Ortho Pro Tip:
The center of resistance of molars is below the trifurcation area. Since we applied force slightly above it, we got a controlled distal shift! 🚀
🤔 What Helped Maintain Symmetry?
✅ The Palatal Arch! 🦷
- Helped move right & left molars symmetrically 📏🔄
- Prevented rotations or uneven shifts 🚫🔄
- Allowed for stable occlusal changes! 🏆
Final Thoughts: Should You Still Consider Headgear?
Despite the rise of TADs (temporary anchorage devices) and other modern alternatives, cervical pull headgear remains a reliable, non-invasive option for controlling molar positioning and maxillary growth. While compliance remains a challenge, the study highlights its effectiveness in correcting skeletal Class II discrepancies without compromising vertical dimension.
🔹 Takeaway: Headgear is not just a relic of the past—it’s a scientifically backed tool that continues to hold value in contemporary orthodontics.
Would you still prescribe it, or do you prefer newer anchorage methods? Drop your thoughts below!