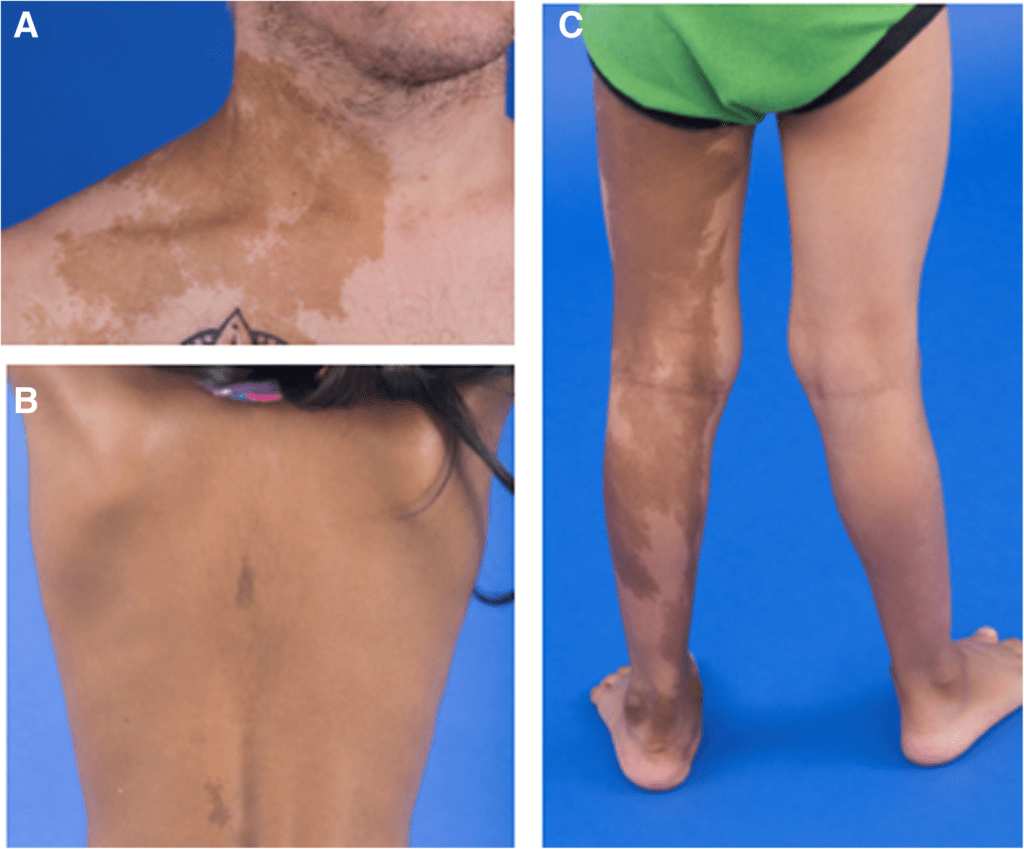
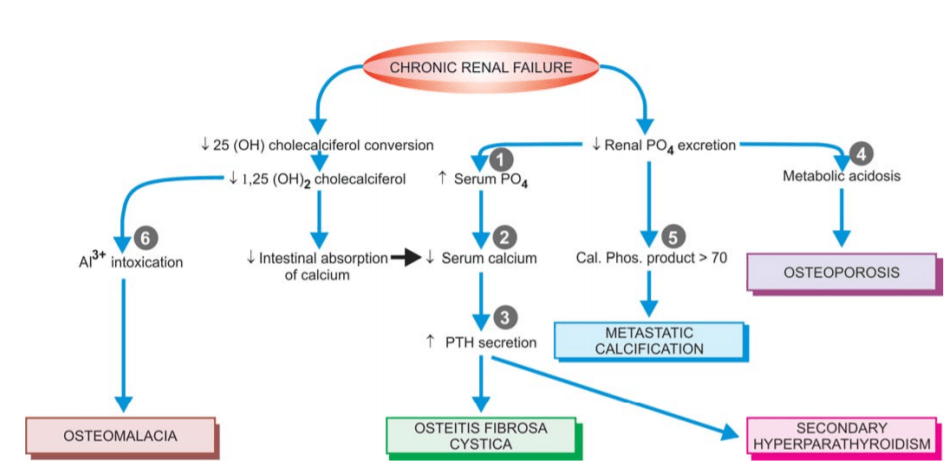
The following skeletal lesions can be identified in renal osteodystrophy:
Mixed osteomalacia-osteitis fibrosa is the most common manifestation of renal osteodystrophy resulting from disordered vitamin D metabolism and secondary hyperparathyroidism.
Pure osteitis fibrosa results from metabolic complications of secondary hyperparathyroidism.
Pure osteomalacia of renal osteodystrophy is attributed to aluminium toxicity.
Renal rickets resembling the changes seen in children with nutritional rickets with widened osteoid seams may occur .
Osteosclerosis is characterised by enhanced bone density in the upper and lower margins of vertebrae.
Metastatic calcification is seen at extraosseous sites such as in medium-sized blood vessels, periarticular tissues, myocardium, eyes, lungs and gastric mucosa.
source -textbook of pathology for dental students c p baveja and image source- Google
Oral cancer is a disease with very poor prognosis because it is not recognised and treated when small and early.
INCIDENCE.
-Squamous cell (epidermoid) carcinoma comprises 90% of all oral malignant tumours and 5% of all human malignancies.
-The peak incidence in the UK and the USA is from 55 to 75 years of age, whereas in India it is from 40 to 45 years of age.
-Oral cancer is a very frequent malignancy in India, Sri Lanka and some Eastern countries, probably related to habits of betel-nut chewing and reversed smoking .
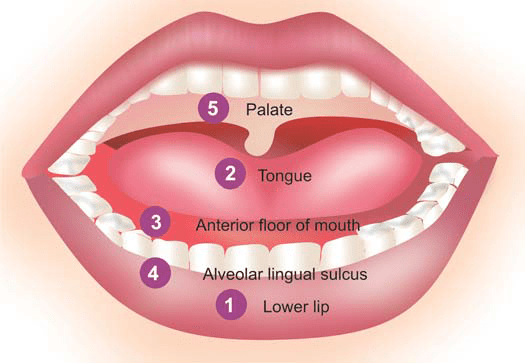
– There is a definite male preponderance. -It can occur anywhere in the mouth but certain sites are more commonly involved.
-These sites, in descending order of frequency, are: the lips (more commonly lower), tongue, anterior floor of mouth, buccal mucosa in the region of alveolar lingual sulcus, and palate.
sites of scc in decending order
ETIOLOGY.
As with other forms of cancer, the etiology of squamous cell carcinoma is unknown. But a number of etiological factors have been implicated: Strong association: i) Tobacco smoking and tobacco chewing causing leukoplakia is the most important factor .
ii) Chronic alcohol consumption. iii) Human papilloma virus infection, particularly HPV 16, 18 and 33 types.
Weak association: i) Chronic irritation from ill-fitting denture or jagged teeth. ii) Submucosal fibrosis as seen in Indians consuming excess of chillies. iii) Poor orodental hygiene. iv) Nutritional deficiencies. v) Exposure to sunlight (in relation to lip cancer). vi) Exposure to radiation. vii) Plummer-Vinson syndrome, characterised by atrophy of the upper alimentary tract.
The most common molecular alterations in oncogenes seen in squamous cell carcinoma of the oral cavity are in p16, p53, cyclin D, p63, PTEN, and EGFR.
MORPHOLOGIC FEATURES.
Grossly, squamous cell carcinoma of oral cavity may have the following types
i) Ulcerative type—is the most frequent type and is characterised by indurated ulcer and firm everted or rolled edges. ii) Papillary or verrucous type—is soft and wart-like growth. iii) Nodular type—appears as a firm, slow growing submucosal nodule. iv) Scirrhous type—is characterised by infiltration into deeper structures.
*All these types may appear on a background of leukoplakia or erythroplasia of the oral mucosa. Enlarged cervical lymph nodes may sometimes bepresent.
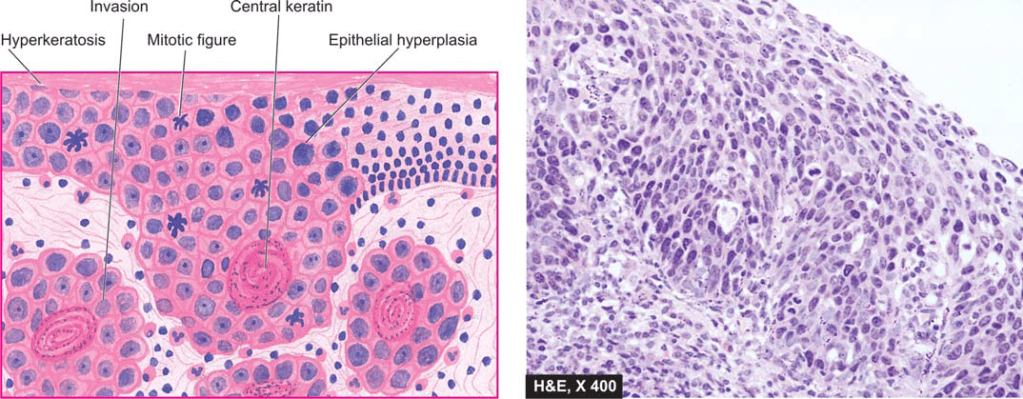
Histologically.
– squamous cell carcinoma ranges from well-differentiated keratinising carcinoma to highly undifferentiated neoplasm . -Changes of epithelial dysplasia are often present in the surrounding areas of the lesion.
–Carcinoma of the lip and intraoral squamous carcinoma are usually always well-differentiated
source -textbook of pathology for dental students harsh mohan
DEFINITION- Leukoplakia (white plaque) may be clinically defined as a white patch or plaque on the oral mucosa, exceeding 5 mm in diameter, which cannot be rubbed off nor can be classified into any other diagnosable disease.
–the term ‘leukoplakia’ is reserved for epithelial thickening which may range from completely benign to atypical and to premalignant cellular changes.
INCIDENCE–
1. It occurs more frequently in males than females.
2.The lesions may be of variable size and appearance.
3. The sites of predilection, in descending orderof frequency, are: cheek mucosa, angles of mouth, alveolar mucosa, tongue, lip, hard and soft palate, and floor of the mouth.
4.In about 4-6% cases of leukoplakia, carcinomatous change is reported.
ETIOLOGY-
1. It has the strongest association with the use of tobacco in various forms, e.g. in heavy smokers (especially in pipeand cigar smokers) and improves when smoking is discontinued, and in those who chew tobacco as in paan, paan masaala, zarda, gutka etc.
2.The condition is also known by other names such as smokers keratosis and stomatitis nicotina.
3. Other etiological factors implicated are chronic friction such as with ill-fitting dentures or jagged teeth, and local irritants like excessive consumption of alcohol and very hot and spicy foods and beverages.
4. A special variety of leukoplakia called ‘hairy leukoplakia’ has been described in patients of AIDS and has hairy or corrugated surface but is not related to development of oral cancer.
leukoplakia seen on the buccal mucosa
MORPHOLOGIC FEATURES.
1.Grossly, the lesions of leukoplakia may appear white, whitish-yellow, or redvelvety of more than 5 mm diameter and variable in appearance.
2.They are usually circumscribed, slightly elevated, smooth or wrinkled, speckled or nodular.
Histologically, leukoplakia is of 2 types:
The hyperkeratotic type- This is characterised by an orderly and regular hyperplasia of squamous epithelium with hyperkeratosis on the surface.
Dysplastic type- When the changes such as irregular stratification of the epithelium, focal areas of increased and abnormal mitotic figures, hyperchromatism, pleomorphism, loss of polarity and individual cell keratinisation are present, the lesion is considered as epithelial dysplasia
-The subepithelial tissues usually show an inflammatory infiltrate composed of lymphocytes and plasma cells.
– The extent and degree of the epithelial changes indicate the degree of severity of the epithelial dysplasia.
-Usually, mild dysplasia may revert back to normal if the offending etiologic factor is removed, whereas severe dysplasia indicates that the case may progress to carcinoma.
source – textbook of pathology for dental students harsh mohan
Transplants from one individual to another member of the same species (‘allografts’) are recognised as foreign and rejected.
Gorer (1930) identified the antigens responsible for allograft rejection in inbred mice that led to the discovery of the major histocompatibility complex (MHC).
The MHC in humans is known as the human leukocyte antigen (HLA) complex.
HLA complex
Histocompatibility antigens mean cell surface antigens that evoke immune response to an incompatible host resulting in allograft rejection.
These alloantigens are present on surface of leucocytes in man and are called human leucocyte antigens (HLA) and the set of genes coding for them is named the HLA Complex.
The HLA complex of genes is located on short arm of chromosome 6 and is grouped in three classes
Class I
HLA-A, HLA-B and HLA-C
Class II
HLA-DR, HLA-DQ and HLA-DP (All of these are present within HLA-D region of HLA complex.)
Class III ( Complement loci encode for C2, C4 and Factor B of complement system and tumour necrosis factors (TNF) alpha and beta)
A locus is the position where a particular gene is located on the chromosome.
HLA loci are multiallelic i.e. the gene present on the locus can be any one of several alternative forms (alleles).
Each allele determines a distinct antigen. There are 24 alleles at HLA-A locus and 50 at HLA-B. HLA system is very pleomorphic. Every individual inherits one set of HLA-genes from each parent.
1.Class 1 MHC Antigens (A, B, C)
The MHC class I antigens are present on the surface of all nucleated cells. They are involved in graft rejection and cell mediated cytolysis. The cytotoxic T cells (CD8) recognise MHC class I antigens for their action.
2 Class II MHC Antigens (DR, DQ and DP)
They have a very limited distribution and are principally found on the surface of macrophages, monocytes, activated T-lymphocytes (CD4) and B-lymphocytes. They are primarily responsible for the graft-versus-host response and the mixed leukocyte reaction (MLR).
3.Class III MHC Antigens
Class III genes encode C2, C4 complement components of the classical pathway and properdin factor B of the alternative pathway.
HLA complex
Source – textbook of microbiology for dental students – harsh mohan
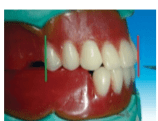
Placement of the maxillary first premolar in all three planes
side view
The buccal cusp tip of the maxillary first premolar is in contact with occlusal plane (black line), and palatal cusp 1 mm short of the occlusal plane
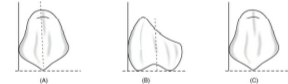
occlusal view
buccal cusp corresponds with the canine tip, and the palatal cusp corresponds to previous drawn reference line of the mandibular residual ridge line
front view
When viewed from: Front: Long axis parallel towards the vertical axis. Side: Long axis parallel towards the vertical axis. Occlusal plane: Buccal cusp is in contact with occlusal plane and palatal cusp 1 mm short of occlusal plane
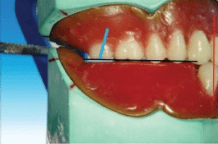
Steps in placement of the maxillary second premolar
Placement of the maxillary second premolar in all three planes
scoop out the waxocclusal relationside view
The buccal surface of the maxillary second premolar is barely visible when the patient smiles when viewed from the front
front view
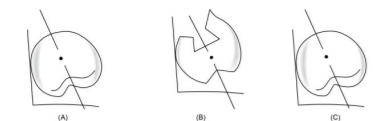
The buccal cusp of the maxillary second premolar corresponds with the buccal cusp of maxillary first premolar (blue line), and the palatal cusps of both the premolars correspond to the previous drawn line
When viewed from: Front: Long axis parallel towards the vertical axis. Side: Long axis parallel towards the vertical axis. Occlusal plane: Both buccal cusp and palatal cusp is in contact with occlusal plane
Steps in placement of maxillary first molar
Placement of the maxillary first premolar in all three planes
side viewfront view
the mesio- and distobuccal cusps correspond with the buccal cusp of second premolar (blue line) and the mesio- and distopalatal cusps correspond to the previous drawn line (yellow line).
When viewed from: Front: Long axis slopes buccally. Side: Long axis slopes distally. Occlusal plane: Only mesiopalatal cusp is in contact with occlusal plane
Steps in placement of maxillary second molar
The long axis of the maxillary second molar (blue line) is distally inclined in relation to the vertical axis (red line) when viewed from the front .
All the cusps are short of the occlusal plane (black line).
The maxillary second molar is slightly buccally inclined when viewed from the front. The buccal surface of the maxillary second molar is barely visible when viewed from the front
front view
When viewed from: Front: Long axis slopes buccally more steeply than first molar. Side: Long axis slopes distally more steeply than first molar. Occlusal plane: Only mesiopalatal cusp is nearest to occlusal plane
Source – S. Lakshmi preclinical manual of prosthodontics