- The widely accepted theory of dental caries is the acidogenic theory
- Miller put forth the acidogenic theory of dental caries in the year = 1890
- The chemo-parasitic theory of dental caries is proposed by = MILLER
- The widely accepted theory of dental caries = Proteolytic chelation theory
- Environmental factors that contribute to dental caries include = nutrition, oral hygiene, fluoride and toothbrush abrasion
- Sucrose = has been determined to be the most cariogenic carbohydrate
- Streptococcus mutans synthesizes levans from = fructose
- Bacteria that adhere to tooth and cause caries is due to = the production of extracellular polysaccharides or dextrans
- The extracellular polysaccharide synthesized by cariogenic streptococci in the presence of excess sucrose is best described as = dextran like glucan**
- Starch is considered to be less cariogenic than monosaccharides and disaccharides because = it does not diffuse through plaque
- Sorbitol acts in the prevention of dental caries by = microorganisms that lack the enzyme to metabolise sorbitol
- Xylitol is a low-calorie sweetener that inhibits the growth of Streptococcus mutans
- On average in the saliva of an adult man, the lactobacilli count is 70000 per ml
- Pathology of dental caries is more closely related to = SUPRA-gingival plaque
- Pathology of periodontal disease is more closely related to = SUB- gingival plaque and Marginal plaque
- Re-mineralisation of the tooth surface is associated with the following component of saliva = Histadine and Statherin
- STEPHAN’s CURVE
- the pH of the plaque = is related to the caries incidence and sugar intake of Stephan’s curve
- Stephan’s curve denotes the relationship between = plaque pH and glucose rinse
- pH at 5.2-5.5 = initiation of caries begins
- TRUE STATEMENTS
- It depends on the amount of calcium and phosphorous in the saliva
- Bicarbonates are the chief buffer of saliva
- At the highest pH, there is a net loss of minerals from the teeth
- pH = 5.5
- The high viscosity of saliva is related to increasing caries in children is partially true
- In a patient with reduced salivary flow, the caries incidence is = more than the patient with normal salivary flow
- In carries free individuals, the saliva has = a high buffering capacity for acids
- The total caries experience in permanent teeth is greater in females than in males of the same age group. The reverse is applied to primary teeth
- Initiation of dental caries depends upon = the localization of acid over the tooth surface
- For a bacterium to be seriously considered in the aetiology of dental caries it must = exist regularly in the dental plaque
- MICROORGANISMS
- Streptococcus mutans
- It is considered to be a principal etiological agent of caries because it produces = organic acids and forms a gelatinous matrix
- S. Sanguis, S.mitor, S.salivarius, S.milleri and Pepto streptococcus** = involved in the initiation of dental caries
- The enzyme glycosyl transferase secreted by S.mutans synthesizes glucans from = SUCROSE
- Lactobacillus acidophilus
- are numerous in caries lesions because they are = secondary invaders and help in the progression of caries, do not initiate smooth surface caries
- It is thought to be one of the etiological agents of dental caries because it is = both acidogenic and acidocuric
- The salivary peroxidase system is known to be effective against = lactobacillus acidophilus
- Organisms involved in deep smooth surface carries = Streptococcus mutans and Lactobacillus acidophilus
- Actinomyces Viscosis and Lactobacillus = Initiates root surface caries***
- Streptococcus mutans
- Smooth surface caries are characterized by the spread of caries in enamel and dentin as CONES, the alignment of the cone is = Apex to base
- SELENIUM = Dental caries is higher in persons residing in seleniferous areas
- Traces of molybdenum and vanadium in the diet may reduce the incidence of caries
- The anti-cariogenic mineral is = vanadium
- In the early stages of the carious lesion.
- Pioneer bacteria are seen in the area of = Dentinal Tubules/Dentin
- Early invading bacteria in carious lesion = Pioneer bacteria
- There is loss of = Interprismatic substance** of enamel with the increased prominence of rods
- Accentuation of incremental lines of retizus is seen
- Clinically the earliest manifestation in an area of a calcification = resembles a smooth chalky white area
- DENTINAL CARIES
- Microscopic zones of dentinal caries starting from DEJ = Bacterial invasion, de-calcification zone and zone of sclerosis
- Miller’s liquefaction foci are present in = Dentinal caries in advanced cases
- The first zone to be found in dentinal caries = Miller’s liquefaction foci
- The clinical significance of sclerotic dentin is that = it is resistant to carries
- Number of dentinal zones = 5
- Turbid dentin in carious tooth
- Zone of bacterial invasion
- Zone which cannot be remineralised
- Zone in which collagen is irreversibly denatured
- Bacteria-free zone of dentinal caries = Zone of dentinal sclerosis
- The lateral spread of caries is facilitated mostly by = dentino-enamel Junction
- Mandibular 1st molar = Tooth in permanent dentition which is more susceptible to dental caries
- Mandibular 2nd Molar = Tooth in primary dentition which is more susceptible to dental caries
- The maxillary arch is more frequently involved by caries than the mandible arch
- Probable reasons for a high incidence of dental caries in the teenage population relate more directly to = the frequency of sucrose intake
- The shape of the cervical form of dental caries = CRESCENT
- The most common surface involved in root carries in the maxillary arch is= the Proximal
- Odontoclasia is = Linear enamel caries
- More number of microorganisms is seen = EARLY MORNING due to the long, overnight incubation period.
- Most pronounced effect on the oral microflora of reduction in the rate of salivary flow = Shift towards in rate of salivary flow
- Ammonia causes = a decrease in plaque formation
- Cavity formation in a tooth, due to dental caries is due to = Lateral spread of caries along DEJ and weakening of the outer covering enamel.
- Animals maintained in germ-free environments did not develop caries even when fed on a high carbohydrate diet given by = Orland and Fitzgerald
- Attachment of actinomyces species to the tooth surface is facilitated by fimbriae
- The type of caries which are not clinically diagnosed but detected only on radiographs = OCCULT caries
- Linear enamel caries lesions in deciduous teeth predominate in = Maxillary anterior teeth
Diagnosis Mystified – Case 8/170
A 1-week-old girl was referred by the paediatrician because of white nodules on her mandibular alveolar ridge.
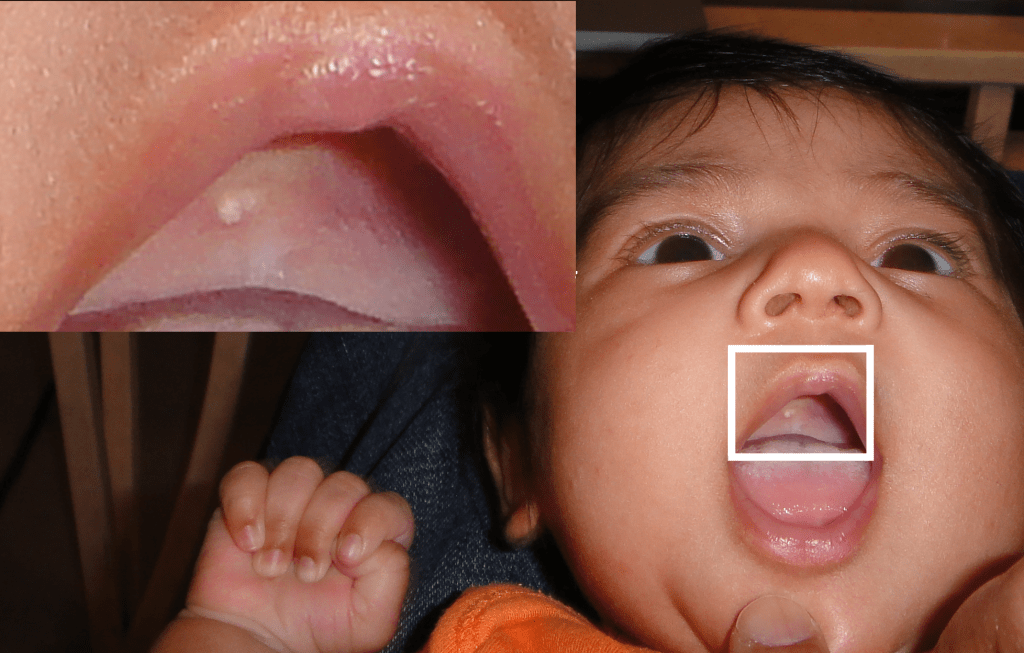
As a dental student, it’s important to learn about various oral conditions that can affect patients of different age groups. Gingival cysts are one such condition that can occur in both neonates (newborns) and adults, although they are more commonly associated with newborns.
In neonates, gingival cysts are often referred to as Epstein’s pearls. These cysts are small, white or yellowish bumps that appear along the gum line or on the roof of the mouth. They are considered a normal finding in newborns and are typically harmless. Epstein’s pearls are thought to result from the accumulation of epithelial cells (the cells that make up the outer layer of the skin) during the development of the gums. They usually resolve on their own within a few weeks or months after birth without requiring any treatment.
On the other hand, gingival cysts can also occur in adults. In adults, these cysts are usually referred to as adult gingival cysts or adult Epstein’s pearls. Adult gingival cysts are similar in appearance to neonatal Epstein’s pearls and can occur anywhere along the gum line. However, unlike neonatal Epstein’s pearls, adult gingival cysts are considered pathological and may require treatment. They are thought to develop due to various factors such as trauma, chronic irritation, infection, or the entrapment of epithelial remnants within the gum tissue.
Diagnosis Demystified – Case 8/255
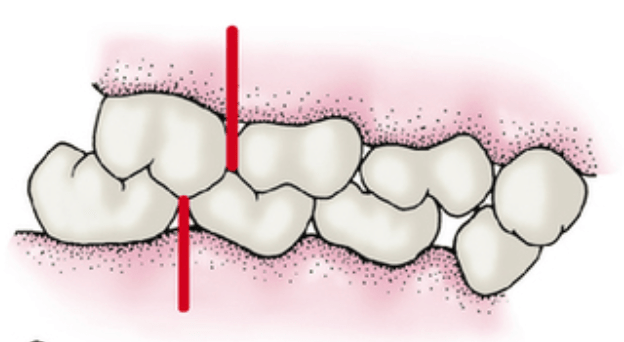
A multilocular radiolucent lesion was found in the interdental bone between the upper first and second premolars. The teeth were vital and after enucleation, the pathologist reported that the cyst had features of a developmental periodontal cyst lined by squamous epithelium with focal thickened areas.

As a dental student, it’s essential to learn about various dental conditions. One specific condition you may come across is called a botryoid cyst or a lateral periodontal cyst.
Botryoid cysts develop from small pieces of tissue called odontogenic epithelial remnants, which are found in the periodontal ligament. These remnants are leftover tissue from tooth development. The term “botryoid” refers to the appearance of these cysts under a microscope, which resembles a cluster of grapes.
Unlike some other cysts caused by inflammation or infection, botryoid cysts are not primarily driven by inflammation. Instead, they are considered a developmental abnormality originating from these remaining epithelial tissues.
When examining a botryoid cyst under a microscope, you may observe focal areas where the cyst lining appears thicker or denser compared to the surrounding epithelium. These areas are known as focally thickened epithelial plaques. The presence of these plaques is a characteristic feature that helps identify botryoid cysts microscopically.
As a dental student, it’s important to keep in mind that this information is based on knowledge available until September 2021. Stay engaged in your studies, seek guidance from your professors, and consult trusted dental resources for the most up-to-date and comprehensive information on dental conditions like botryoid cysts.
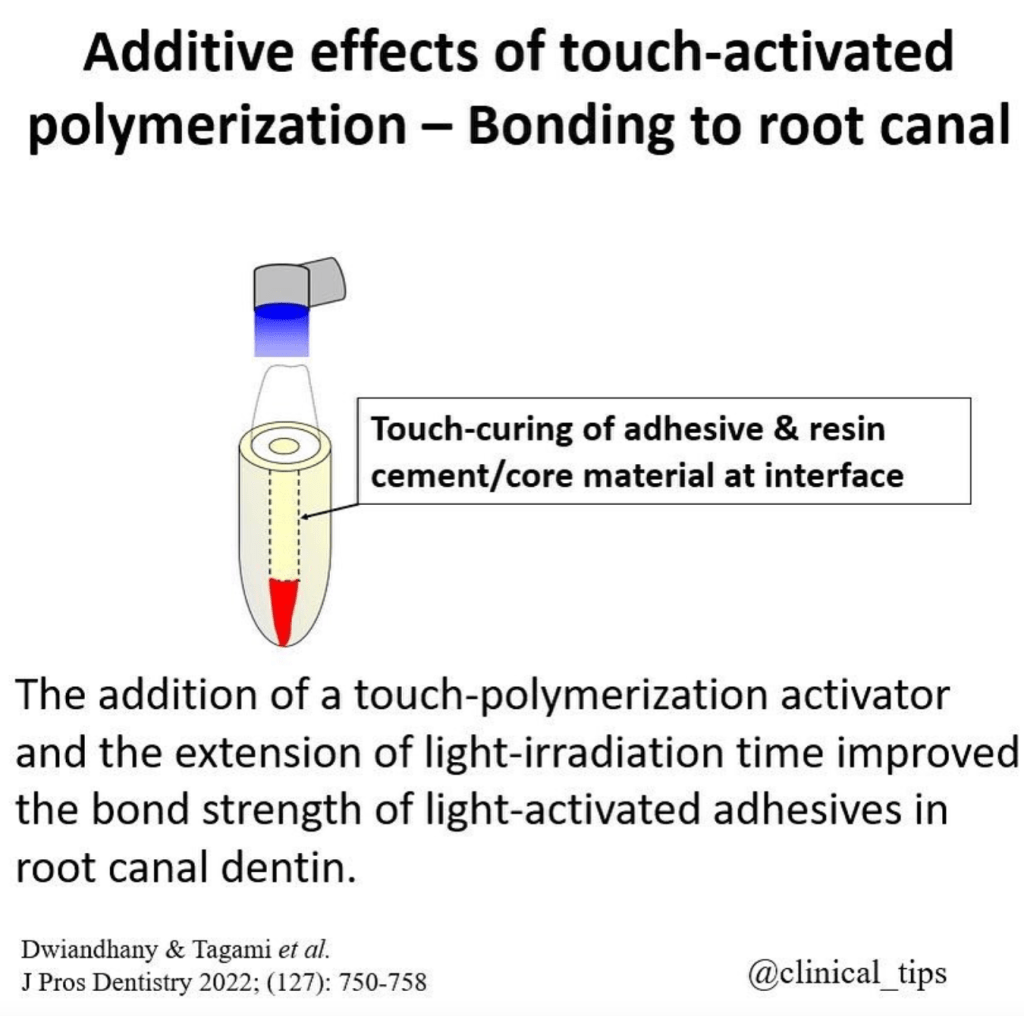
Additive effects of touch activated polymerization – Bonding to root canal
Additive effects of touch activated polymerization have been studied in the context of bonding to root canal dentin. Studies have shown that stresses from polymerization shrinkage and problems with adequate access to the root canal complicate the formation of high-strength bonds when cementing endodontic posts with resin cements [1].
The effects of different bonding systems with various polymerization modes and root canal regions on the bond strength of core build-up resin composite to dentin have also been investigated [2][4].
The interaction of geometrically related factors predicts that bonding of adhesive root-filling materials to root canals is highly unfavorable when compared with indirect intracoronal restorations with a similar resin film thickness [3].
Resin cement polymerization results in shrinkage, creating micro gaps between the fiber-reinforced composite (FRC) posts and the root canal wall [7].
The BS of fiber posts to root canals can be improved by soft-started polymerization [6].
The effect of composite post placement and/or light-irradiation of dual-cure resin composite on adhesion to root canal dentin using the chemical activation mode of a 1-step self-etch dual-cure adhesive has also been evaluated [8].
The activity of matrix metalloproteinases (MMPs) following endodontic irrigation protocols and correlation to the push-out bond strength (PBS) and nanoleakage expression (NL) in the root dentin have been studied [9].
Finally, the mechanical properties of the bonding agent, which could be enhanced by adequate polymerization, have been shown to affect the bond strength to root canal dentin [10].
[1] (2003). Microtensile bond strength between adhesive cements and root canal dentin. Dental Materials, 3(19), 199-205. https://doi.org/10.1016/s0109-5641(02)00030-1
[2] (2021). Effects of different bonding systems with various polymerization modes and root canal region on the bond strength of core build-up resin composite. J Prosthodont Res, 4(65), 521-527. https://doi.org/10.2186/jpr.jpr_d_20_00251
[3] (2005). Geometric Factors Affecting Dentin Bonding in Root Canals: A Theoretical Modeling Approach. Journal of Endodontics, 8(31), 584-589. https://doi.org/10.1097/01.don.0000168891.23486.de
[4] (2021). Effects of different bonding systems with various polymerization modes and root canal region on the bond strength of core build-up resin composite. J Prosthodont Res, 4(65), 521-527. https://doi.org/10.2186/jpr.jpr-d-20-00251
[5] (2020). Novel Bioactive and Therapeutic Root Canal Sealers with Antibacterial and Remineralization Properties. Materials, 5(13), 1096. https://doi.org/10.3390/ma13051096
[6] (2017). Is the bonding of self-adhesive cement sensitive to root region and curing mode?. J. Appl. Oral Sci., 1(25), 2-9. https://doi.org/10.1590/1678-77572015-0430
[7] (2020). The Effects of Differences in Post Canal Widths on Microleakage in Prefabricated Fiber Reinforced Composites. sod, 2(5), 1-8. https://doi.org/10.28932/sod.v5i2.2432
[8] (2010). Effect of composite post placement on bonding to root canal dentin using 1-step self-etch dual-cure adhesive with chemical activation mode. Dent. Mater. J., 6(29), 642-648. https://doi.org/10.4012/dmj.2010-006
[9] (2022). In Situ Zymography Analysis of Matrix Metalloproteinases Activity Following Endodontic Irrigation Protocols and Correlation to Root Dentine Bond Strength. Polymers, 17(14), 3567. https://doi.org/10.3390/polym14173567
[10] (2005). Regional Bond Strength of Four Self-etching Primer/Adhesive Systems to Root Canal Dentin. Dental Materials Journal, 2(24), 261-267. https://doi.org/10.4012/dmj.24.261
Dental Caries Pathology – NEET Pearls from Dentest and Pulse
- The widely accepted theory of dental caries is the acidogenic theory
- Miller put forth the acidogenic theory of dental caries in the year = 1890
- The chemo-parasitic theory of dental caries is proposed by = MILLER
- The widely accepted theory of dental caries = Proteolytic chelation theory
- Environmental factors that contribute to dental caries include = nutrition, oral hygiene, fluoride and toothbrush abrasion
- Sucrose = has been determined to be the most cariogenic carbohydrate
- Streptococcus mutans synthesizes levans from = fructose
- Bacteria that adhere to tooth and cause caries is due to = the production of extracellular polysaccharides or dextrans
- The extracellular polysaccharide synthesized by cariogenic streptococci in the presence of excess sucrose is best described as = dextran like glucan**
- Starch is considered to be less cariogenic than monosaccharides and disaccharides because = it does not diffuse through plaque
- Sorbitol acts in the prevention of dental caries by = microorganisms that lack the enzyme to metabolise sorbitol
- Xylitol is a low-calorie sweetener that inhibits the growth of Streptococcus mutans
- On average in the saliva of an adult man, the lactobacilli count is 70000 per ml
- Pathology of dental caries is more closely related to = SUPRA-gingival plaque
- Pathology of periodontal disease is more closely related to = SUB- gingival plaque and Marginal plaque
- Re-mineralisation of the tooth surface is associated with the following component of saliva = Histadine and Statherin
- STEPHAN’s CURVE
- the pH of the plaque = is related to the caries incidence and sugar intake of Stephan’s curve
- Stephan’s curve denotes the relationship between = plaque pH and glucose rinse
- pH at 5.2-5.5 = initiation of caries begins
- TRUE STATEMENTS
- It depends on the amount of calcium and phosphorous in the saliva
- Bicarbonates are the chief buffer of saliva
- At the highest pH, there is a net loss of minerals from the teeth
- pH = 5.5
- The high viscosity of saliva is related to increasing caries in children is partially true
- In a patient with reduced salivary flow, the caries incidence is = more than the patient with normal salivary flow
- In carries free individuals, the saliva has = a high buffering capacity for acids
- The total caries experience in permanent teeth is greater in females than in males of the same age group. The reverse is applied to primary teeth
- Initiation of dental caries depends upon = the localization of acid over the tooth surface
- For a bacterium to be seriously considered in the aetiology of dental caries it must = exist regularly in the dental plaque
- MICROORGANISMS
- Streptococcus mutans
- It is considered to be a principal etiological agent of caries because it produces = organic acids and forms a gelatinous matrix
- S. Sanguis, S.mitor, S.salivarius, S.milleri and Pepto streptococcus** = involved in the initiation of dental caries
- The enzyme glycosyl transferase secreted by S.mutans synthesizes glucans from = SUCROSE
- Lactobacillus acidophilus
- are numerous in caries lesions because they are = secondary invaders and help in the progression of caries, do not initiate smooth surface caries
- It is thought to be one of the etiological agents of dental caries because it is = both acidogenic and acidocuric
- The salivary peroxidase system is known to be effective against = lactobacillus acidophilus
- Organisms involved in deep smooth surface carries = Streptococcus mutans and Lactobacillus acidophilus
- Actinomyces Viscosis and Lactobacillus = Initiates root surface caries***
- Streptococcus mutans
- Smooth surface caries are characterized by the spread of caries in enamel and dentin as CONES, the alignment of the cone is = Apex to base
- SELENIUM = Dental caries is higher in persons residing in seleniferous areas
- Traces of molybdenum and vanadium in the diet may reduce the incidence of caries
- The anti-cariogenic mineral is = vanadium
- In the early stages of the carious lesion.
- Pioneer bacteria are seen in the area of = Dentinal Tubules/Dentin
- Early invading bacteria in carious lesion = Pioneer bacteria
- There is loss of = Interprismatic substance** of enamel with the increased prominence of rods
- Accentuation of incremental lines of retizus is seen
- Clinically the earliest manifestation in an area of a calcification = resembles a smooth chalky white area
- DENTINAL CARIES
- Microscopic zones of dentinal caries starting from DEJ = Bacterial invasion, de-calcification zone and zone of sclerosis
- Miller’s liquefaction foci are present in = Dentinal caries in advanced cases
- The first zone to be found in dentinal caries = Miller’s liquefaction foci
- The clinical significance of sclerotic dentin is that = it is resistant to carries
- Number of dentinal zones = 5
- Turbid dentin in carious tooth
- Zone of bacterial invasion
- Zone which cannot be remineralised
- Zone in which collagen is irreversibly denatured
- Bacteria-free zone of dentinal caries = Zone of dentinal sclerosis
- The lateral spread of caries is facilitated mostly by = dentino-enamel Junction
- Mandibular 1st molar = Tooth in permanent dentition which is more susceptible to dental caries
- Mandibular 2nd Molar = Tooth in primary dentition which is more susceptible to dental caries
- The maxillary arch is more frequently involved by caries than the mandible arch
- Probable reasons for a high incidence of dental caries in the teenage population relate more directly to = the frequency of sucrose intake
- The shape of the cervical form of dental caries = CRESCENT
- The most common surface involved in root carries in the maxillary arch is= the Proximal
- Odontoclasia is = Linear enamel caries
- More number of microorganisms is seen = EARLY MORNING due to the long, overnight incubation period.
- Most pronounced effect on the oral microflora of reduction in the rate of salivary flow = Shift towards in rate of salivary flow
- Ammonia causes = a decrease in plaque formation
- Cavity formation in a tooth, due to dental caries is due to = Lateral spread of caries along DEJ and weakening of the outer covering enamel.
- Animals maintained in germ-free environments did not develop caries even when fed on a high carbohydrate diet given by = Orland and Fitzgerald
- Attachment of actinomyces species to the tooth surface is facilitated by fimbriae
- The type of caries which are not clinically diagnosed but detected only on radiographs = OCCULT caries
- Linear enamel caries lesions in deciduous teeth predominate in = Maxillary anterior teeth
Diagnosis Demystified – Case 8/255
A cyst was removed along with an unerupted third molar tooth. The pathologist reported a fibrous capsule that was myxoid in places and that was lined by a thin layer of squamous and cuboidal epithelium. The cyst originated from the amelocemental junction.
As a dental student, it’s important to have a good understanding of dentigerous cysts. Dentigerous cysts are a type of cyst that form around unerupted or impacted teeth. They develop from a structure called the dental follicle, which surrounds the tooth germ or the developing tooth.
When a tooth fails to erupt properly, sometimes a cyst can form around it. This cyst is called a dentigerous cyst. It is characterized by a fibrous capsule, which is like a protective layer, and it is lined by stratified squamous epithelium, which is a type of tissue that forms the outer layer of the cyst.
Histologically, dentigerous cysts may show various features such as the thickness of the epithelial lining or the presence of inflammation or keratinization. However, these features are not unique to dentigerous cysts and can also be seen in other types of cysts.
In terms of diagnosis, clinical features are important. Dentigerous cysts are usually discovered during routine dental exams or through radiographic evaluations. One of the key clinical features is that the cyst originates from the amelocemental junction, which is the junction between the enamel (the hard outer layer of the tooth) and the cementum (the specialized tissue covering the root of the tooth).
On an X-ray, the dentigerous cyst appears as a well-defined radiolucent area around the crown of the impacted tooth. It’s important to note that dentigerous cysts often don’t cause any symptoms and are found incidentally. However, if they grow in size or become infected, they can lead to swelling, pain, or displacement of nearby teeth.
Treatment for dentigerous cysts usually involves surgical removal or marsupialization, which is a procedure that creates a surgical opening to allow drainage and shrinkage of the cyst. This is done to prevent complications and facilitate the eruption of the impacted tooth.
Overall, understanding the clinical and histological features of dentigerous cysts is crucial for diagnosing and managing these conditions effectively as a dental student.
Pictorial Puzzles – Pedodontics – Module 2

Veau Classification of Cleft Palate – CLASS 1 – Only soft palate is involved
Distal Molar relationship transforms into Class 2
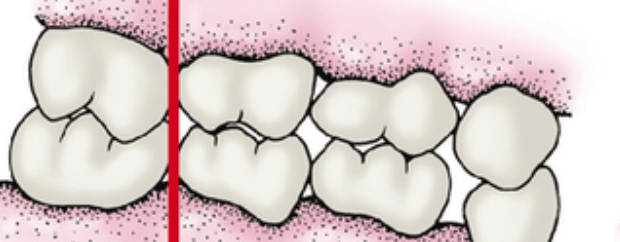
Edge to edge molar relationship transforms into Class 1 or Class 3
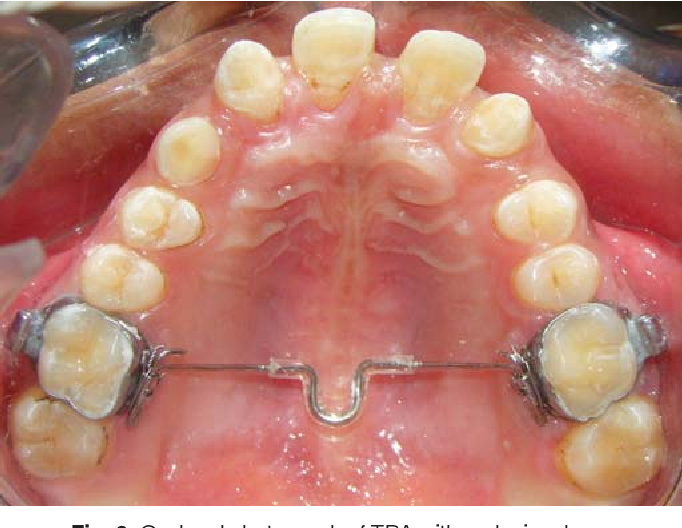
Transpalatal arch = In cases of unilateral loss

Nance Palatal arch = In cases of bilateral loss

Maxillary Anterior bite plane = correction of deep bite

Split labial bow – correction of midline diastema

Crouzon syndrome – Obliteration of saggital sutures, multiple marks in the skull region
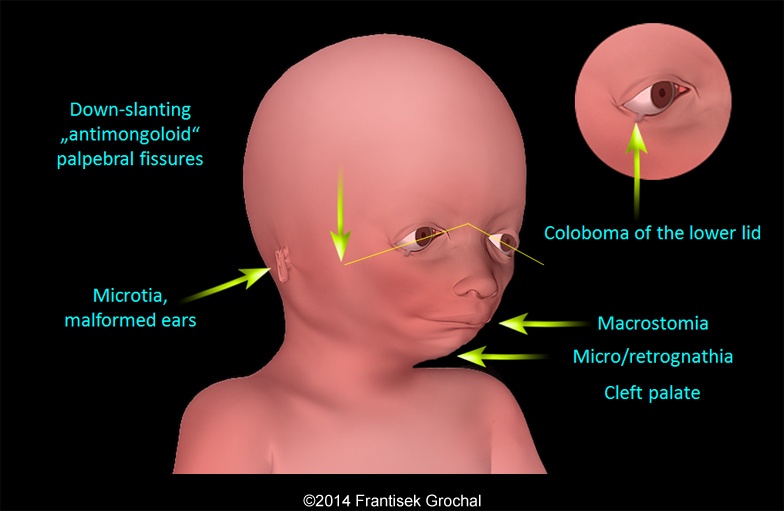
This is Treacher collins syndrome = Autosomal Dominant
Autosomal Recessive – Cystic fibrosis and sickle cell anaemia
X Linked recessive = Hemophilla
X linked dominant = Double cortex syndrome

Red Line = Genital growth
Pictorial Puzzles – Pedodontics – Module 1

Internal Resorption

First permanent molar is about to erupt, so the age = is 5 years

Number of teeth = 19, FUSION
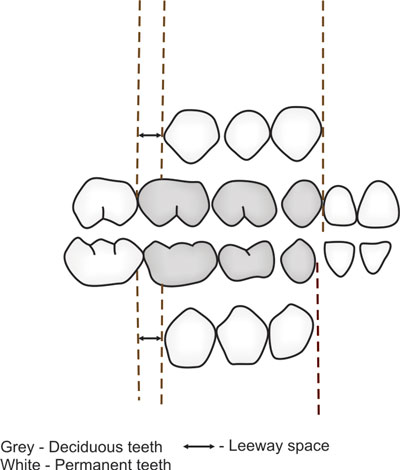
LEEWAY SPACE – Maxillary = 0.9 mm and Mandibular = 1.7 mm

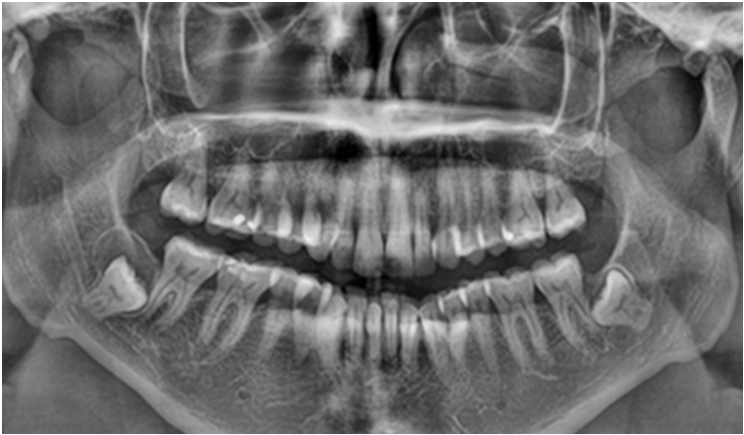
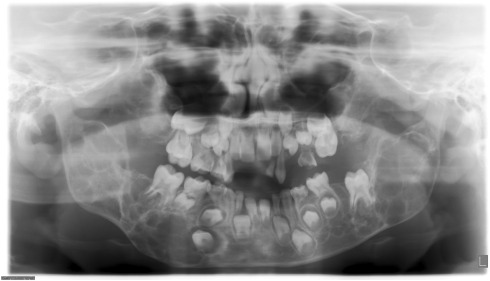
OPG of 10 year old child – permanent CI, LI and first molar has erupted. The primary canine, first molar and second molar are also present.
8 year old male patient comes to your clinic with bilateral swelling in the jaw, upturned eyes with excessive sclera visible beneath the iris = CHERUBISM

AMELOBLASTOMA = Multilocular radiolucency = Honeycomb appearance

FIBROUS DYSPLASIA = mc seen in maxillary bone

Thumb sucking appliance – CRIBS are given

Mouth breathing appliance – ORAL SCREEN
Pictorial Puzzles – Oral Path – #2

Coup de sabre appearance in Sceloroderma
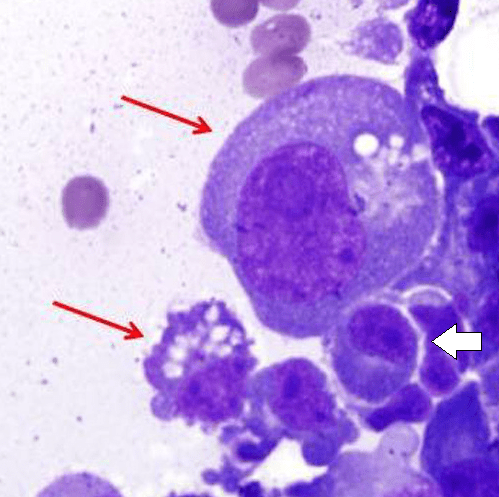
Russell bodies in Multiple Myeloma, In lab findings – Increase in A/G ratio
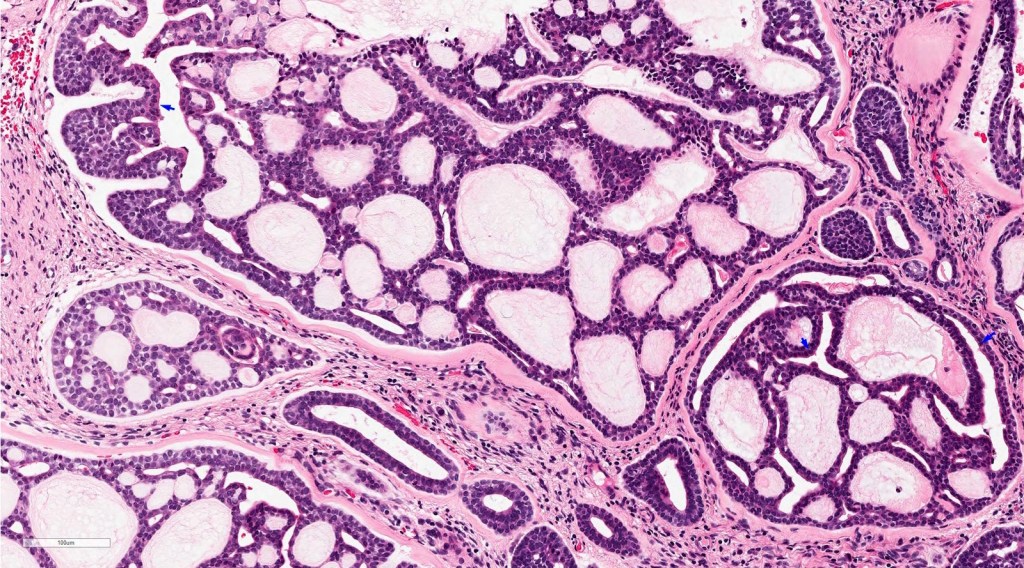
Histological appearance of Adenoid Cystic Carcinoma
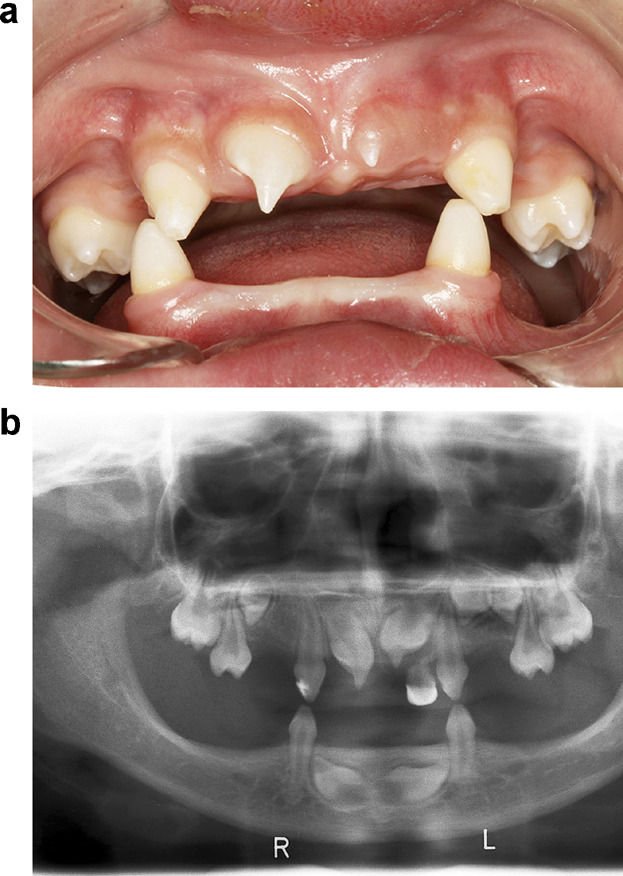
Typical dentition seen in ectodermal dysplasia
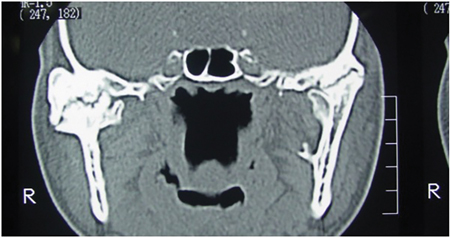
Coronal CT scan showing TMJ ankylosis
Diagnosis Demystified – Case 7/255
A cyst was enucleated from the posterior mandible of a 38-year-old man. The pathologist reported that the lining was composed of stratified squamous epithelium that showed parakeratosis and basal-cell palisading. Some areas were inflamed and cholesterol nodules were noted.

As a dental student, it’s important to understand the histological features of odontogenic keratocyst (OKCs) in order to recognize and diagnose them accurately. Here’s a breakdown of the key features:
- Basal-cell palisading: Odontogenic keratocysts have a specific arrangement of cells in their lining. The cells at the base of the epithelium align in a palisade-like fashion, with their nuclei positioned away from the central cavity of the cyst. This is a distinctive characteristic often seen in OKCs.
- Keratinisation: Odontogenic keratocysts exhibit a high degree of keratinization. This means that the cells within the lining of the cyst produce a protein called keratin, resulting in the formation of a layer of keratinized cells. This keratinization gives the lining a unique appearance when observed under a microscope.
- Uniform thickness: The epithelial lining of an odontogenic keratocyst tends to have a relatively consistent thickness throughout. This means that when examining a tissue sample of an OKC, you will notice that the lining is of similar thickness in different areas. However, it’s important to remember that this feature alone is not sufficient for making a definitive diagnosis.
- Lumen filled with keratinous material: The central space or lumen within an odontogenic keratocyst is typically filled with keratinous material. This material is composed of dead cells that have undergone keratinization. Essentially, the lining of the cyst sheds these keratinized cells, and over time, they accumulate within the cystic space, filling it with this keratin debris.
Remember, these histological features are indicative of an odontogenic keratocyst, but a comprehensive diagnosis also requires consideration of other clinical and radiographic findings. It’s crucial to consult with an experienced oral and maxillofacial pathologist for a definitive diagnosis and to determine the appropriate treatment plan for the patient.
