•When tooth eruption is impeded, surgical removal of the excessive tissue and exposure of the teeth are indicated.
•The cosmetic appearance may also require surgical excision.
•The lesion sometimes recurs. It has been reported that tooth extraction alone will cause the tissues to shrink almost to normal and that recurrences can be prevented by this.
Source- textbook of oral pathology Shafers and Google images
Rather this can be called a developmental anomaly.
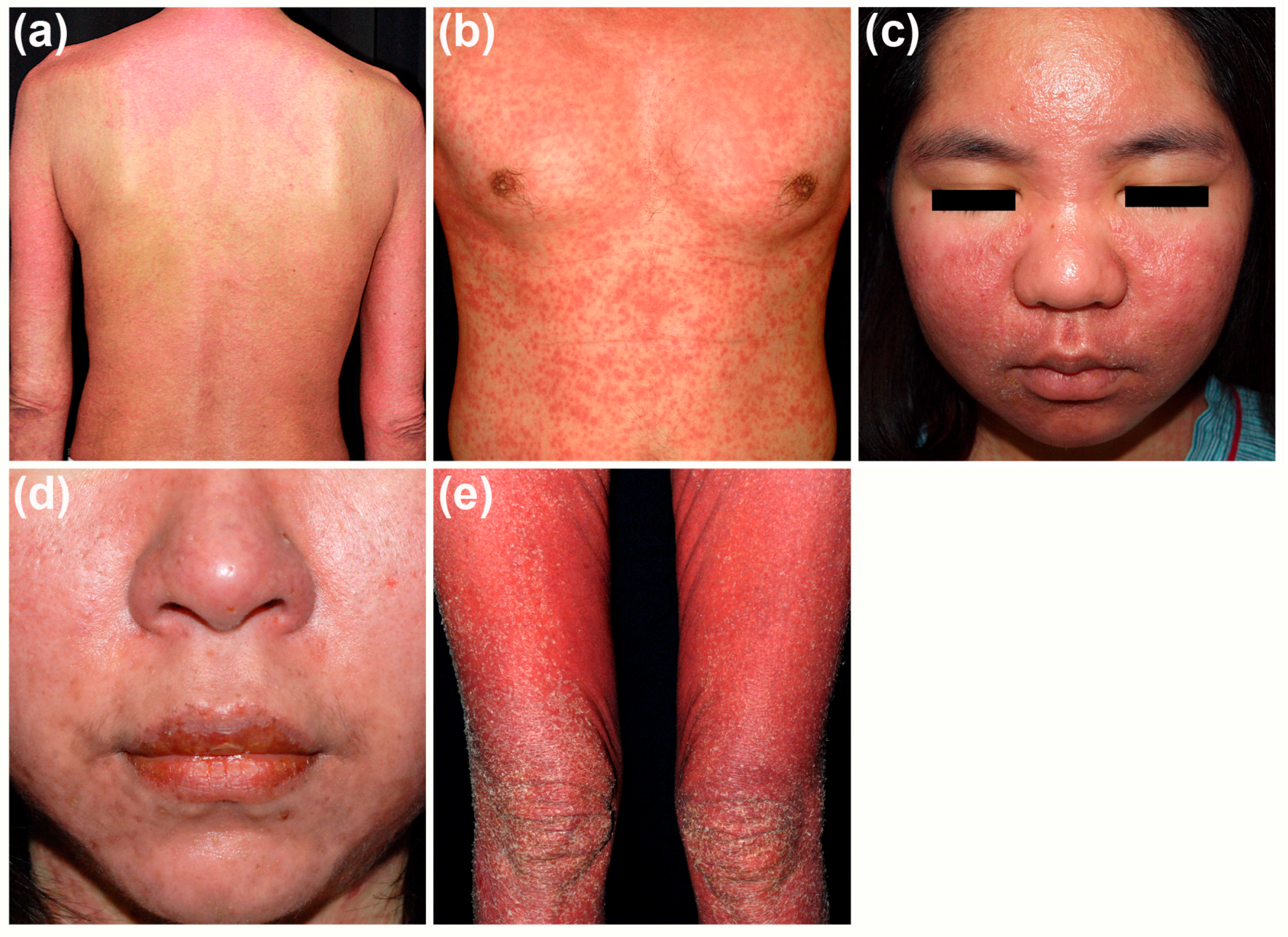
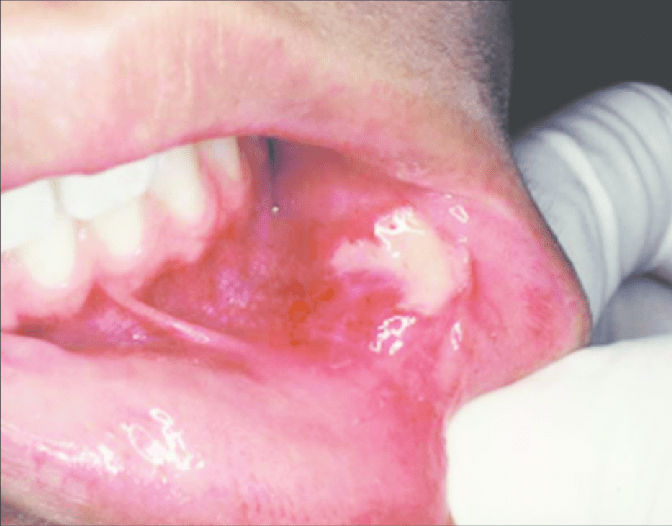
It is characterised by heterotopic collection of sebaceous glands in various sites of the oral cavity.
It is said that the occurance of sebaceous glands in the mouth may be by inclusion in the oral cavity of the ectoderm.
This has some of the potentialities of skin during the development of the maxillary and the mandibular processes during the embryonic life.
Clinical features-
1.Appearance-
as yellow spots, seperated
or forming large plaques
project slightly above the suface of tissue
2. Site of appearance- found frequently in a bilateral symmetical pattern
mucosa of cheeks (opposite the molar teeth)
inner surface of lips
retromolar region
tongue
gingiva
palate
frenum
Besides the oral cavity they also appear in the oesophagus ,the female genital tract ,cervix uteri, male genitilia ,nipples, palms ,soles ,parotid ,larynx and the orbit .
3. Usually seen more in adults than children . This is due to the better development of sebaceous glands and hair system is not seen until puberty.
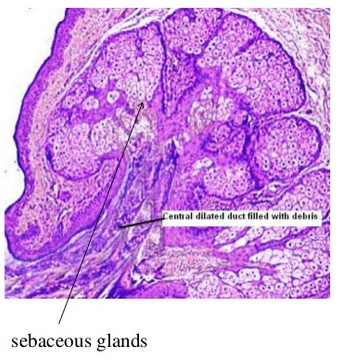
Histology
These are heterotopic collection of sebaceous glands and they are identical with those that are seen in the skin.
But they are unassociated with hair follicles and hair shaft from the gingiva. (this may be a very rare occurance )
Glands are located superficially.
There may be few or many lobules.
They are grouped around one duct or more ducts and they open at the surface of the mucosa .
The ducts may show keratin plugging.
Treatment-
It requires no treatment.
source – textbook of oral pathology shafers and google images .
Defined as physiological wearing away of tooth structure.
This phenomenon is more physiological than pathological
🛑SITES OF OCCURRENCE-
occlusal surface
incisal surface
proximal surface
It is also associated with the aging process.More the older the person gets more it regresses
🛑MAIN CAUSE-Tooth to Tooth contact during Mastication
It is seen in deciduous as well as in permanent dentition.
🛑Types of attrition
🔸Physiological attrition: Attrition which occurs progressively during normal aging process as a result of masticatory occlusion. Usually a slow process through out life .
🔸Pathological attrition: This is a severe form of attrition that occurs as a result of abnormalities in occlusion ,chewing pattern and structural defects in teeth .
Examples are bruxism or clenching
🛑AETIOLOGY
Abnormal chewing habits: Parafunctional chewing habits like Bruxism and chronic persistent chewing of coarse foods or other substances like tobacco.
In other occupations workers are exposed to an atmosphere of abrasive dusts e.g. silica
Amelogenesis imperfecta and dentinogenesis imperfecta in which the hardness of enamel and dentine is reduced and such teeth become more prone to attrition and is seen in children
🛑Clinical presentation –
Appearance of small polished facet on the cusp tip /ridge or slight flattening of the incisal edge
Sensitivity and pain : attrition may be entirely asymptomatic or there may be dentine hypersensitivity.
Tooth discoloration : attrition and erosion of the enamel exposes inner and darker dentine giving a yellower appearance
Compromised periodontal support leading to drifting of teeth
Altered occlusion due to decreasing occlusal vertical dimension
Men usually have more attrition than women as a result of greater masticatory force .
Also variations are seen with the coarseness in diet and chewing tobacoo
advanced attrition
Sources -textbook of oral pathology – shafers, slide share , pictures – google photos.