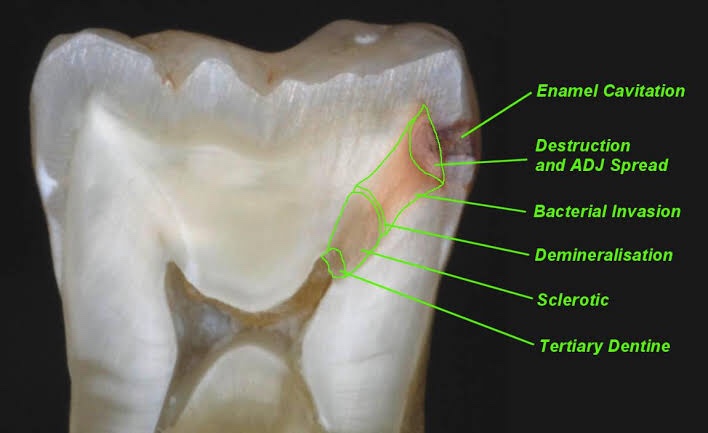
Zone I: Zone of fatty degeneration of odontoblast process Zone 2: Zone of dentinal sclerosis characterized by deposition of cal- cium salts in dentinal tubules Zone 3: Zone of decalcification of dentin, a narrow zone, preceding bacterial invasion Zone 4: Zone of bacterial invasion of decalcified but intact dentin Zone 5: Zone of decomposed dentin
Early dentinal caries
Fatty degeneration of odontob/ast process
>Disposition of fat globules – precedes early sclerotic changes >Special stains – Sudan red >Significance- 1.Fat contributes to impermeability
2.Predisposing factor for dental sclerosis
Sclerotic dentin
>Reaction of vital pulp – calcification of dentinal tubules (DT)
>Seals off DT from further penetration of microorganisms
>Minimal in rapidly advancing caries
>Prominent in slow caries
>Sclerotic dentin – appear white in transmitted light
Decalcification of dentinal tubules
>Above dentinal sclerosis – zone of decalcification
>Occurs in advance of bacterial invasion of DT
>Pioneer bacteria >The initial decalcification – only the walls of DT
>Study of tubules- pure form of microorganisms
Zone of microbial invasion
>Proteolytic organisms – predominantly in deeper layers Acidogenic microorganisms – more in early caries >Supporting the hypothesis that initiation and progression are two distinct processes and must be differentiated
Advanced dentinal caries
>Decalcification of the walls of DT – confluence
>Thickening of sheath of Neumann – along its course • Increase in the diameter of DT – microorganisms
>Focal coalescence of adjacent tubules and ovoid area of destruction- liquefaction foci >Acidogenic organisms – initial decalcification
>Proteolytic organisms – matrix destruction
>Multiple areas of destruction>Necrotic mass of dentin (leathery consistency)
>Formation of transverse cleftsExtend at right angles to DT and parallel contour line
>Peeling away of carious dentin
REFERENCE- Shafers textbook of oral pathology 8th edition
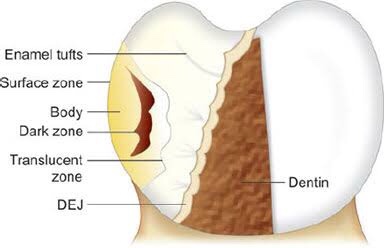
Four zones are clearly distinguishable, starting from the inner advancing front of the lesion. These are the (1) translucent zone, (2) dark zone, (3) body of the lesion and (4) surface layer.
Zones of enamel caries Translucent zone {TZ)
First recognizable zone of alteration
Advancing front of the lesion
Half the lesions demonstrate TZ, not always present
Seen in longitudinal ground sections in clearing (quinoline – RI – 1.62)
TZ appears structureless
Pore volume – I% (compared to 0.1 % of sound enamel)
Dark zone
Lies adjacent and superficial to the translucent zone Positive zone
Shows positive birefringence (in contrast to sound enamel.
Pore volume of 2-4% (polarized light) Presence of small pores; large molecules of quinoline are unable to penetrate Micropore system – gets filled with air and becomes dark Medium like water may penetrate
Body of the lesion
Between unaffected, surface and dark zone Area of greatest demineralization Pore volume – 5% in periphery and 25% in centre Quinoline imbibition – body appears transparent Water imbibition – positive birefringence compared to sound enamel Striae of Retzius – prominent
Surface zone
Quantitative studies – partial demineralization of 1-10% • Pore volume – less than 5% of the spaces
Negative birefringence – water imbibition
Positive birefringence – porous subsurface All the four zones of enamel caries cannot be seen with same immersion medium.
REFERENCE – Shafers textbook of oral pathology 8th edition
The term “juvenile periodontitis” was introduced by Chaput and colleagues in 1967 and by Butler in 1969. In 1971, Baer definedit as “a disease of the periodontium occurring in an otherwise healthy adolescent which is characterized by a rapid loss of alveolar bone about more than one tooth of the permanent dentition.
• Usually affecting persons under 30 years of age (however, may be older).
• Generalized proximal attachment loss affecting at least three teeth other than first molars and incisors.
• Pronounced episodic nature of periodontal destruction. • Poor serum antibody response to infecting agents.
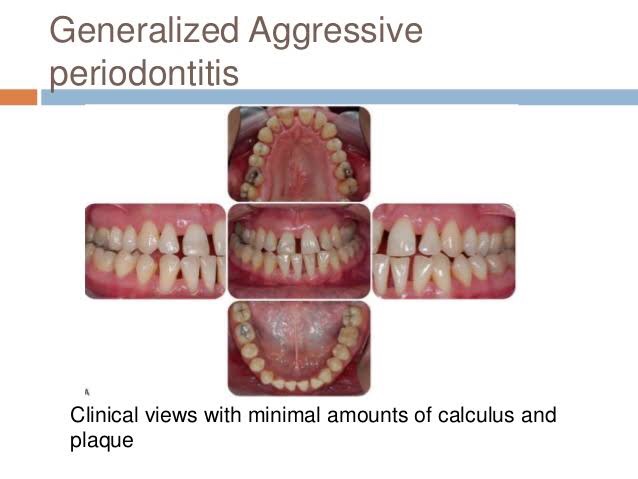
Clinical Characteristics
GAP usually affects individuals under age 30, but older patients also may be affected. In contrast to LAP, evidence suggests that individuals affected with GAP produce a poor antibody response to the pathogens present.
Clinically, GAP is characterized by “gen- eralized interproximal attachment loss affecting at least three per- manent teeth other than first molars and incisors.”The destruction appears to occur episodically, with periods of advanced destruction followed by stages of quiescence of variable length (weeks to months or years).
P. gingivalis, A. actinomycetemcomitans, and Tannerella forsythia (formerly Bacteroides forsythus) frequently are detected in the plaque that is present.
Two gingival tissue responses can be found in cases of GAP. One is a severe, acutely inflamed tissue, often proliferating, ulcerated, and fiery red. One is a severe, acutely inflamed tissue, often proliferating, ulcerated, and fiery red.
Bleeding may occur spontaneously or with slight stimulation. Suppuration may be an important feature. This tissue response is believed to occur in the destructive stage, in which attachment and bone are actively lost.
Some patients with GAP may have systemic manifestations, such as weight loss, mental depression, and general malaise.
Radiographic Findings
No definite pattern of distribution occurs, The radiographic picture in GAP can range from severe bone loss associated with the minimal number of teeth to advanced bone loss affecting the majority of teeth in the dentition.
Prevalence and Distribution by Age and Gender
A US national survey of adolescents ages 14 to 17 reported that 0.13% had GAP. In addition, blacks were at much higher risk than whites for all forms of aggressive periodontitis, and male teenagers were more likely to have GAP than female adolescents.
Treatment of aggressive periodontitis
• Successful treatment of EOP depends on early diagnosis use of antibiotics against the infecting micro organisms and provision of an infection free environment for healing
• EOP both localized and generalized types includes surgery and use of tetracyclines (Lindhe 1982, Christersson and Zambon 1993)
• T/T of GAP – often less predictable – alternative antibiotics directed to specific pathogenic flora require
– Multidisplinary approach combines clinical labroartory evaluation with conventional periodontal therapeutic methods for diagnosis and t/t of GAP
The term “juvenile periodontitis” was introduced by Chaput and colleagues in 1967 and by Butler in 1969. In 1971, Baer defined it as “a disease of the periodontium occurring in an otherwise healthy adolescent which is characterized by a rapid loss of alveolar bone about more than one tooth of the permanent dentition.
According to Hart et al. diagnosis of localized early-onset periodontitis is based on
• attachment loss of > or equal 4 mm on at least two permanent first molars
and incisors (one of which must be a first permanent molar)
Not more than two other permanent teeth, which are not first permanent molars or incisors, should be affected
• Bone loss around primary teeth can be early finding in LAP
Clinical Characteristics
The lack of clinical inflammation despite the presence of deep periodontal pockets and advanced bone loss .
The amount of plaque on the affected teeth is minimal, which seems inconsistent with the amount of periodontal destruction present.The plaque that is present forms a thin biofilm on the teeth and rarely mineralizes to form calculus.
The rate of bone loss is about three to four times faster than in chronic periodontitis.
Other clinical features of LAP may include (1) distolabial migration of the maxillary incisors with concomitant diastema formation, (2) increasing mobility of the maxillary and mandibular incisors and first molars, (3) sensitivity of denuded root surfaces to thermal and tactile stimuli, and (4) deep, dull, radiating pain during mastication, probably caused by irritation of the supporting structures by mobile teeth and impacted food.
Radiographic Findings
Vertical loss of alveolar bone around the first molars and incisors, beginning around puberty in otherwise healthy teenagers, is a classic diagnostic sign of LAP. Radiographic findings may include an “arcshaped loss of alveolar bone extending from the distal surface of the second premolar to the mesial surface of the second molar”
Prevalence and Distribution by Age and Gender
LAP affects both males and females and is seen most frequently in the period between puberty and 20 years of age.
RISK FACTORS FOR AGGRESSIVE PERIODONTITIS
Microbiologic Factors
A. actinomycetemcomitans, Capnocytophagaspp., Eikenella corrodens, Prevotella intermedia, and Campylobacter rectus), A. actinomycetemcomitans has been implicated as the primary pathogen associated with LAP.
Immunologic Factors
Some immune defects have been implicated in the pathogenesis of aggressive periodontitis. The human leukocyte antigens (HLAs), which regulate immune responses, have been evaluated as candidate markers for aggressive periodontitis.
Genetic Factors
Familial pattern of alveolar bone loss and have implicated genetic factors in aggressive periodontitis.
Environmental Factors
The amount and duration of smoking are important variables that can influence the extent of destruction seen in young adults.46 Patients with GAP who smoke have more affected teeth and more loss of clinical attachment than nonsmoking patients with GAP.16 However, smoking may not have the same impact on attachment levels in younger patients with LAP.
Treatment
In ps with LAP,
Aa organisms penetrate into crevicular epithelium T/T with antibiotic alone such as 2 week course of doxycycline reduce Aa organisms
Surgical removal of infected crevicular epithelium and debridement of root surface during surgery while the patient is on a 14 day course of doxycycline hyclate (1gm per day) (Mandell and Sockaransky 1988, Saxen et al 1990).
Microdentex manufacturers the DMDx(Microdentex, FORT MYERS, Florida) test, a DNA test kit for establisting the risk of aggressive periodontits and confirms whether the child has responded favorably to the use of antimicrobial therapy Retesting after 4-6 weeks after the completion of antibiotic therapy determines the pts response to t/t
• Rams and collagues described keyes technique for treating LAP Scaling and root planning of all teeth , with irrigation to probing depth of saturated inorganic salt solutions and 1% chloramine T.((sodium para-toluene sulfonchloramide) In addition recommended administration of systemic tetracycline (18 per day) for 14 days This dose appropriate for pts 12 yrs of age and older
Home T/T Daily application of paste of sodium bicarbonate and 3% hydrogen peroxide and inorganic salt irrigation.
Cigarettes contain nicotine and by smoking regularly and for long hours, your body becomes dependent on it. Giving up smoking can cause nicotine withdrawal symptoms which are :
Restlessness ,impatience
Eating more than usual
Anxiety / tension
Headaches,irritability / anger
Difficulty in concentration + Depression
Loss of energy,dizziness
Sweating
Insomnia
Stomach or bowel problems
Heart palpitations
Tremors
Craving for tobacco
Stop smoking medicines along with nicotine replacement therapy are effective aid to tobacco cessation & can help control these symptoms.
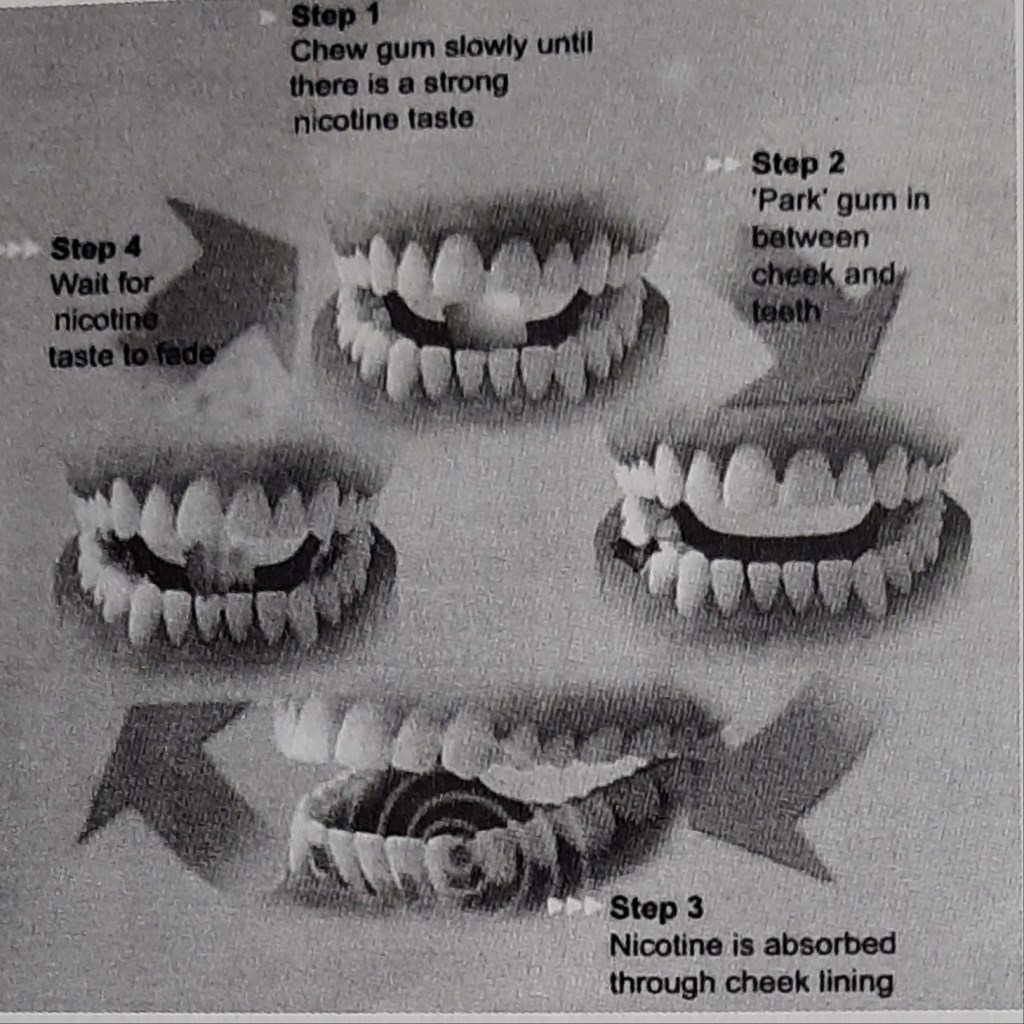
Tobacco intakers who are motivated to quit the habit & are dependent on nicotine should be offered NRT.
Prescribed for 6 to 8 weeks,in blocks of up to 2 weeks,contingent on continued abstinence.
If one type of NRT is not working for the patient ,the health professional is advised to prescribe a suitable type informing about the dosage & maximum amount to take a day.
Is it safe?
NRT is safe because of the facts that the nicotine levels are low and it’s lessaddictive delivery mechanism (unlike smoking tobacco where the nicotine reaches the brain quickly) and also because most of the harmful problems are caused by the other components of tobacco smoke ,not by the nicotine.
NRT is safe for most adults and in people with stable cardiac diseases, but caution needed in unstable,acute cardiovascular disease,pregnancy,or breastfeeding or in those aged under 18 years.
Brownie points-reduces the constant urge to munch on food,thus reducing weight gain.😊
When should one stop using NRT?
Most courses of NRT recommend use for about 12 weeks.This is because it takes this much time for the brain to adjust to working without the high doses of nicotine that the cigarettes supply.However there is no hard and fast rule.After starting the therapy,most people mistake the lack of discomfort for the belief that the addiction is over,leading to stop using the product too soon. This can result only in reappearing of the symptoms.
The best method is to take the help of the health professional when you start the therapy and keep them updated about the progress.
Lastly ,we all are not the same….each tobacco smoker’s tendency & pattern to quit may vary & it depends on different factors like age,gender,environment, general physical and mental health.
Tobacco is the leading preventable cause of death in the world and is the only consumer product that kills when used as intended by its manufacturers ;which may become deadly for non-smokers also.
FACTS & FIGURES:
Tobacco causes 1 in 10 adult deaths worldwide,nearly 5 million deaths a year or one death every 6.5 seconds,killing 50% of regular users.
Total global smoking prevalence is 29%;47.5% men & 10.3% women.
By 2030,70% of deaths in the world is attributable to tobacco.
It’s a known or probable cause of about 25 diseases.
Smokeless tobacco causes oral cancer,especially in lips,tongue,mouth and throat area.
Breathing Environmental Tobacco Smoke(ETS) (i.e .side stream,exhaled smoke from cigarettes,cigars and pipes)causes serious health problems & aggravates allergies and increase the severity of symptoms in children & adolescents, with asthma and heart diseases.
People who start using tobacco early have more difficulty in quitting,are more likely to be heavy smokers and if young people donot begin to use tobacco before the age of 20,they are unlikely to start the habit.
The World Bank estimated that smoking prevention is among the most effective of all health interventions.
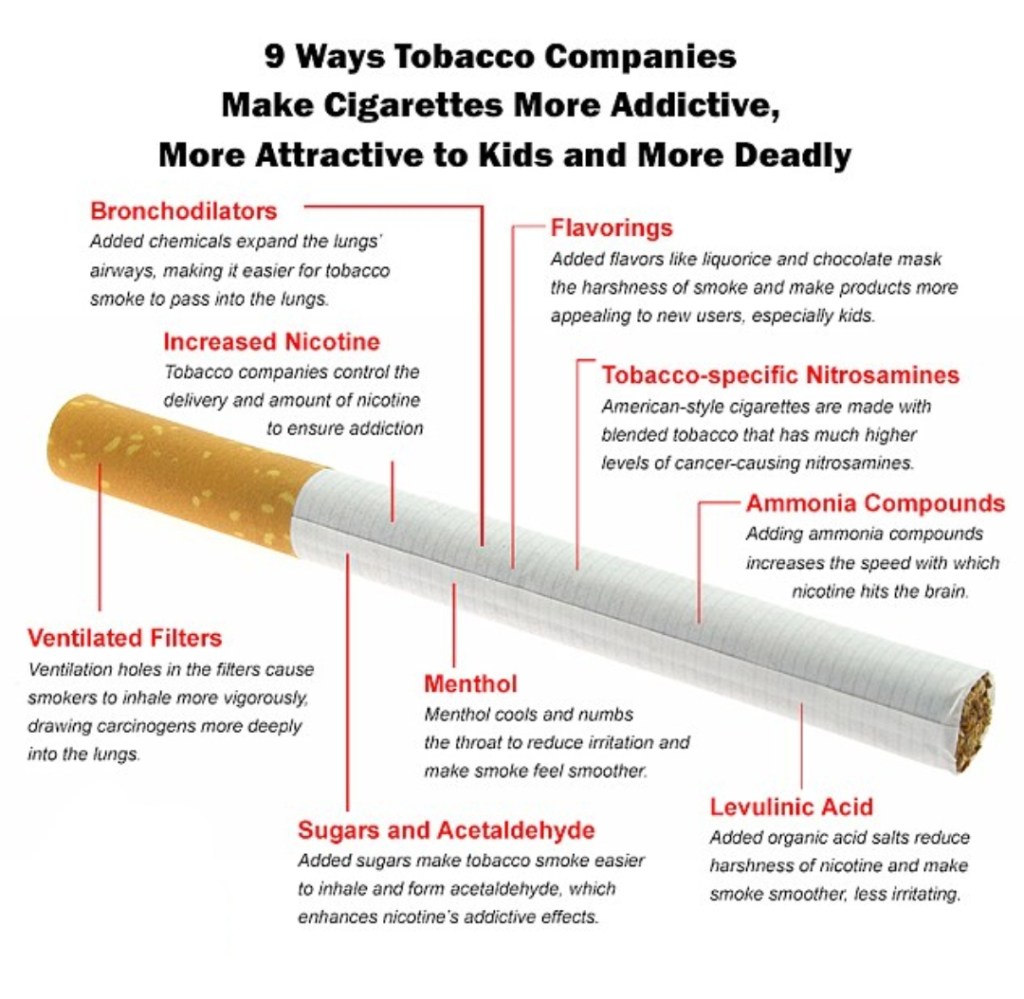
Deadlier than ever-how cigarettes have evolved over last 50 years.
EFFECTS OF NICOTINE :
Electroencephalographic desynchronisation.
Increased circulating levels of catecholamines, vasopressin, growth hormone,adenocorticotropic hormone,cortisol,prolactin,and beta-endorphin.
Increased metabolic rate
Lipolysis,increased free fatty acids.
Heart rate acceleration, nicotine can increase the heart rate by 10-15 beats/min.
Cutaneous & coronary vasoconstriction
Increased cardiac output & blood pressure by 5-10 mm Hg
Skeletal muscle relaxation
Nicotine can induce pathogenic changes to the endothelium associated with atherosclerotic process.
Halitosis,staining of teeth and soft tissues(smokers melanosis),drying of mouth.
‘Nicotine itself is not carcinogenic unless it undergoes nitrosation toform nitrosamines(during tobacco curing & combustion).’
HOW TO ASSESS TOBACCO DEPENDENCE?
A question-answer session with the individual would be very helpful ….
The total score can be calculated to know the dependence.
THE 5 A’S :
ASK-health care professionals / dentists should ask the patient about his or her tobacco intake habits which includes the questions discussed above,during every visit.
ADVICE-health care professional / dentists should continually advice patient to quit the habit thereby emphasizing the importance of the issue.
ASSESS- patients readiness & motivation to quit the habit must be assessed- cause this is a ‘major lifestyle change & requirespreparation, readiness & several failed attempts’.
ASSIST-health care professionals/ dentists should assist those individuals who are motivated- by informing,suggesting and prescribing a pharmacological cessation aids ( nicotine replacement therapy ) and providing or referring the patient to counseling ( individual, group or over telephone ) and behavioral therapies and support services where available.
Lastly,ARRANGE-follow up services are often critical & the dentists can help the patient be tobacco free by providing services like advising availability of national hotlines,support from non-smoking friends or colleagues,or community based support groups.
The best time to quit smoking was the day you started,the second best time is today.
Lastly ,dentists play a major role in helping a patient quit smoking because we might be the first to detect an abnormality( be it a small stain or an abnormal mass ) in the oral cavity during routine examination. Do yourpart ,every small step counts……
Sources- S.S Hiremath textbook of preventive and community dentistry ,www.alhambraesd.org ,www.tobaccofreekids.org