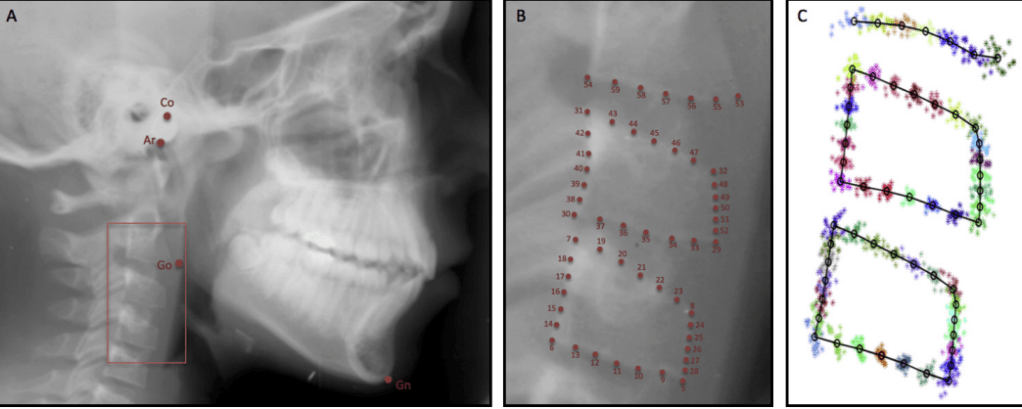
CVM Basics
- Vertebrae used: C2, C3, C4
- Visible on lateral cephalogram (no extra radiation)
- Traditionally used to estimate skeletal maturity & mandibular growth peak
CVM Stages (Baccetti et al.)
- CS1 – Inferior borders of C2–C4 flat; bodies trapezoidal.
- CS2 – Concavity begins at C2 lower border.
- CS3 – Concavity at C2 & C3; bodies less trapezoid.
- CS4 – Distinct concavities at C2–C4; bodies nearly rectangular.
- CS5 – Strong concavities; square vertebrae.
- CS6 – Deep concavities; taller than wide.
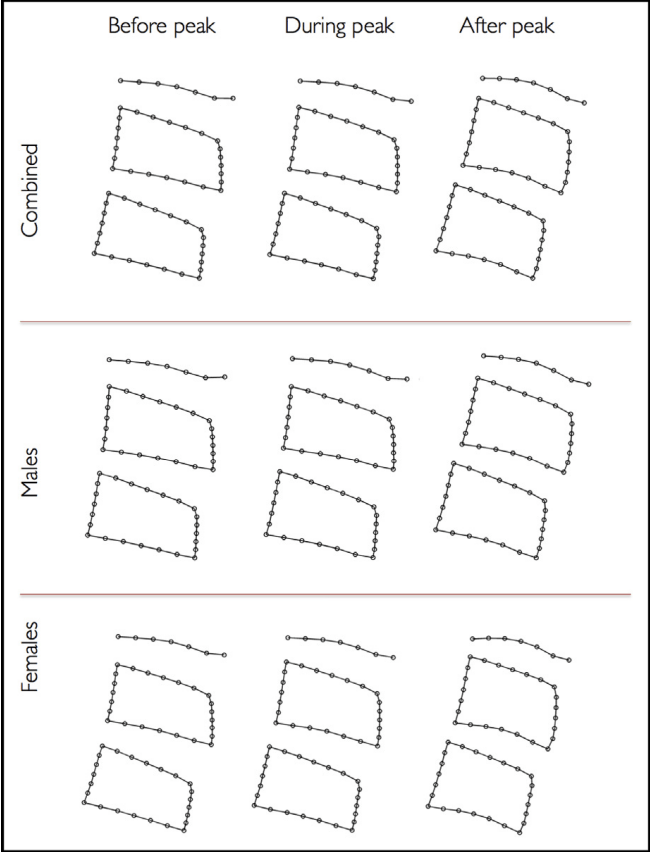
CVM Shape Changes with Age
- C2–C4 Inferior Borders → Concavity increases with age
- C3 & C4 Height → Becomes taller, shape transitions trapezoid → rectangular/square
- Sex Difference: Girls reach each stage earlier than boys

Study Findings (Gray et al., 2016)
✅ Morphometric changes match classic CVM descriptions
❌ CVM stages did not reliably predict mandibular growth peak
👉 Growth peak often occurred before or after CS3, not always between CS3–CS4
Peak mandibular growth: typically occurs around CS3, but study shows high variability:
- 32% after CS3
- 28% after CS1
- 20% after CS2
- 20% after CS4
- No growth peak at CS5 or CS6
Clinical Pearls
- CVM can confirm if peak growth has passed, but
- Chronologic age is often a better predictor than CVM alone
- Always combine with:
- Secondary sex characteristics
- Height/weight velocity
- Dental development
- Clinical growth indicators
📌 Quick Rule of Thumb
- Before CS3 → Growth spurt may still be coming.
- At CS3 → Possible growth peak (but variable).
- After CS4 → Growth peak has passed.
Clinical MCQs – Cervical Vertebrae & Mandibular Growth
Q1.
A 12-year-old boy presents for orthodontic evaluation. His lateral cephalogram shows concavity in the inferior borders of C2 and C3, but not yet in C4. The vertebral bodies are less trapezoid, approaching rectangular.
What can be inferred about his mandibular growth peak?
A. Growth peak is most likely already passed
B. Growth peak is occurring now or will occur soon
C. Growth peak cannot occur at this stage
D. Growth peak will only occur at CS5–CS6
Answer: B
Explanation: Concavities at C2 and C3 correspond to CS3, which is often associated with the timing of peak mandibular growth. However, variability exists (some peak after CS1, CS2, or CS4).
Q2.
During a growth assessment, a girl’s cephalogram shows all three cervical vertebrae (C2–C4) with distinct concavities, and the vertebral bodies appear rectangular and taller. She is 14 years old.
What is the most likely clinical implication?
A. She is approaching mandibular growth peak
B. She is currently at growth peak
C. She has already passed mandibular growth peak
D. She will have another growth spurt at CS6
Answer: C
Explanation: Distinct concavities and rectangular vertebrae (CS4 or later) suggest the growth peak has passed.
Q3.
Which of the following statements best reflects the findings of the study?
A. CVM staging alone is a reliable predictor of mandibular growth peak
B. Morphometric analysis can clearly differentiate “before” and “during” mandibular growth peak
C. Chronologic age is a better predictor of mandibular growth peak than CVM stage
D. Mandibular growth always occurs after CS3
Answer: C
Explanation: The study found chronologic age correlated more consistently with mandibular growth than CVM staging. Morphometric differences were only clear after the peak, not before vs during.
Q4.
An orthodontist uses CVM staging to plan functional appliance therapy in a boy. His CVM stage is CS3. According to the study, what percentage of children actually reach peak mandibular growth after CS3?
A. 20%
B. 28%
C. 32%
D. 50%
Answer: C
Explanation: Only 32% of participants reached peak mandibular growth after CS3, highlighting variability.
Q5.
Which of the following sex differences were observed in the study regarding mandibular growth peak timing?
A. Boys reached peak earlier (mean 11.7 yrs) than girls (mean 12.8 yrs)
B. Girls reached peak earlier (mean 11.7 yrs) than boys (mean 12.8 yrs)
C. No sex differences were found in timing of growth peak
D. CVM stage timing was identical in both sexes
Answer: B
Explanation: Girls reached mandibular growth peak earlier (mean 11.7 years) than boys (12.8 years).