A pear-shaped and well-circumscribed radiolucent lesion with a corticated outline was found on a radiograph related to the root of an upper central incisor. The tooth was not restored and proved vital on testing.
A nasopalatine duct cyst is a specific type of cyst that develops from remnants of the nasopalatine duct. During embryonic development, this duct is involved in the formation of the nasal and oral cavities. Sometimes, remnants of this duct can persist and give rise to a cystic lesion later in life.
The nasopalatine duct extends from a structure called the incisive canal, which is located in the midline of the maxillary bone (the bone that comprises the upper jaw). The cyst can develop anywhere along this tract.
When we examine the lining of a nasopalatine duct cyst under a microscope, we typically observe the presence of both respiratory and squamous epithelium. This finding is significant because it indicates the origin of the cyst from the nasopalatine duct. The respiratory epithelium represents the lining of the nasal portion of the duct, while the squamous epithelium represents the lining of the oral portion.
Furthermore, a nasopalatine duct cyst often contains a neurovascular bundle within its capsule. This bundle consists of nerve fibers and blood vessels that supply the nasopalatine area. Its presence within the cyst is a characteristic feature.
In clinical practice, nasopalatine duct cysts are usually asymptomatic and are often discovered incidentally during routine dental examinations. However, if the cyst becomes large or infected, it can cause pain, swelling, and discomfort in the affected area.
As a dental student, it’s important to be familiar with the clinical presentation, radiographic appearance, and management of nasopalatine duct cysts. Treatment typically involves surgical removal of the cyst to relieve symptoms and prevent potential complications.
Chronic pulpal infection = rarefaction at bony furcation
Carious involvement = Radiolucency in the furcation area
ACUTE ALVEOLAR ABSCESS (TRUE STATEMENTS)
Primary tooth = more diffuse
A localized collection of pus at root apex in alveolar bone
There is swelling, mobility and elevation of a tooth from its socket
Pulse oximetry
Measures the pulpal circulation directly
TRUE STATEMENTS
Objective test
Measures and compares amplitudes of ratios of transmitted infrared light with red light
Capable of evaluating the stature of blood vasculature
Depends on pulsatile blood flow
Laser doppler flowmetry
Based on the velocity of RBC cells in capillaries
A non-invasive method to measure blood flow
GAZELIUS
Indirect Pulp Therapy
Objective = Eliminate the removal of deep caries
Indicated (imp)
in primary molars when the carious lesion is suspected of producing an exposure of the pulp
when there is no history of spontaneous pain = Tooth must be asymptomatic
IPT = It is dependent on the remineralisation of affected dentin and reparative dentin formation
The success of IPT = placement of temporary restoration with excellent sealing properties
Most ideal material = Calcium hydroxide
Introduced by FAUCHARD
When applied to residual carious dentin = it remains for6 – 8 weeks
Following amputation of the coronal portion of the pulp of an immature permanent first molar = the stump is capped with CaOH
The success of CaOH pulpotomy is determined by = Continuation of root formation and apexogenesis
Dentin bridge is formed =at a level slightly below the amputation
Direct Pulp Therapy
Amount of repartive/3* dentin formed after 30 days = 1.5 microns/day and then slows down after 48 days
Contraindicates in primary teeth
Prognosis is best = mechanically exposed permanent tooth
Indicated in cases of little (Pinpoint exposure = less than 1 mm) or no haemorrhage from the exposure site
The pulp should be vital
Done in traumatic or iatrogenic cases = Reported within 24 hours
High rate of failure = high cellular content of pulp
Pulpotomy
The simplest form of pulp therapy
Contraindicated = If there is Inflammation of radicular pulp and pain
Mechanicalexposure of mesiobuccal pulpal horns in primary maxillary 1st molar with moderate caries lesion on the mesial-distal surface = formocresol PULPOTOMY + stainless steel CROWNS
Pulp preservative material and best = MTA
The primary function of MTA = Apexification of immature traumatised pulpless tooth
Important criteria of success = Root end completion
Formocresol Pulpotomy
SWEET
Composition of Buckley Solution
1:2 parts F: C
19% formaldehyde
13% cresol
15% glycerine
Successful treatment for vital primary second molar with a large carious and pulpal exposure
The success of the technique depends on vital root pulp
Cotton pellet applied to the pulpal stumps after formocresol pulpotomy should be = Dampened with formocresol and placed for 5 mins
Amount of pulp to be removed in formocresol technique= entire coronal pulp down to the cervical constriction of each root canal
FERRIC SULPHATE = material with haemostatic effect, used as a substitute for formocresol pulpotomy
EFFECT = Surface fixation of pulpal tissue accompanied by degeneration of odontoblasts
The first sign of formocresol technique failure = Internal resorption
Glutaraldehyde Pulpotomy
Superior fixative properties
Conc as pulpotomy agent = 2 to 5 % concentration
The cotton pellet is kept on pulp stumps = for 3-4 mins
KOPEL
Ferric Sulphate Pulpotomy
2 – 5 seconds
15.5% concentration
100% clinical success rate
CaOH Pulpotomy
contraindicated in primary teeth due to internal resorption – odontoclastic reaction
Immediate reaction = Severe inflammatory reaction
The calcified bridge is evident within = 1 month
Increases in thickness – next 12 months
Failure of technique =
Cvek Pulpotomy
Partial technique
Important criteria of success = Root end completion
Pulpectomy
The entire pulpal tissue is removed
Complete Pulpectomy technique for primary molars is developed by = STARKEY
Pulp extirpation in primary teeth is difficult because = Tortuous anatomy and branching of canals
The major problem with this technique = is limited knowledge of pulpal anatomy
KRI paste used for obturation in case of pulpectomy is primarily a mixture of = Iodoform and CMCP
MC filling material, traditionally = Zinc Oxide Eugenol
ROOT CANAL SPREADER = It is not used in the widening of root canals
Pulp Devitalization
PARAFORMALDEHYDE = common medicament in all types of devitalization pulpotomy
Laser = Nd: YAG
Pulp mummification = Indicated in = traumatic exposure of a vital primary tooth
Apexification
Rx of pulpless/nonvital immature young permanent tooth
A condition that leads to apexification = Pulpectomy of the young permanent tooth with incomplete root formation
Any excess CaOH periapically = will be removed by multinucleated giant cells
Increase success rate = Increased blood supply through the wide apex
Best obturated by = OBTURA – thermoplasticizedgutta percha system
FRANK technique
Uses CaOH and CMCP (Camphorated monochlorophenol)
To stimulate root closure/ apexification in incompletely developed young permanent tooth
CMCP = 6 months
Rate of resorption in pulpless primary teeth compared to vital teeth = SIMILAR
In the absence of second premolar roots of primary second molar will most likely = resorb more slowly than normal
Ideal Root Canal filling = CaOH
Rx choice in poor prognosis cases, alveolar abscess and necrotic pulp cases = extraction
Apexogenesis
TRUE STATEMENTS
More of a physiological process
Root development continues
Indicates in pulp tissue with mild inflammation
Done in the vital and infected tooth
In regenerative endo therapy, Metronidazole is replaced by = Ornidazole
Reattachment of fractured tooth fragments using the resin bonding technique is called = Fragment Restoration
STAINLESS STEEL CROWN
Rx of choice for Ankylosis of a primary molar with the absence of a permanent successor
Rx of choice for amelogenesis imperfecta in primary dentition = SSC
A 26-year-old African patient presented with a rapidly growing lesion that expanded the mandible. There was bone destruction on the radiograph and therefore malignancy was suspected. On biopsy, the lesion was intraosseous and was cavitated. There was profuse bleeding and a small biopsy of the lining was taken. The pathologist reported osteoclast-like giant cells and granulation tissue with blood clots.
An aneurysmal bone cyst is a type of benign bone tumor that can occur in the jawbone. It is called an “aneurysmal” because it contains blood-filled spaces that can resemble the sac-like structure of an aneurysm. These cysts are relatively rare, accounting for less than 1% of all bone tumors.
Clinically, an aneurysmal bone cyst can be dramatic because it can grow rapidly and attain a large size. This can cause symptoms such as pain, swelling, and displacement of nearby teeth. When a biopsy is performed to confirm the diagnosis, bleeding can be profuse due to the presence of fragile blood vessels within the cyst. In some cases, a blood transfusion may be necessary to manage the bleeding.
It is important to note that aneurysmal bone cysts often form around an underlying primary lesion, such as a vascular malformation or bone tumor. Therefore, it is crucial to thoroughly evaluate any aneurysmal bone cyst to determine if there is an underlying primary lesion that needs to be addressed. Treatment options for aneurysmal bone cysts may include surgical excision or minimally invasive procedures such as sclerotherapy or curettage.
As a dental student, it is important to be aware of aneurysmal bone cysts as a potential differential diagnosis when evaluating patients with jaw pain, swelling, or other symptoms. If you suspect a patient may have an aneurysmal bone cyst, referring them to an oral and maxillofacial surgeon for further evaluation and management is important.
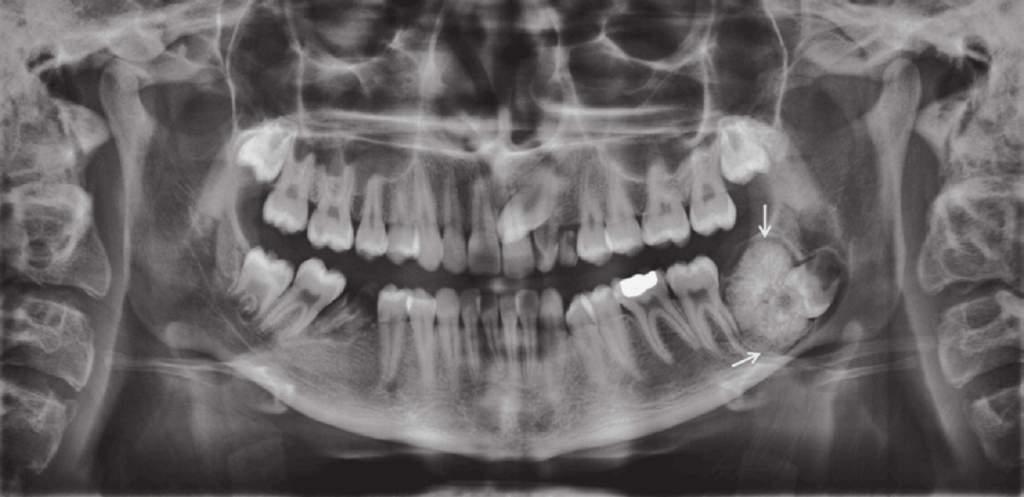
A radiolucent lesion was found incidentally on a dental panoramic radiograph in a 30-year-old man. The cyst was located in the lower molar area above the inferior alveolar canal and showed a scalloped outline extending between the roots of the teeth. All teeth in the area were vital and the lamina dura was intact. Clear straw-coloured fluid was aspirated from the lesion
Solitary bone cyst (SBC), also known as simple bone cyst, is a benign bone lesion that most commonly occurs in children and adolescents. While the exact cause of SBC is still unknown, it is believed to be the result of a disturbance in the normal bone remodeling process.
SBC typically presents as a painless swelling or bump in the affected bone, often discovered incidentally on routine imaging. Diagnosis is usually made by imaging studies such as X-rays or MRI, as well as fine needle aspiration to confirm the presence of fluid within the cyst.
In many cases, SBCs will heal on their own without the need for any intervention. However, if the cyst is causing significant pain or functional impairment, or if it is at risk of fracturing or expanding and causing further damage to the bone, treatment may be necessary.
Treatment options for SBC include observation, which involves monitoring the cyst with regular imaging studies to ensure that it is not growing or causing any problems; curettage, which involves surgically removing the cyst and filling the cavity with bone graft material to promote healing; or injection of bone-stimulating agents such as bone morphogenetic protein (BMP) to promote healing and prevent recurrence.
The decision on whether to intervene or not will depend on various factors, including the size and location of the cyst, the age of the patient, and the presence of any associated symptoms or complications.
A 22-year-old man attended for treatment. He had a history of Gardnerʼs syndrome and noticed a bony hard lump on the ascending ramus of the mandible.
Gardner’s syndrome, also known as familial adenomatous polyposis (FAP), is a rare genetic disorder that affects the colon and rectum. It is caused by mutations in the APC gene and is inherited in an autosomal dominant pattern.
Individuals with Gardner’s syndrome develop numerous polyps in the colon and rectum, which can eventually lead to colorectal cancer if left untreated. Additionally, they may also develop polyps in the stomach and small intestine. The condition is typically diagnosed in the teenage years or early adulthood.
Gardner’s syndrome can also cause abnormalities in the jaw, including multiple osteomas, odontomas, and areas of hazy sclerosis. These dental findings may be one of the earliest signs of the condition and can help with early diagnosis.
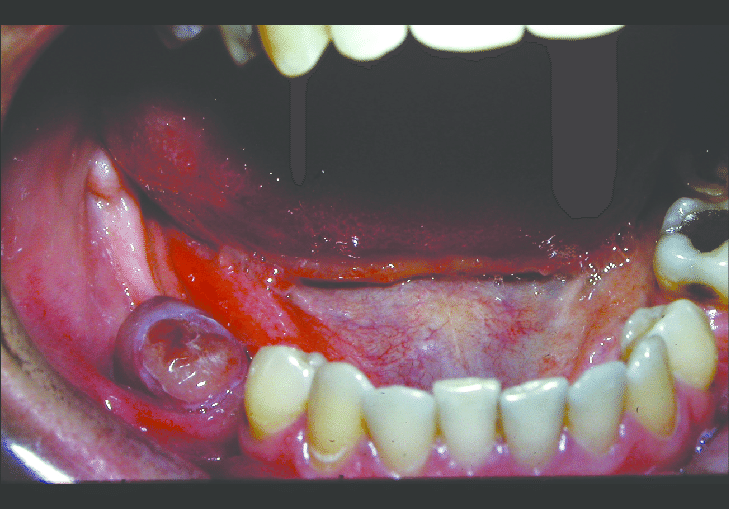
A 58-year-old man presented with a brown–red granular epulis. A periapical radiograph showed underlying bone destruction and a biopsy was reported as showing osteoclast-like giant cells in a spindle-cell background with numerous thin- walled vessels. Haemosiderin and extravasated red cells were abundant.
The clinical and radiographic findings suggest that the 58-year-old man may have a peripheral giant-cell granuloma (PGCG). This is a benign, non-cancerous tumor that often arises from the gum tissue and can cause bone destruction in the underlying jawbone.
The biopsy findings support the diagnosis of PGCG, as the presence of osteoclast-like giant cells and spindle cells in a background of abundant thin-walled vessels is characteristic of this condition. The haemosiderin and extravasated red cells seen in the biopsy are likely a result of bleeding within the lesion, which is common in PGCG.
These same features may also be observed in hyperparathyroidism. However, in hyperparathyroidism, serum calcium levels are typically elevated, while this is not the case in giant-cell granuloma. Therefore, measuring serum calcium levels can be a useful diagnostic tool in differentiating between these two conditions, especially when giant-cell granuloma features are observed.
Treatment for PGCG typically involves surgical removal of the lesion, along with the underlying affected bone. Recurrence is possible, so close follow-up and monitoring is important.