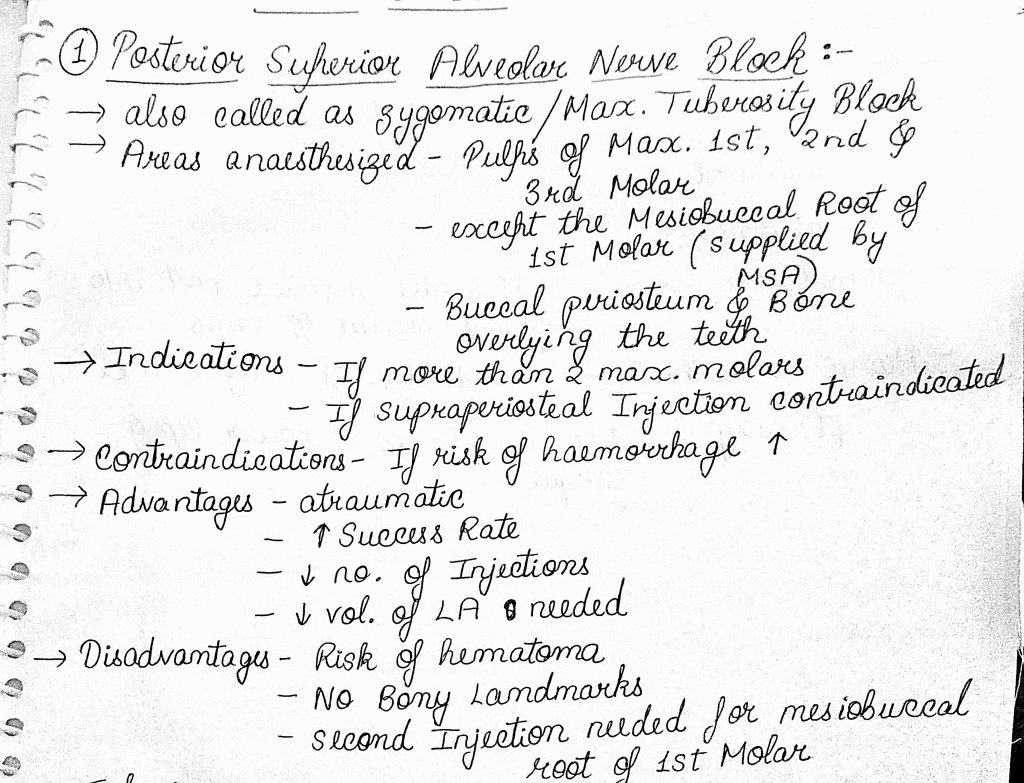


Reference-
Handbook of local anaesthesia by Stanley F. Malamed
Reference-
Handbook of local anaesthesia by Stanley F. Malamed
In general, there are two types of Dental indices.
The first type of index measures the ‘number’ or ‘proportion ‘ of people in a population with or without a specific condition at a specific point in time or interval of time.
The send type of Dental index measures the ‘number of people affected’ and the ‘severity’ of a specific condition at a specific time or interval of time.
1.Based upon the direction in which their scores can fluctuate:
▪️Irreversible index:
An index that measures conditions whose scores will not decrease on subsequent examinations. Eg: DMFT index.
▪️Reversible index:
An index that measures conditions that can increase or decrease on subsequent examinations. Eg: Loe and Silness gingival index.
2.Depending upon the extent to which areas of oral cavity are measured
▪️Full mouth indices:
These indices measure the patient’s entire periodontium or dentition. Eg: Russell’s Periodontal Index
▪️Simplified indices:
These indices measure only a representative sample of the dental apparatus. Eg: Greene and Vermillion’s Oral Hygiene index – Simplified
3.Indices may be classified under certain general categories according to the entity which they measure
▪️Disease index:
The ‘D’ (decay) portion of the DMFT index best exemplifies a disease index.
▪️Symptom index:
The indices measuring gingival/sulcular bleeding are essentially symptom indices.
▪️Treatment index:
The ‘F’ (filled) portion of the DMFT index best exemplifies a treatment index.
4.Dental indices can also be classified under special categories as,
▪️Simple index
An index that measures the presence or absence of a condition. Eg: Silness and Loe Plaque Index
▪️Cumulative index:
Am index that measures all the evidence of a condition, past and present. Eg:DMFT index for dental caries.
References:
Textbook of Public Health Dentistry – Soben Peter 6th edition.
Also known as Auriculotemporal syndrome or Gustatory sweating, it is an unusual phenomenon which arises as a result of damage to the auriculotemporal nerve and subsequent reinnervation of sweat glands by parasympathetic salivary fibers.
Etiology: This syndrome follows some surgical operation (area involving auriculotemporal nerve) , during which the damaged nerve regenerates, parasympathetic nerve supply develops, interacting sweat glands, which then function after salivary, gustatory, or psychic stimulation.
Clinical features: Patient typically exhibits flushing and sweating of the involved face, mainly temporal region, during eating.
Profused sweating can be evoked by parenteral administration of pilocarpine or eliminated by administration of atropine or a prominent block of auriculotemporal nerve.
The syndrome is a possible complication of parotitis, parotid tumor, ramus resection, mandibular resection for correction of prognathism. It has been reported as a complication in as high as 80% of cases following parotidectomy.
Treatment: Intracranial division of auriculotemporal nerve.
Reference: Shafer’s Textbook of Oral Pathology, 9th edition.
Defn and classification:-

Ventricular Septal Defect


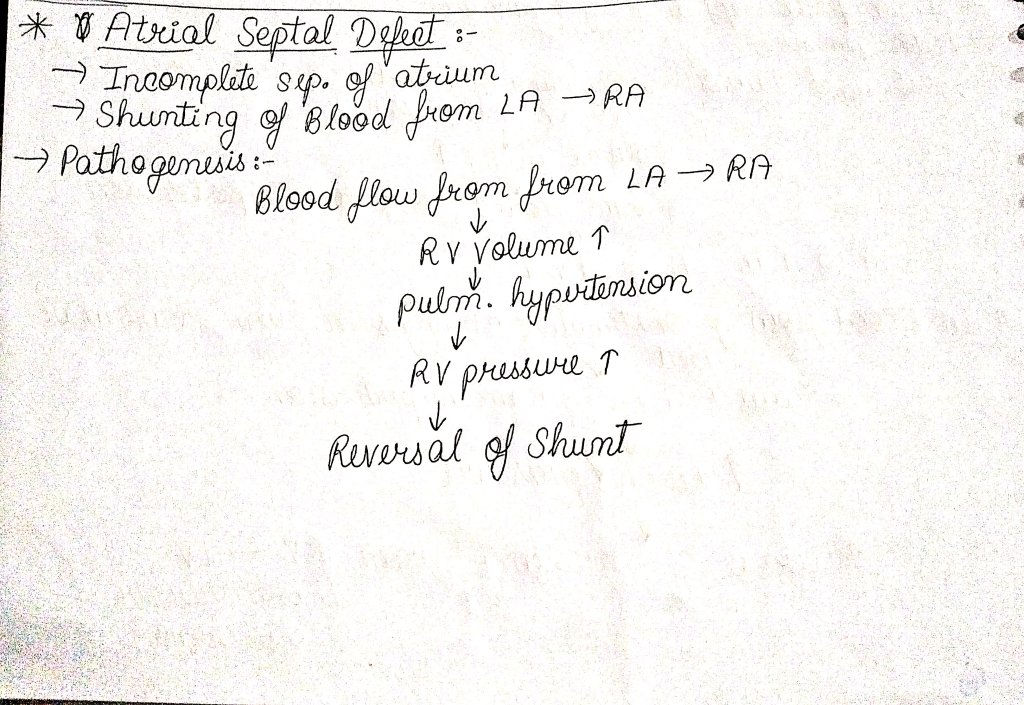
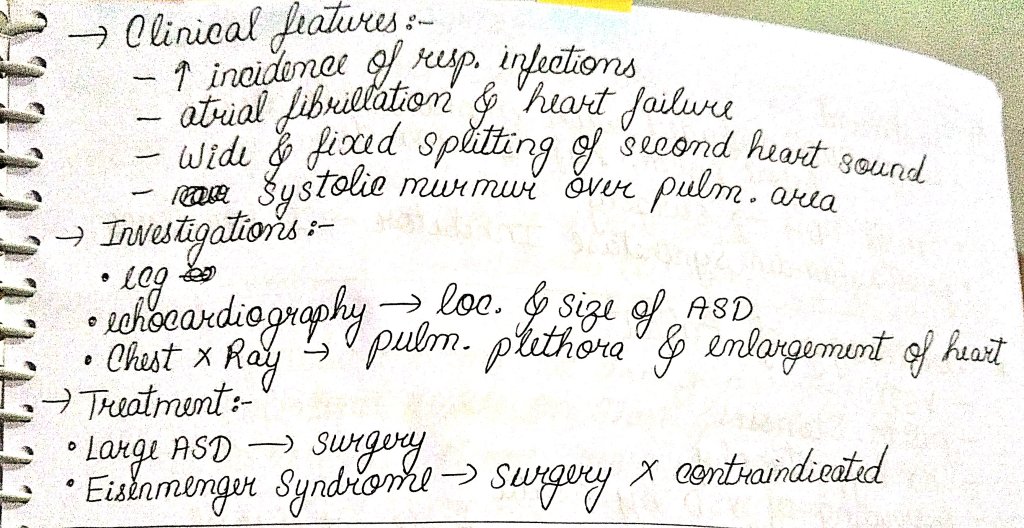
Atrial Septal Defect
Patent Ductus Arteriosus

Teratology of Fallot (imp saq)

Reference- a.k. tripathi for general medicine
Parry-Romberg syndrome is also called as facial hemiatrophy. It is slowly progressive atrophy of the soft tissues of half of the face and also progressive wasting of subcutaneous fat with atrophy of skin,cartilage,bone and muscle.
extraction of teeth
local trauma
infection
genetic factors
disruption of stapedial artery
SEX: females are more affected than males with ratio of 3:2
AGE: occurs generally in the first decade
SITE: Mostly occurs on the left than the right side
CLINICAL PRESENTATION-
It is a painless cleft near the midline of the face or forehead.
Marks the boundary between normal and atrophic tissue.
Bluish hue may appear in the skin overlying atrophic fat.
The affected area extends with atrophy of skin,cartilage,alveolar bone and soft palate on that side of the face.
facial wasting: ipsilateral salivary glands and hemiatrophy of the tongue,unilateral involvement of the ear,larynx,oseophagus,diaphragm,kidney and brain.
No specific treatment but cosmetic surgeries are recommended.

Clasps are the retentive components of the removable appliances.

Mode of action-
Adams clasp also called as universal clasp, liverpool clasp and modified arrowhead clasp.
Parts of adams clasp-
Advantages of adams clasp-
Modifications of adams clasp-
Reference- Bhalajhi 7th edition
Its an uncommon condition which occurs from occlusion of hepatic vein or inferior vena cava . it may be acute but usually is chronic.
Budd-Chiari Syndrome may also cause other conditions, including:
As promised here is meself pretending like its Decemeber 2020 and there is nobody more fired up for fourth year exams than me. 🥲
It’s so very easy to get caught up in downward spiral of self doubt and past failures, even though I try to be as optimistic as I can..I am not immune to it. So, I lost few days to overthinking and worrying but not anymore.
I believe a lot of us are in the same position, we want to do our best, we want to study for many many hrs a day, we want to get done with our daily targets but there is some invisible force stopping us, making us give half hearted attempts at everything we try to do.
As for the identity of this invisible force, I believe its fear and self doubt and a feeling of being alone in our struggle, all these cloaked and disguised so that we cant figure out how to fight it.
But I have figured it out, like I mentioned before I have a superawsome brain, (it might not fetch me a cool rank in exam but it does other really wonderful things). 😂😂
So, here is my plan to fight off these invisible forces and make room for the possibility of a bright future –
.
🧠 Forget about strategies, just read, anything, all the time, if boring subjects are giving you a hard time, switch immediately, there is no time to waste.
🧠 7 hrs a day is a must!
🧠 I will focus on strengthening the 80% syllabus that will get me 70% scores
🧠 Watching 2 to 3 video lectures on a daily basis especially live classes or interactive classes, especially of your fav teachers or subjects will give you enough boost!
🧠 Encourage and support each other, that’s the best way to not succumb to despair.
YOSH!
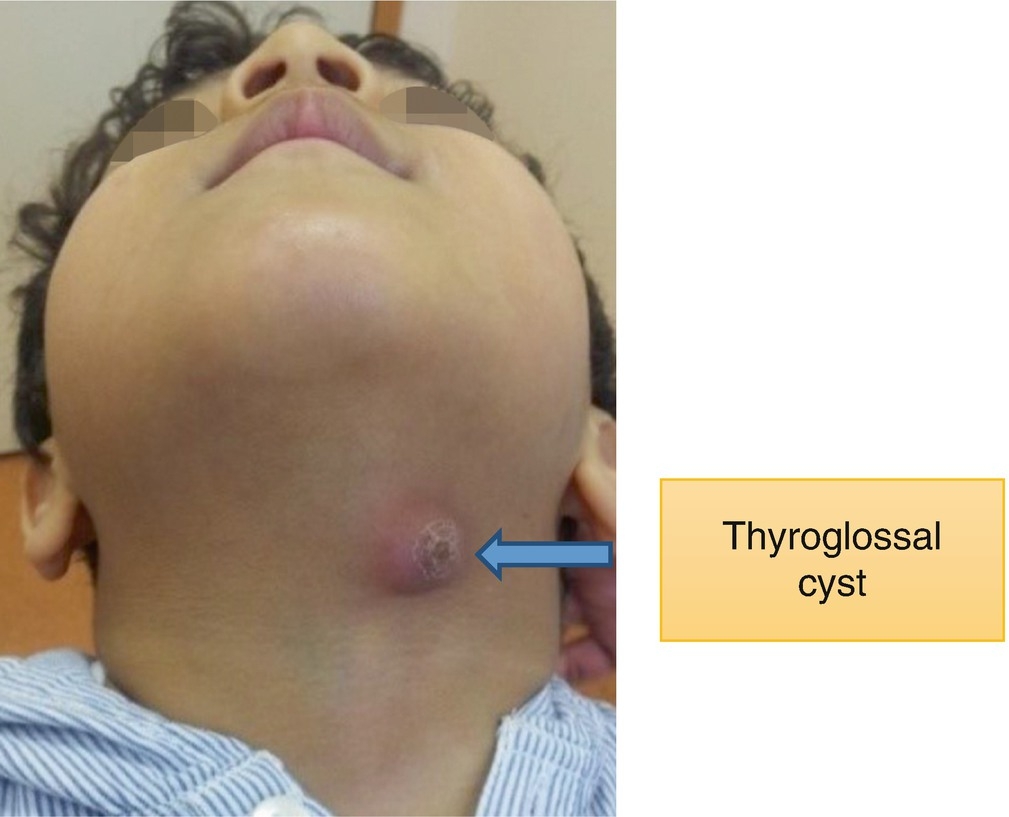
A thyroglossal cyst is a fibrous cyst that forms from a persistent thyroglossal duct. Thyroglossal cysts can be defined as an irregular neck mass or a lump which develops from cells and tissues left over after the formation of the thyroid gland during developmental stages