🔻They are Lipopolysaccharide in nature and former integral part of the gram negative bacteria cell wall.
🔻 They are Heat stable.
🔻Form integral part of the cell wall; released only on disruption of bacterial cell.
🔻Weakly antigenic; antitoxin is not formed but antibodies against polysaccharide are raised.
🔻Cannot be toxoided.
🔻No enzymatic action.
🔻Non-specific action of all endotoxins.
🔻Low potency
🔻Non-specific in action.
🔻Usually produce fever.
🔻Produced by Gram-negative bacteria.
🔻 Massive gram negative septicemia may cause a syndrome of endotoxic shock characterized by fever, leukopenia, thrombocytopenia ,profound fall of blood pressure and circulatory collapse to death.
Exotoxins
🔻Protein (polypeptides) M.W. 10,000 to 900,000.
🔻 Heat labile (more than 60°)
🔻Actively secreted by living cells into medium.
🔻 Highly antigenic, stimulates formation of antitoxin which neutralises toxin.
🔻Converted into toxoid by formaldehyde.
🔻Enzymatic in action.
🔻Specific pharmacological effect for each exotoxin.
🔻Very high potency.
🔻Highly specific for particular tissue eg. tetanus toxin for CNS.
🔻Don’t produce fever in host.
🔻Produced mainly by Gram-positive bacteria and also by some Gram-negative bacteria.
Source- textbook of microbiology for dental students c p baveja
After the registration of the maxillo-mandibular , the artificial teeth must be set in centric occlusal position.
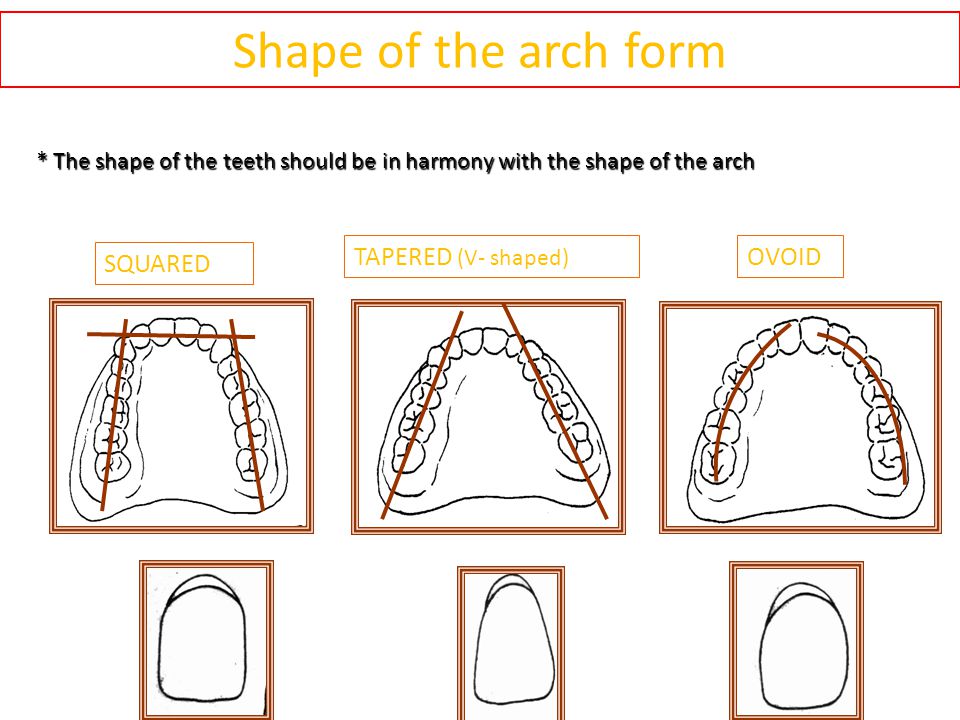
Selecting of artificial teeth
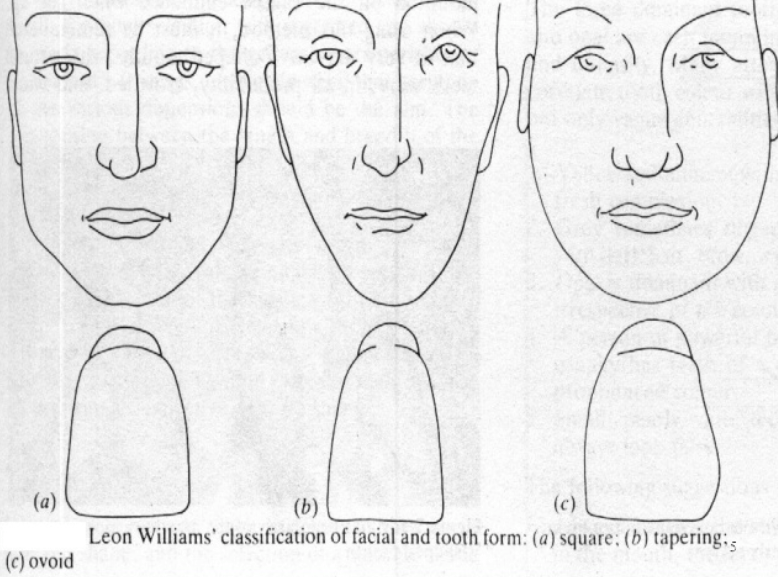
The facial form of the patient should be classified into-
–square
–ovoid
– tapering
-The form of the teeth should be in harmony with the form of the face, square teeth are used for those with a square face and so on.
-In addition, the patient’s age, gender and personality should be taken into consideration when trying to improve to improve the appearance.
-The color is also important, dark and opaque teeth should be selected for elderly patient, light and translucent teeth for the young patients.
-The size of the teeth must also be in harmony according to the size of the face and the gender of the patient.
Objectives of setting teeth are-
to provide a comfortable and atraumatic occlusion
to assist in preparing food for deglutition
to impart a pleasing and natural appearance
to assist in speech
Teeth arrangement of anteriors and posteriors
Armamentarium
•Maxillary occlusal rim with cast
• Mandibular occlusal rim with cast
• Mean value articulator
• Teeth shade
• Measurement scale
• Wax knife
• Roach carver
• Wax spatula
• Wax sheet
• Gas torch
• Cotton
• Rubber bowl with cold water
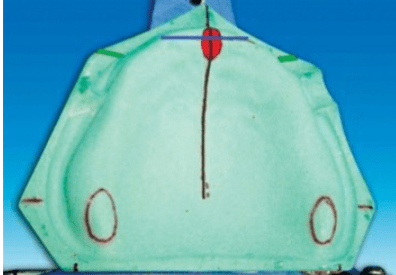
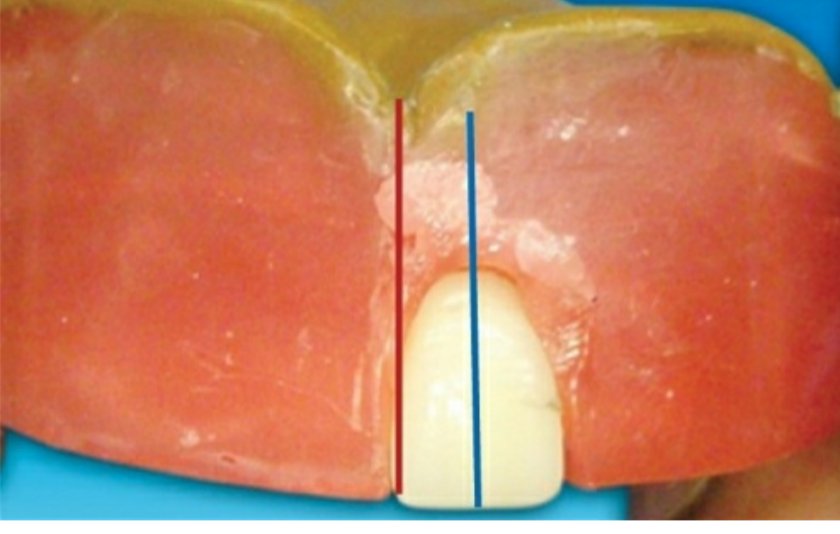
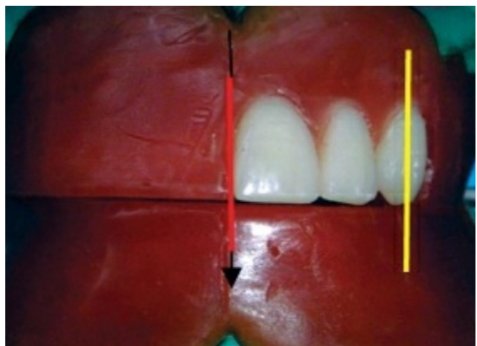
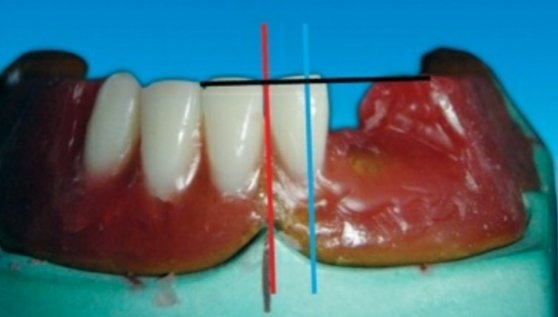
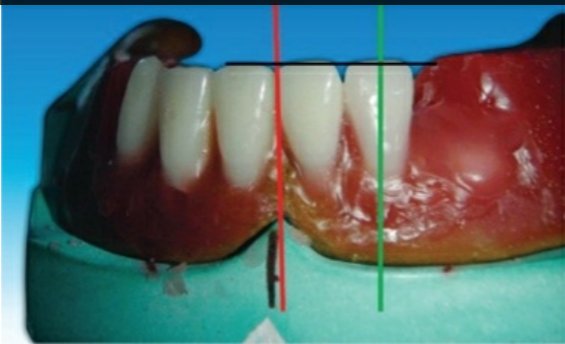
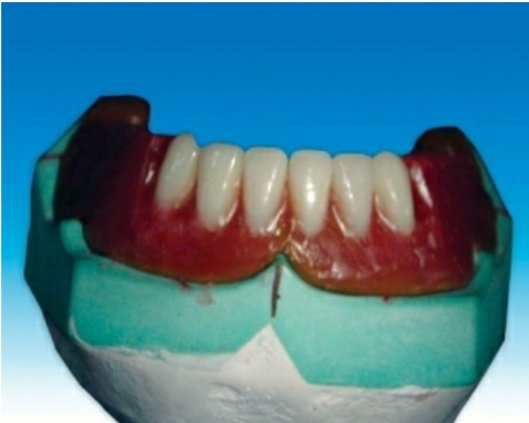
Guidelines for anterior teeth setting are marked on the cast and the land area of the cast.
I. The centre of the incisive papilla (marked in red)
II. A line is drawn along the midline of the cast through the centre of the incisive papilla (marked in black).
III. A perpendicular line is drawn to the above line through the centre ofincisive papilla till the land area (marked in blue; CPC line).
IV. During setting of maxillary canine, the cuspid tip of the canine should be placed in line with this point
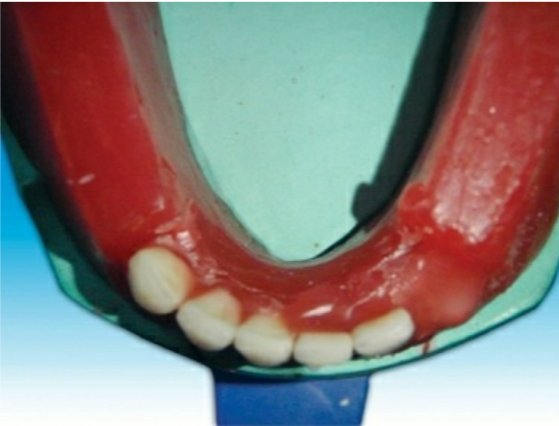
The crest of the lower residual alveolar ridge is marked in red colour along the posterior aspect of the lower cast. A corresponding line is marked on the upper cast in blue
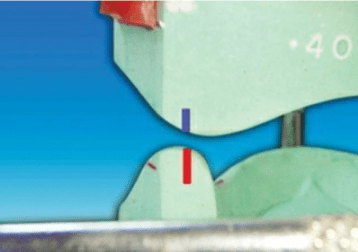
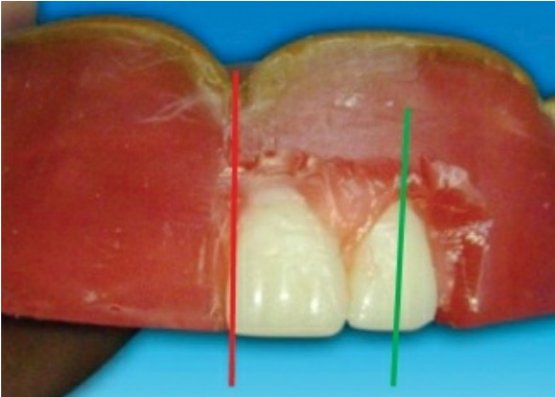
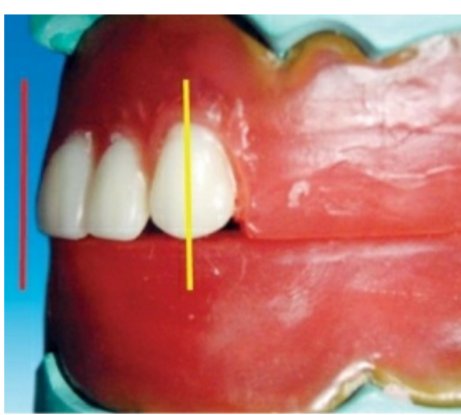
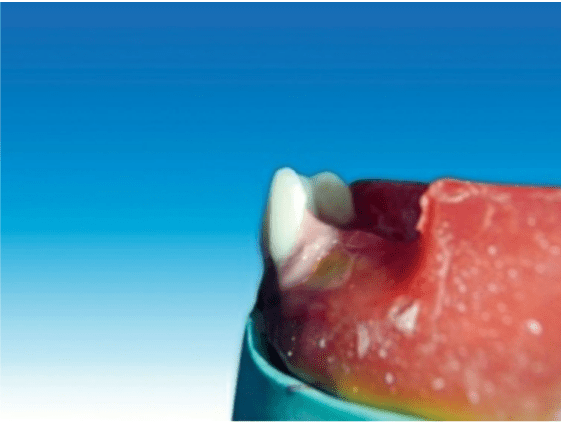
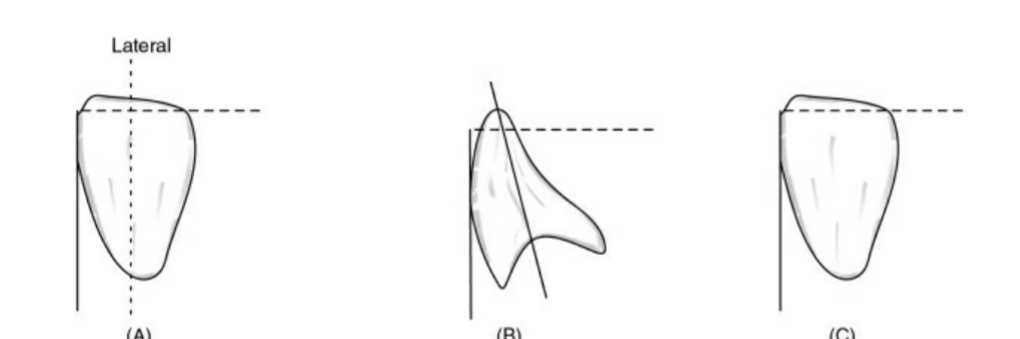
Steps in placement of maxillary central incisor
Placement of the maxillary central incisor in relation to all three planes.
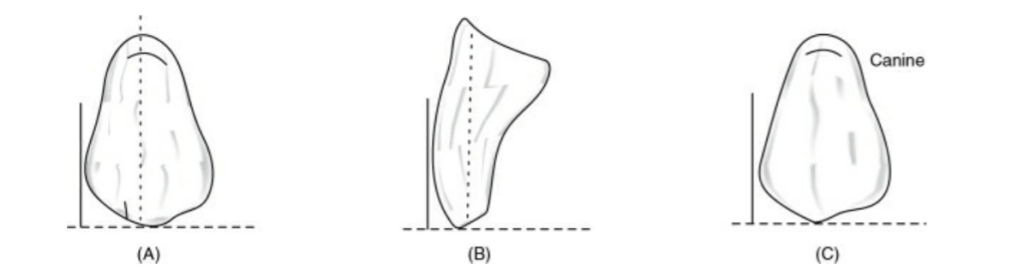
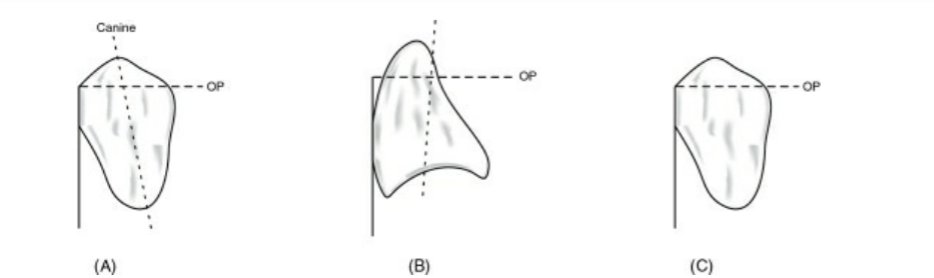
🔻The long axis of the central incisor (the blue line) is positioned parallel to the vertical axis (the red line) when viewed from the front
Front view
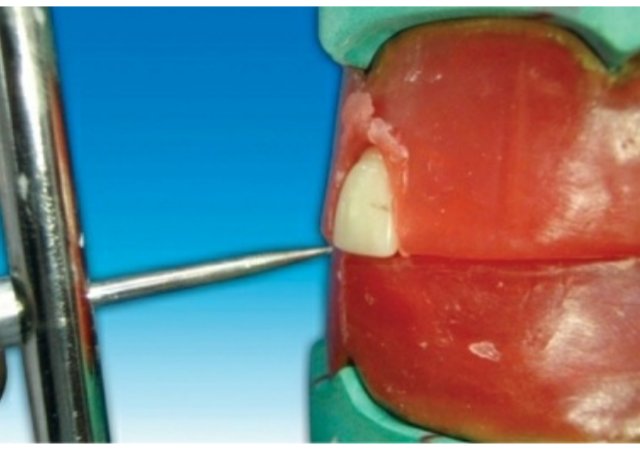
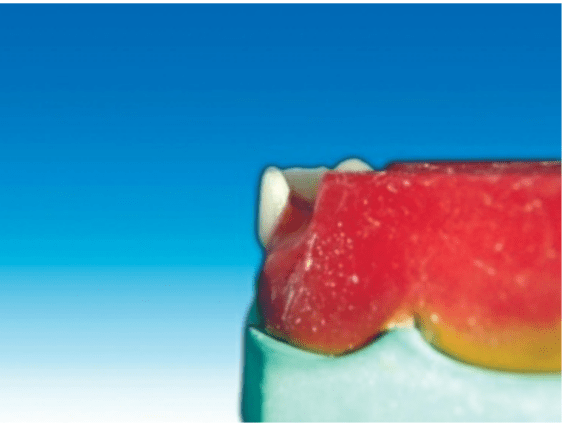
🔻The incisal edge of the maxillary central incisor is positioned in line with the anterior occlusal plane . The central pin of the articulator will point the mesioincisal line edge of the central incisor.
Side view
🔻The central pin of the articulator will point the mesioincisal line edge of the central incisor.
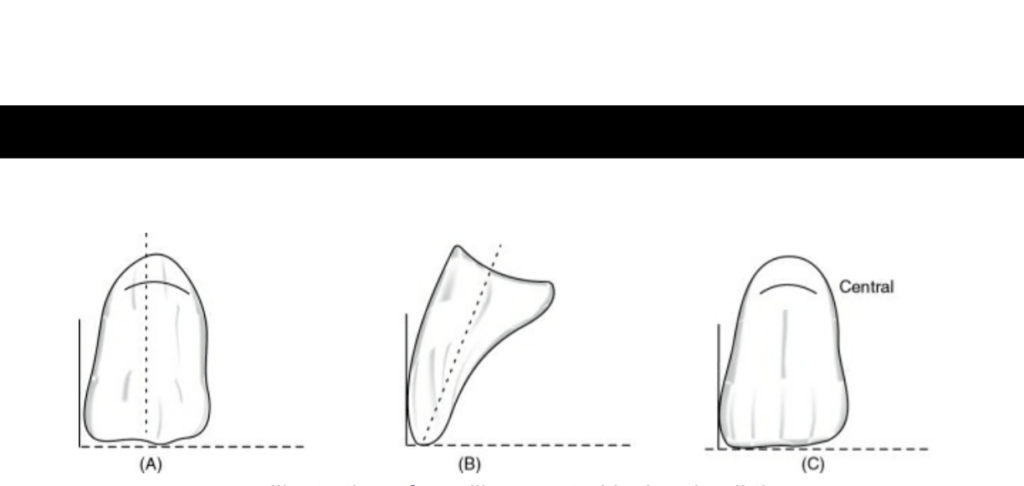
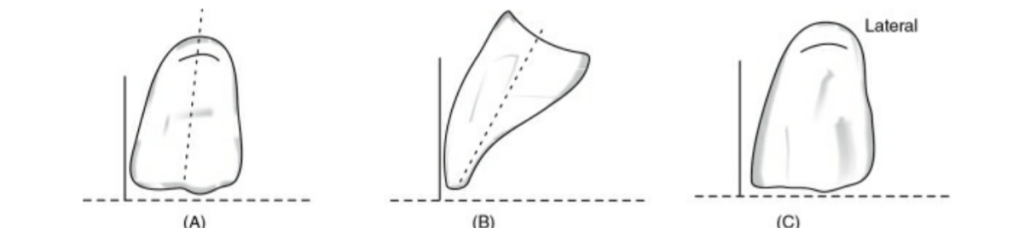
When viewed from: Front: Long axis parallel towards the vertical axis. Side: Slopes labially about 15 degrees. Occlusal plane: Incisal edge is in contact with occlusal plane
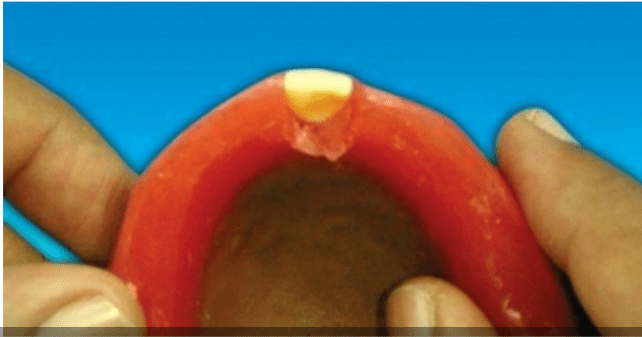
Occlusal view
Steps in placement of maxillary lateral incisor
Front view
🔻The long axis of the lateral incisor (green line) is placed slightly inclined to the vertical axis (red line).
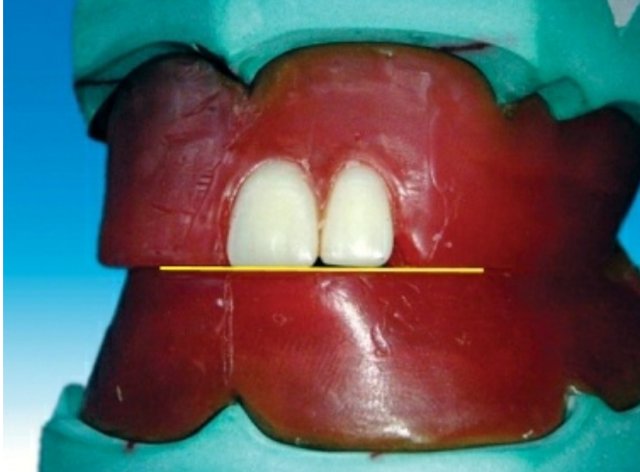
🔻The incisal edge of the maxillary lateral incisor is placed slightly short of the occlusal plane (marked as yellow line).
Side view
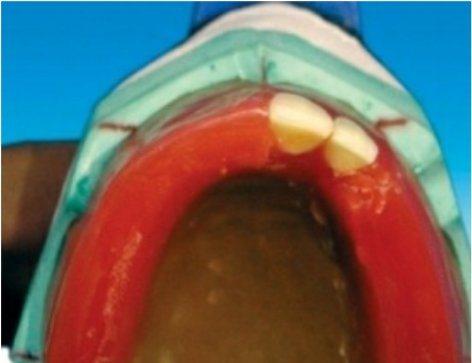
🔻The incisal edge of the maxillary lateral incisor should follow the outline of the occlusal rim when viewed occlusally
Occlusal view
When viewed from: Front: Long axis slopes towards midline at incisal edge. Side: Slopes labially about 20 degrees. Occlusal plane: Incisal edge is 1 mm short of occlusal plane
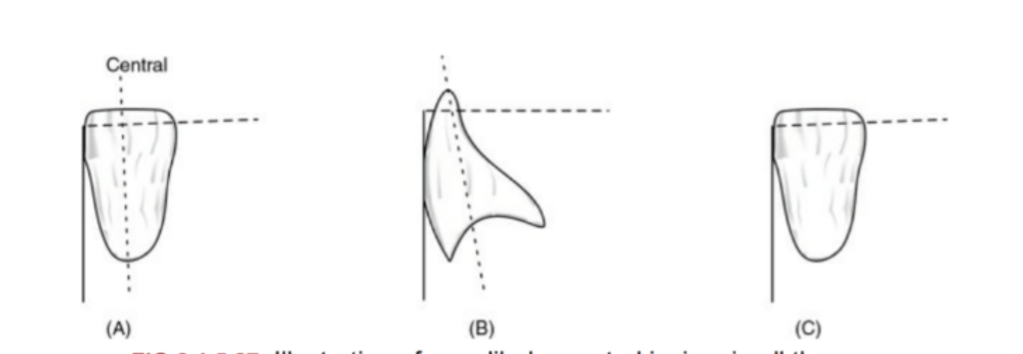
Steps in placement of the maxillary canine.
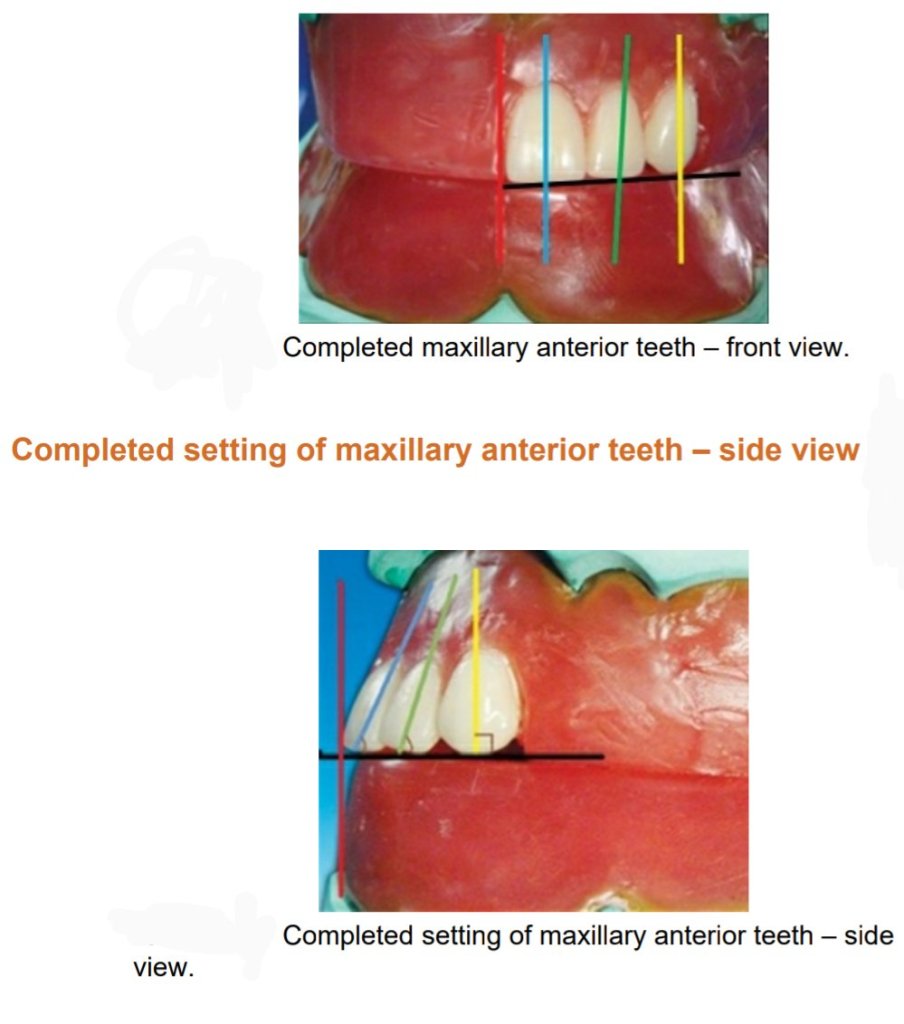
🔻The long axis of the maxillary canine (yellow line) should be parallel to the vertical axis (red line) when viewed from the front.
Front view
🔻The long axis of the maxillary canine (yellow line) should be parallel to the vertical axis (red line) when viewed from the side .
Side view
Maxillary canine follows the outline of occlusal rim, and the tip of the canine corresponds to the canine papillary line
Occlusal view
When viewed from: Front: Long axis parallel towards the vertical axis. Side: Long axis parallel towards the vertical axis. Occlusal plane: Cuspid tip is in contact with occlusal plane
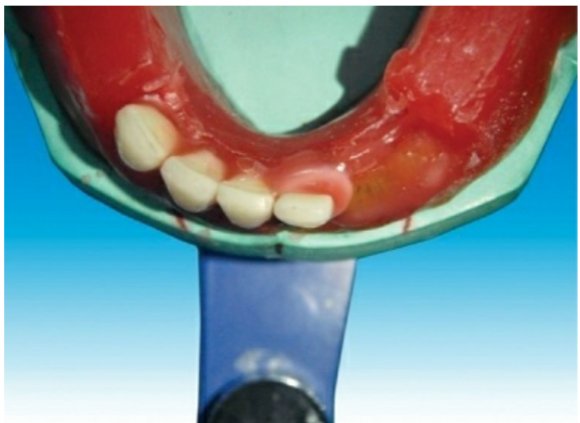
Teeth setting of anterior teeth
Steps in placement of mandibular central incisors
From front From side
🔻The incisal edge of the mandibular central incisor should follow the outline of the occlusal rim, and the incisal edge of the mandibular central incisor tooth should not cross over the land area when viewed occlusally
When viewed from: Front: Long axis inclines slightly towards the vertical axis. Side: Slopes labially. Occlusal plane: Incisal edge is 0.5–1 mm above the occlusal plane
Occlusal view
Steps in placement of mandibular lateral incisor
From front The incisal edge of the mandibular lateral incisor should follow the outline of the occlusion rim, and the incisal edge should not cross over the land area of the cast when viewed occlusally
When viewed from: Front: Long axis inclines towards the vertical axis. Side: Slopes labially less than central incisor. Occlusal plane: Incisal edge is 0.5–1 mm above the occlusal plane
Occlusal view
Steps in placement of a mandibular canine
From front From side From occlusal view
When viewed from: Front: Long axis inclined towards midline. Side: Slopes lingually. Occlusal plane: Cuspid tip is 0.5–1 mm above the occlusal plane
Maxillary and mandibular canine relation
The mesial slope of the maxillary canine should overlap the distal slope of the mandibular canine
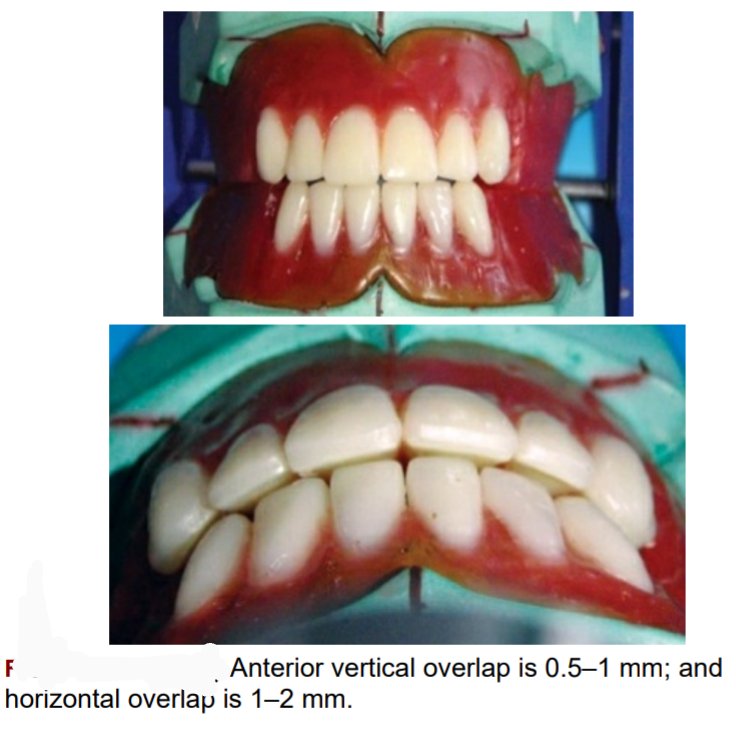
Complete teeth setting of maxillary and mandibular anteriors
🛑The vertical overlap (over bite) between the maxillary and mandibular incisal edge should be 0.5–1 mm, and the horizontal overlap (over jet) between the maxillary and mandibular incisal edges should be 1–2 mm.
🛑The horizontal overlap should be uniform from left maxillary to right maxillary canine
Source – preclinical manual of prosthodontics S . Lakshmi
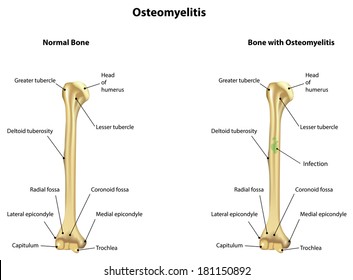
Definition: Osteomyelitis is defined as inflammation of the bone and marrow.
source -google
Classification
🔻Primary: Where bone is the primary solitary focus of disease .
🔻Secondary: Develops as a complication of any systemic infection.
Any infection (bacteria, viruses, parasites, fungi) may cause osteomyelitis but infections certain pyogenic bacteria and mycobacteria are the most common
Etiology
It is usually caused by bacteria.
• Most common pathogens are Staphylococcus species (aureus in 80-90% of the cases).
🔻Other organisms: Klebsiella, Neisseria gonorrhoeae, Haemophilus influenzae Escherichia coli, Pseudomonas, and Salmonella species
🔻Escherichia coli in patients with genitourinary tract infections or intravenous drug abusers.
Neonatal period:Haemophilus Influenzae and group B streptococci.
Patients with sickle cell disease: Salmonella infection.
• Mixed bacterial infections: It is due to direct spread or surgery or open fractures.
• In about 50%, no organisms can be isolated.
Portal entry of organisms
Causative organisms may reach the bone through the bloodstream, directly or extend from a contiguous site.
Hematogenous spread:
• Source of organisms may be a focus of infection anywhere in the body (e.g skin pustule or infected teeth and gums, intestinal mucosa).
• Minor injuries to the mucosa (vigorous chewing of hard foods, brushing of teeth), or minor infections of the skin, release these organisms into the blood → causing temporary bacteremia → reach the bone.
•In children (5 to 15 years) and drug addicts (infected needles), it develops in the long bones.
Direct implantation: Organisms may enter into bone by penetrating wounds, open fractures, or surgical procedures (staphylococci, streptococci, anaerobic organisms).
Spread from adjacent (contiguous) site: e.g. infections of the feet may spread into the bone in diabetics.
Location of infection: It varies with age.
• Neonate: Metaphysis, epiphysis, or both.
•Adult: Epiphysis and subchondral regions
•Children with hematogenous spread: Metaphysis of long bones (knee, ankle, and hip).
Pathogenesis and Morphology
The sequence of events and morphological features in osteomyelitis are described together.
• Transient bacteremia: Mild injury or trauma can initiate bacteremia by organisms (eg.Staphylococcus aureus).
•Infection reaches metaphysis long bone: Because in the metaphysis capillaries form loop – which slows the blood flow provides time for bacteria to penetrate blood vessel walls and establish infective foci within the marrow.
• Inflammatory Reaction: Once in bone, the bacteria grow and induce an acute inflammatory reaction with exudates.
• Necrosis of bone: Exudate increases the pressure on the adjacent vessels and further decreases the blood supply produces bone necrosis. The necrotic areas coalesce and allow further bacterial proliferation.
•Formation of sequestrum: Bacterial infections and pus spreads into the cortex and collects beneath the periosteum and may lift the periosteum and reduce the blood supply to the affected region.
The fragment of dead necrotic piece of bone, which is embedded in the pus, is known as a sequestrum.
source -google
What is a sequestrum ?
🔻The pus penetrates the periosteum and leads to a soft-tissue abscess may penetrate the skin form a draining sinus.
Hole formed in the bone during the formation of a draining sinus is known as cloaca
🔻The sinus tract may become epithelialized and may remain open, continually draining pus, necrotic bone, and bacteria.
Involucrum
After first week, chronic inflammatory cells become more numerous and the cytokines released stimulates osteoclastic bone resorption and deposition of reactive bone in the periphery.
Reactive new bone forms a sheath around the necrotic (segment of devitalized infected bone) sequestrum. This reactive new bone formed is known as involucrum.
Variants of osteomyelitis
• Brodie abscess: It is a distinctive form of subacute pyogenic osteomyelitis.
It appears as a small, solitary, intraosseous abscess localized to the metaphysis and is surrounded by reactive bone.
It may be due to inadequate treatment of infection by less virulent organisms.
source -google
• Sclerosing osteomyelitis of Garre – characterized by extensive newborn formation which obscures the underlying structure of the bone and typically develops in the jaw.
source -google
Complications
•Septicemia: From infection in the bone, organisms may disseminate through the blood stream and cause septicemia.
• Acute suppurative arthritis: Infection may spread through the articular surface into a joint producing suppurative arthritis may lead to destruction of the articular cartilage and permanent disability. It is more common in infants.
•Pathologic fractures.
•Squamous cell carcinoma: It may arise from the epithelialized sinus tract, rarely sarcoma of bone may develop.
• Secondary amyloidosis.
• Chronic osteomyelitis: It may develop due to delay in diagnosis, extensive bone necrosis, and inadequate therapy.
Clinical therapy
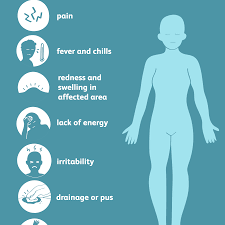
🔻 present with malaise, fever, chills , leukocytosis and throbbing pain over the affected area
source -google
🔻 Diagnosis-
Radiography- lytic focus of bone destruction
Blood cultures are positive
Biopsy and bone culture
source -textbook of pathology for dental students Harsh mohan
Chemical alteration of the drug in a living organism is called biotransformation.
The metabolism of a drug usually converts the lipid-soluble and unionized compounds into water-soluble and ionized compounds.
They are not reabsorbed in the renal tubules and are excreted. If the parent drug is highly polar (ionized), it may not get metabolized and is excreted as such.
Sites: Liver is the main site for drug metabolism: other sites are GI tract, kidney, lungs, blood, skin and placenta.
1.Active drug to inactive metabolite: This is the most common type of metabolic transformation
Conscious sedation is a level of CNS depression where a patient does not lose consciousness but is able to communicate and cooperate during the procedure/treatment.
Indications
•Uncooperative patients.
• Anxious patients.
• Emotionally compromised patients.
Conscious sedation should be avoided in:
• Chronic obstructive pulmonary disease.
• Pregnancy
• Prolonged surgery.
• Psychoses
Drugs used
Drugs used
Benzodiazepines
Diazepam is the most commonly used drug for conscious sedation.
Small doses (1-2 mg) of diazepam is administered intravenously slowly. It can also be administered orally.
Midazolam is a short-acting BZD given intravenously. Temazepam is given orally. It is safe and has better patient compliance.
Nitrous oxide + oxygen: Nitrous oxide is given by inhalation route along with 100% oxygen.
Propofol( i.v. infusion), fentanyl (i.v.), etc. can also be used for conscious sedation.
Precautions
• Written informed consent should be obtained from the patient prior to the procedure.
• Conscious sedation should be administered by trained personnel.
• Constant monitoring of the vital signs should be done during and after the procedure.
• The procedure should be documented. Postoperative instructions should be in written form.
• Equipment and emergency drugs should be kept ready to tackle any emergency • Patient should be escorted by an attendant.
Source- textbook of pharmacology for dental students – Tara V Shanbhag
Systemic glucocorticoids: Intravenous hydrocortisone 200 mg i.v stat followed by a hydrocortisone 100mg or oral prednisolone 30-60 mg day, depending on the patient’s condition
Intravenous fluids to correct dehydration
Potassium supplement: To correct hypokalemia produced by repeated dose of salbutamol or terbutaline.
Paracetamol is effective by oral and parenteral routes. It is well absorbed, widely distributed all over the body, metabolized in liver by sulphate and glucuronide conjugation. The metabolites are excreted in urine.
Uses
1.As an antipyretic– reduces body temperature
2.as an analgesic to relieve headache , toothache, bodyache
2. Preferably used in asthmatics patients with peptic ulcers , hemophilia
Adverse effects
Side effects are rare, occasionally causes skin rashes and nausea.
Hepatotoxicity: with acute overdose or chronic use.
Nephrotoxicity is commonly seen on chronic use.
Acute paracetamol poisoning
Acute overdose mainly causes hepatotoxicity the symptoms are –
nausea, vomiting, diarrhea abdominal pain, hypoglycaemia, hypotension, hypoprothrombinemia, coma, etc.
Death is usually due to hepatic necrosis.
Mechanism of toxicity and treatment
1.The toxic metabolite of paracetamol is detoxified by conjugation with glutathione and gets eliminated.
2.High doses of paracetamol cause depletion of glutathione levels. In the absence of glutathione, toxic metabolite (NAPQI) binds covalently with proteins in the liver and kidney and causes necrosis. Alcoholics and premature infants are more prone to hepatotoxicity.
3.N-Acetylcysteine or oral methionine replenishes the glutathione stores of the liver and protects liver cells.
4.Activated charcoal is administered to decrease the absorption of paracetamol from the gut. renal failure.
5.Haemodialysis may be required in cases with acute renal failure.
Source – textbook of pharmacology for dental students- Tara Shanbhag