
INTERESTING FACTS ON SMILING!

Here’s a list of the few laboratory tests and investigations which are helpful & specific for diagnosis of certain diseases and conditions.


Sources : Burkets oral medicine 11th edition,Shafer’s textbook of oral pathology 7th edition,www.glasbergen.com
Rubber dam was introduced byBarnum, a New York dentist in 1863
Advantages of using a rubber dam
• It is raincoat for the teeth
• It helps in improving accessibility and visibility of the working area
• It gives a clean and dry aseptic field while working
• It protects the lips, cheeks and tongue by keeping them out of the way
• It helps to avoid unnecessary contamination through infection control
• It protects the patient from inhalation or ingestion of instruments and medicaments
• It helps in keeping teeth saliva free while performing a root canal so that tooth does not get decontaminated by bacteria present in saliva
• It improves the efficiency of the treatment
• It limits bacterial laden splash and splatter of saliva and blood
• It potentially improves the properties of dental material.
• It provides protection of patient and dentist.
Disadvantages of using a rubber dam
• Takes time to apply
• Communication with patient can be difficult
• Incorrect use may damage porcelain crowns/crown margins/ traumatize gingival tissues
• Insecure clamps can be swallowed or aspirated.Contraindications of use of rubber dam
• Asthmatic patients
• Allergy to latex
• Mouth breathers
• Extremely malpositioned tooth • Third molar (in some cases).
Rubber dam equipment
• Rubber dam sheet• Rubber dam clamp • Rubber dam forceps• Rubber dam frameRubber dam accessories•Lubricant/petroleum jelly• Dental floss• Rubber dam napkin.

Rubber Dam Sheet

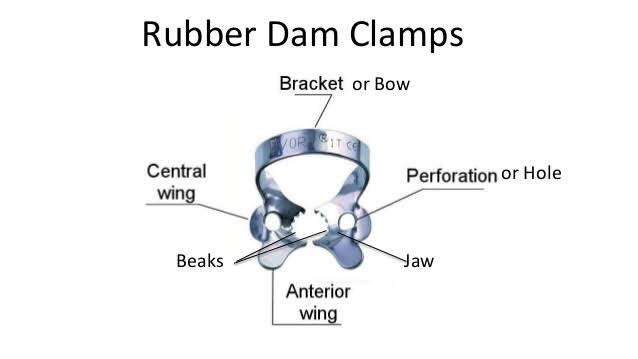
Rubber Dam Clamps
Rubber Dam Forceps

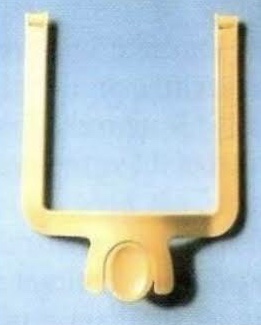
Rubber Dam Frame
Rubber dam frame supports the edges of rubber dam .Frames have been improved dramatically since their old style with the huge ‘butterflies’.Modern frames have sharp pins which easily grip the dam. These are mainly designed with the pins that slope backwards.
• Rubber dam frames are available in either metal or plastic.
• Plastic frames have advantage of being radiolucent.
• When taut, rubber dam sheet exerts too much pull on the rubber dam clamps, causing them to come loose,especially clamps attached to molars.
• To overcome this problem, a new easy-to-use rubber dam frame (Safe-T-Frame) has been developed that offers a secure fit without stretching the rubber dam sheet. Instead, its “snap-shut” design takes advantage of the clamping effect on the sheet, which is caused when its two mated frame members are firmly pressed together. In this way, the sheet is securely attached, but without being stretched. Held in this manner, the dam sheet is under less tension, and hence, exerts less tugging on clamps—especially on those attached to molars.

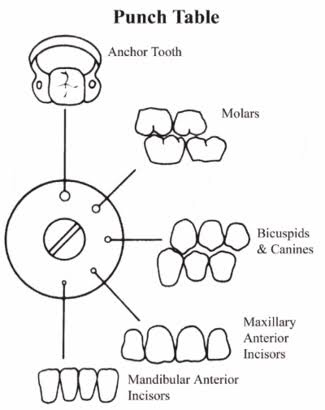
Rubber Dam Punch


Rubber Dam Napkin
• This is a sheet of absorbent materials usually placed between the rubber sheet and soft tissues.
• It is generally not recommended for isolation of single tooth.

REFERENCE – NISHA GARG TEXTBOOK OF ENDODONTICS AND GROSSMAN’S TEXTBOOK OF ENDODONTICS
A continuation of the previous post on syndromes and easy short forms to remember the key features. Hope you find it helpful. Sources: Shafers textbook of oral pathology,www.rxpg.com,instagram–@_dentistars_,@dental_exams,www.medinaz.com

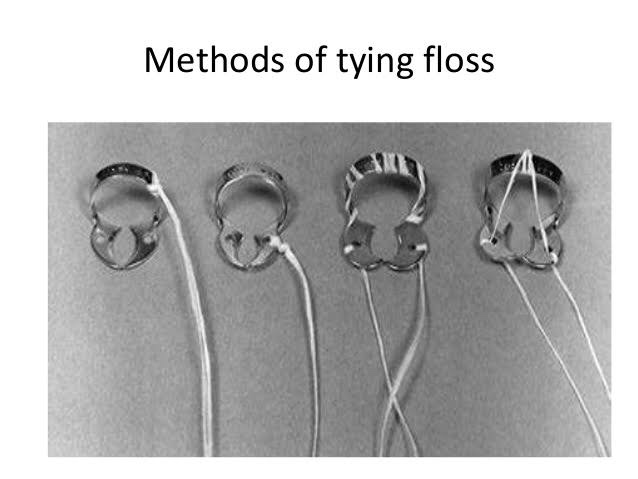
Method II: Placement of rubber dam and clamp together

Split dam technique is indicated:
• To isolate anterior teeth
• When there is insufficient crown structure
• When isolation of teeth with porcelain crown is required. In such cases placement of rubber dam clamp over the crown margins can damage the cervical porcelain.
• Dam is placed without using clamp.
• Here two overlapping holes are punched and dam is stretched over the tooth to be treated and adjacent tooth on each side.
REFERENCE- NISHA GARG TEXTBOOK OF ENDODONTICS

• Occlusal restoration—some suggested that occlusal restoration may lead to weakening of tooth ability to resist the stresses of occlusion leading to abfraction.
• Predisposing factors—factors, such as erosion and abrasion may play a significant role in tooth tissue loss.
Clinical features
REFERENCE- ANIL GHOM TEXTBOOK OF ORAL MEDICINE [2nd ed]
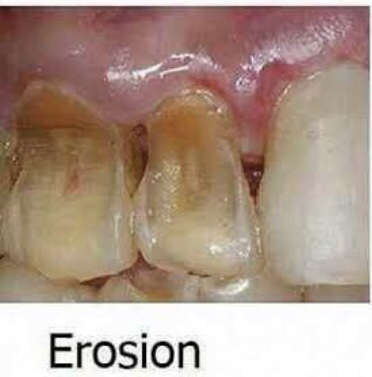
It is the loss of tooth substance by chemical process that does not involve known bacterial action. Dissolution of mineralized tooth structure occurs due to contact with acids. Erosion is a chemical process in which the tooth surface is removed in the absence of plaque.
Types (depending upon etiology)
• Sites—It occurs most frequently on labial and buccal surfaces of teeth; some times, may occur on proximal surfaces of teeth. Usually confined to gingival thirds of labial surface of anterior teeth. Erosion may involve several teeth of dentition. From extrinsic source, it causes erosion on labial and buccal surface and from intrinsic source, it causes erosion on lingual or palatal source.
REFERENCE- ANIL GHOM TEXTBOOK OF ORAL MEDICINE [2nd ed]
Abrasion is the pathological wearing away of tooth substance through some abnormal mechanical process. Abrasion usually occurs on the facial surface of the crown and the exposed root surfaces of teeth, but under certain circumstances it may be seen elsewhere such as on incisal or on proximal surfaces.

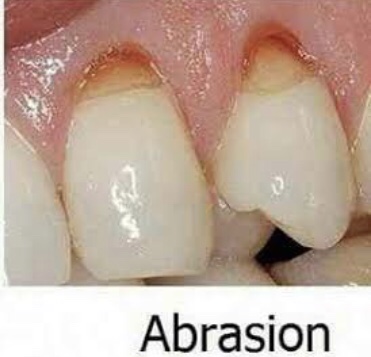
• Mechanism—it occurs due to back and forth movement of brush with heavy pressure causing bristles to assume wedge shaped arrangement between crown and root.
• Appearance—in horizontal brushing there is usually a ‘V’ shaped or ‘wedge’ shaped ditch on the root at cementoenamel junction . It is limited coronally by enamel.
• Symptoms—patient develops sensitivity as dentin becomes exposed.
• Signs—the angle formed in the depth of the lesion as well as that of enamel edge is a sharp one. Cervical lesions caused purely by abrasion have sharply defined margins and a smooth, hard surface. The lesion may become more rounded and shallow, if there is an element of erosion present.
• Dentinal features—exposed dentin appears highly polished Exposure of dentinal tubules and consequent irritation of the odontoblastic processes stimulates secondary dentin formation which is sufficient to protect the pulp from clinical exposure.
Dental floss or tooth pick injury
• Site—Cervical portion of proximal surfaces ,just above the gingival margin, is affected. Grooves on distal surface are deeper than on mesial surface
Radiographic features
Tooth brush injury
• Modified teeth cleaning habits—modification of teeth cleaning habits will be indicated.
• Removal of cause—elimination of causative agent should be carried out.
• Restoration—restoration should be done for esthetics purpose and to prevent further tooth wear.
REFERENCE- ANIL GHOM TEXTBOOK OF ORAL MEDICINE [2nd ed]

Types
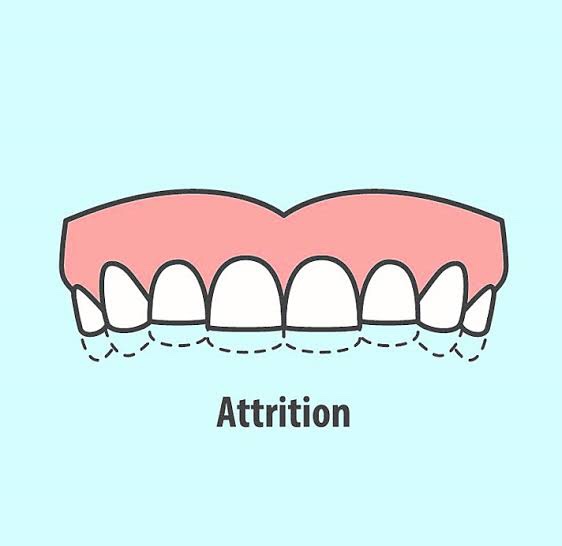
• Physiological attrition—attrition which occurs due to normal aging process, due to mastication.
• Pathological attrition—it occurs due to certain abnor- malities in occlusion, chewing pattern or due to some structural defects in teeth.
Etiological factors for pathological attrition
• Abnormal occlusion
• Developmental—malocclusion and crowning of teeth, may lead to traumatic contact during chewing, which may lead to more tooth wear.
• Acquired—due to extraction of teeth. Extraction causes increased occlusal load on the remaining teeth, as the chewing force for the individual remains constant.
• Premature contact in case of edge-to-edge contact,pathological attrition can also occur.
• Abnormal chewing habits parafunctional chewing habit like bruxism and chronic persistent chewing of coarse and abrasive food or other substances like tobacco.
• Occupation in certain occupations, workers are exposed to an atmosphere of abrasive dust and cannot avoid it getting into mouth.
• Structural defect in defects like amelogenesis imperfecta and dentinogenesis imperfecta, hardness of enamel and dentin is reduced and such teeth become more prone to attrition.
Clinical features
• Sex—men usually exhibit more severe attrition than women due to greater masticatory forces.
• Sites—it may be seen in deciduous as well as permanent dentition. It occurs only on occlusal, incisal and proximal surfaces of teeth. Severe attrition is seldomly seen in primary teeth, as they are not retained for any great period. Palabal cusps of maxillary teeth and buccal cusps of mandibular posterior teeth show most wear.
• Appearance – the first clinical manifestation of attrition is the appearance of small polished facet on a cusp tip or ridge and slight flattening of an incisal edge.
Physiologic attrition
• Pathologicalattrition
Severe tooth loss—in pathological attrition severe tooth loss is seen .
Dentoalveolar compensation—if attrition affecting the occlusal surfaces of teeth has occurred, then reduction in occlusal face height (vertical dimension of occlusion) and increase in the freeway space could be anticipated. This may be further complicated by forward posturing of mandible. It is often observed, however, that despite overall tooth surface loss, the freeway space and the resting facial height appear to remain unaltered primarily because of dentoalveolar compensation. This is important with respect to patient assessment. If restoration of worn teeth is being planned then the extent of dentoalveolar compen- sation would appear to determine the dentist’s strategy; defining the need to carry out measures such as crown lengthening, to ensure the same vertical dimension of occlusion and freeway space.
Radiographic features
• Crown—smoothwearingofincisalandocclusalsurfaces of involved teeth is evident by shortened crown image
• Pulp—sclerosisofpulpchamberandcanalsisseendue to deposition of secondary dentin which narrows the pulp canals.
• Periodontal ligament—widening of periodontal ligament space and hypercementosis.
• Alveolar bone—some loss of alveolar bone.

Management
REFERENCE- ANIL GHOM TEXTBOOK OF ORAL MEDICINE [2nd ed]
Source Gurkeeraat Singh textbook
