
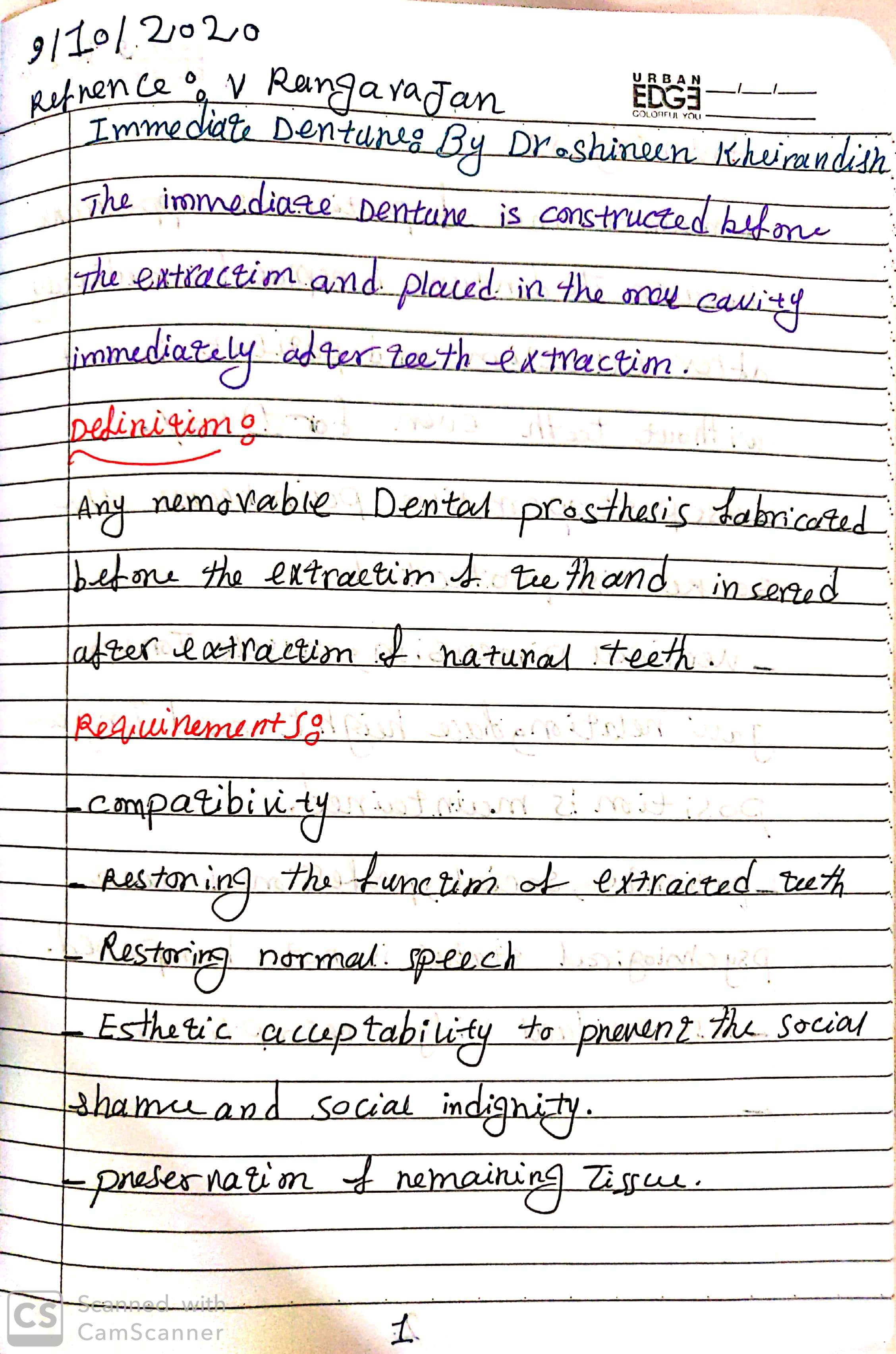
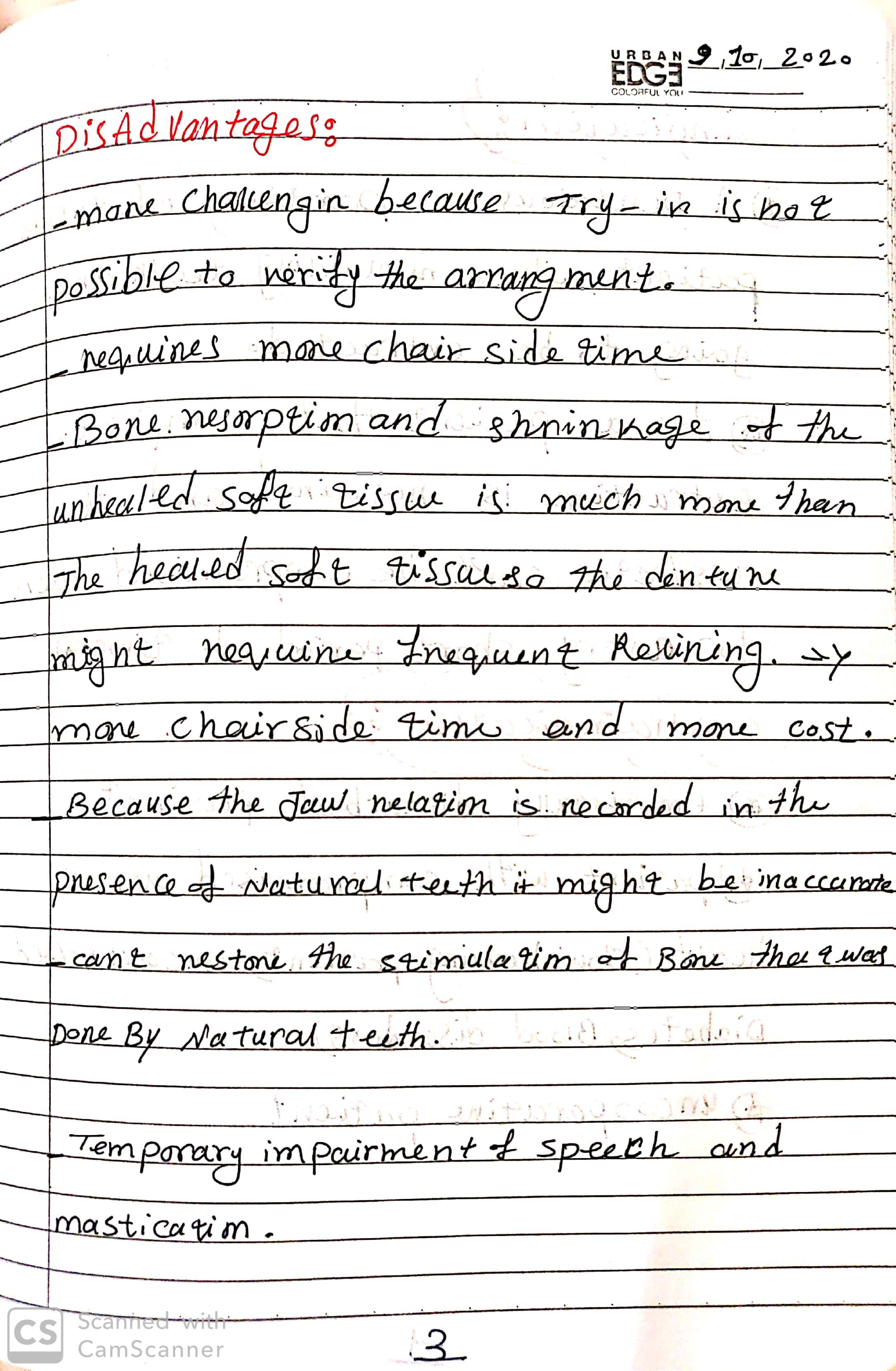
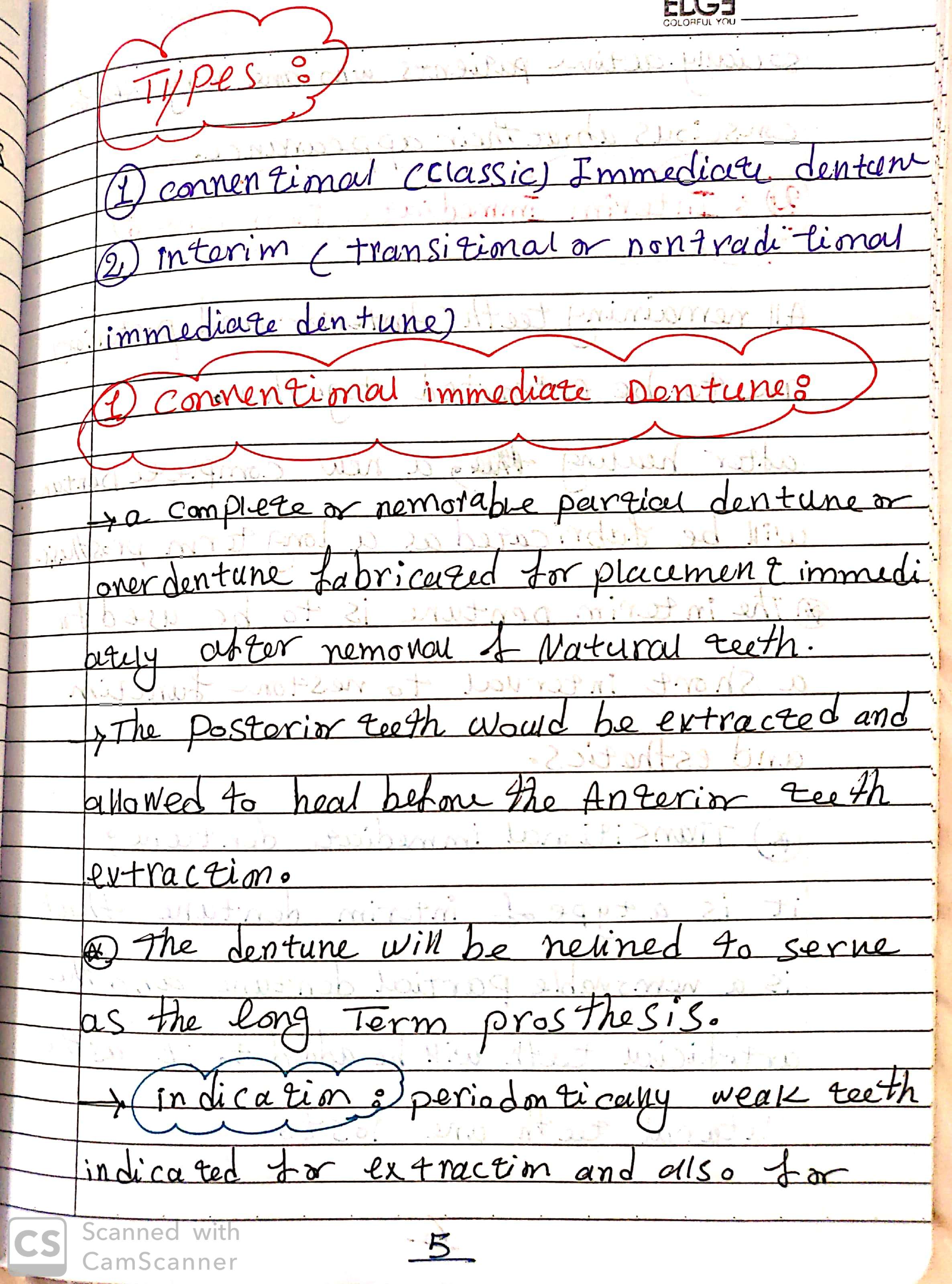
Immediate Dentures





In the NEET MDS Preparation process, the students need to study the previous year exams thoroughly and identify the important topics. This article sheds light on Operative Dentistry & the list of Questions MERITERS experts will answer that are essential for an effective and efficient preparation:
10-13/240 Questions (5%)


Author : V Gopikrishna
INR 1,338 Buy on Amazon

Author : Andre V. Ritter DDS MS
INR 7,595 Buy on Amazon
| Unit | Most Important Topics |
| Cariology | Diagnosis and Treatment planning |
| Operator Positions | |
| Microbiology of Caries | |
| Classification of Caries- GV Black, Root caries, Caries cone | |
| Histo-pathological changes of Enamel and Dentin | |
| Diagnosis of Caries | |
| After Restoration Procedures | |
| Infection control | Occupational Safety and Health ActAerosols and UltrasonicsClassification of Medical, Surgical and Dental InstrumentsSterilization |
| Dental Adhesion | Enamel and dentin bonding systems |
| Direct filling gold | ClassificationManipulationPrinciples of tooth preparation |
| Composites | Composition and classificationCavity preparationPolymerization of composites |
| Amalgam | ClassificationPin retained amalgam restorationsMercury toxicityTrituration |
| Caries and Cavity Preparation | CariologyTooth preparation |
| Sterlization and Isolation | Moist and dry heat sterilization, ETOX gasRubber damMatrices |
| Direct Filling Gold | Types of Direct Filling GoldCavosurface MarginCohesive GoldDegassingCondensation and CompactionProperties of Gold |
| Cast Gold Restorations, Inlays, Onlays | Indications and Contraindications |
| Principles of Tooth Preparations | |
| Finish Lines and Cavosurface Margins | |
| Sprue | |
| Porosities | |
| CAD –CAM | |
| Functional Cusp Bevel | |
| Biomechanical Principles | Cavity Preparation, Smear Layer |
| Rubber Dam in Detail | |
| Separators/ Wedges/ Matrices | |
| Gingival Retraction | |
| Debridement, Polishing Agents | |
| Pulp Protection, Air Abrasion | |
| UltraSonics and Lasers in Cavity Preparation | |
| Walls of Cavity/ Line Angles/ Point Angles | |
| Outline Form, Resistance Form | |
| Retention Form, Bevels | |
| Depth Of Cavity, Ferrules | |
| Instrumentation | Hand Cutting Instruments |
| Instrument Formula | |
| GMT, Angle Former | |
| Hatchets, Angles of Dental Bur | |
| Efficiency of Burs | |
| Carbide/ Diamond/ Stainless Steel Burs | |
| Amalgam Restorations | Indications/ Contraindications of Amalgam Restorations |
| Father of Amalgam | |
| Properties of Amalgam | |
| Creep, Phases of Amalgam | |
| Microleakage, Delayed Expansion | |
| Overhangs, Trituration | |
| Eame’s Technique | |
| Burnishing, Condensation | |
| Mercuric Toxicity | |
| Pin Retained Amalgam Restorations | |
| Types of Pins, Thread Mate System | |
| Bonded Amalgam Restorations | |
| Tooth Colored Restorations | Advantages/Disadvantages |
| Indications/Contraindications | |
| Acid Etching | |
| Skipping Effect | |
| Dentin Conditioner | |
| Primers and Adhesive Resin Generations | |
| Fillers in Composites | |
| C-Factor | |
| Margins and Cavosurface Angles | |
| Shade Determination | |
| BIS-GMA | |
| Compomers | |
| Giomers | |
| Porcelain Restorations | |
| Other topics | Dentin Hypersensitivity |
| Mahler Scale | |
| Box and Tunnel Restorations | |
| Veneers and Laminates | |
| Bonding Agents |
1. Single best answer
2. Image based questions
3. True or false type questions
Please watch the above featured video for more detailed explanation about this article.
We hope this blog will assist you in preparing this subject meticulously for MDS entrance exams.
Prepare judiciously..
SOURCE: MERITERS!!
We have compiled a list of Questions in this article, which MERITERS experts will answer and are very essential for an effective and efficient preparation:


Author : SHILLINGBURG H.T
INR 2,680 Buy on Amazon
Author : Stephen F. Rosenstiel BDS MSD
INR 950 Buy on Amazon
| UNIT NAME | MOST IMPORTANT TOPICS |
| Diagnosis and treatment planning | Diagnostic Casts |
| Indications, Contra Indications | |
| Pontic Designs, Trauma from Occlusion | |
| Mouth Preparation | |
| Cantilever | |
| Retainers and connectors | Components of FPD |
| Indications for Non-Rigid FPD | |
| Partial Veneer Crowns Indications and Contra Indications Porcelain Jacket Crown | |
| Abutments | Ante’s Law |
| Optimum Crown-Root Ratio | |
| Root Surface Area of Each Tooth | |
| Pontics | Types of Pontics and their Important Features |
| Gingival End of Pontic | |
| Pontics Suitable for Anterior Region | |
| Pontics Suitable for Posterior Region | |
| Technical considerations | Forces acting on Abutment Tooth |
| Structural Durability | |
| Retention, Taper | |
| Freedom of Displacement | |
| Reduction, Types of Crowns | |
| Three-Quarter Crowns | |
| Retentive Grooves | |
| Porcelain Jacket Crown | |
| Indications of Laminates | |
| Metal Ceramic Restorations | |
| Types of Finish Lines and their Indications | |
| Pier Abutment | |
| Lost Salt Technique | |
| Maryland Bridge | |
| Rochette Bridge | |
| Virginia Bridge | |
| Miscellaneous | Gingival Retraction |
| Failure of Abutment | |
| Cementation and post- cementation problems | Thickness of Luting Cement |
| Occlusal Disharmony | |
| Occlusal considerations | Variation between Centric Relation and Maximum Intercuspation |
| Canine Protected Occlusion | |
| Bennett Shift | |
| Bennett Movement | |
| Working Side | |
| Non-Working Side | |
| Selective Grinding | |
| Beyron’s Point | |
| Types of Bone Quality | |
| Obturators |
1. Single best answer
2. Image based questions
3. True or false type questions
Please watch the above featured video for more detailed explanation about this article.
We hope this blog will assist you in preparing this subject meticulously for MDS entrance exams.
Prepare judiciously..
SOURCE: MERITERS!!
Muhad Noorman P – Final year -Team Dentowesome
Most often we get frustrated by studying for days before exams, often we fail to recollect or forget while writing exams. It’s a quite natural process for a human body to forget.
However there are tricks to master our hippocampus and remember for long. Excelling in exams are only possible based on how much you remember topics.
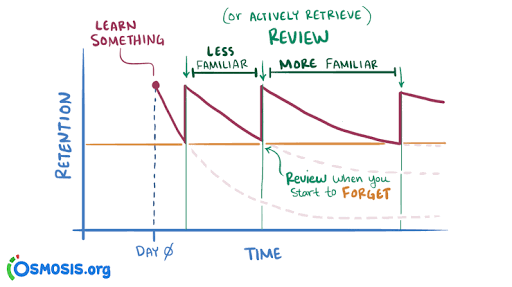
According to Ebbinghaus curve of forgetting information is lost from brain and we’re inable to recollect it.A typical graph of the forgetting curve purports to show that humans tend to halve their memory of newly learned knowledge in a matter of days or weeks unless they consciously review the learned material.

In oder to master long term memorization, we need to practice following methods
Revision : You still remember, A for apple and mitochondria is power house of cell. Constant and frequent revison makes your hippocampus to convert short term memory to long term memory.
Spaced repetition learning technique
Review Your Notes. Within 20-24 hours of the initial intake of information, make sure the information is written down in notes and that you have reviewed them.
Recall the Information for the First Time. Recall the Materials Again.
Study It All Over Again
Difficult topics are checked regularly while easy topics could be reviewed occasionally

Take a break method
Study for 20 minutes take a 5 minute break repeat pattern for 3 to 4 hours. It helps to gain more focus, At the end you’ll be happy for the productive hours. Without break in intervals your brains rejects input eventually your output becomes non productive. Mastering this techinque daily, your graph of productivity hits up.
Use body movements while learning,helps to Tigger muscle memory.
Make a story to memorize long topics. Pieces of information are always connected each other when a story link is given.
Organise your study table. Neat study table and fresh environment boost your intake . Bright light, fresh air, erect spine enhance brain functioning. Feel comfortable stay away from cluttered environment
Try to understand what you learn, things you understand and studied are memorised 9 times.
Learn opposite things .
Switch your topics frequently. Similiar memory get’s intermixed (interference theory).
Things learned at the beginning and end are most memorized. Plan your topics accordingly.
Dicatate your topics and record in dictaphone you can download in your phone. Hear audios before you sleep, going to a beach or restaurant… Brain makes short term memory to long term memory while relaxed.
Visualise your topics. You still remembers the colour of precipitate and titration from your 12th chemistry lab practicals. Visualized memory is far beyond your imaginations.
Read first from books, 2 or 3 days later watch related topics videos from Youtube or any informative apps. Audio+ video learning brushes your previous stored information
Always make use of Sticky notes of alternating colours (prefer light colours- eye rejects dark colour for long time. Use sticky notes apps In your phone screen ( numericals, years etc.could be written in it).
Last days before your exams should be used for rough reading or revison not for studying. Brain rejects things learned in stressed or a state of anxiety .( Your neurotransmitters makes it mess. Respect them 🤣)
Credits : 1) Forgetting curve definition:Wikipedia. Image : Internet. 2) Spaced repetition technique images from Internet and Osmosis.org website . Spaced repetition method content from Google.
Muhad Noorman P, Final year Student – Team Dentowesome

Scoring good and better marks are always priority of any student irrespective of their level and class . Hard work and smart work helps to score good marks.
Some tips to study smart and score more marks
1) Always organise yourself, Never procrastinate. Don’t think about wasted days ,look forward days ahead and make efficient planning.
2) Give importance to every subject equally, start with easy and end in hard nuts.
3) Identify your best time, and place to study. Ignore and never seek how you’re peer group works. Always your peer lies about studies, focus on yourself 🙂
4) Cut your social distraction, even though it sounds like a rocket science, regular practice helps to cut your Distraction. Utilise focus mode in android phones, Install Forest app. It Helps to prioritise your study hours.
5) Teach yourself as if you’re a teacher, trust me you’ll crack a million topics.
6) Teach you’re peer group , it’ll help to recollect and brush up your brain.
7) Regularly shift your studyplace , between a period of 1 hour or 2 hour later, brain and mind always rejects learning from a same environment.
8) Get familiarise with the exam layout, use previous year question, understand nature of questions , prepare accordingly.
9) Always finish with previous questions first and if time allows study other topic left, mentioned in University syllabus.
10) Reading a book not studying : Revise topic after 1 or 2 hour, Prepare notes, put away books . Attempt topic as an exam question. Self realization is best methodology to improve yourself.
11) Never cut too many corners: Often we get devastated listening rumors , predictable questions . And the truth is anything can come.
12) Practice mock exams during free times. Practice always make a man perfect.
13) Organize your answer while writing in exam papers. Never forget, Presentation matters. Include as much as figures, flowcharts, pie diagrams..etc.. Proove examiner you have an edge over topics. Underline important points with seperate ink.
14) Last but not least get an adequate sleep.(Ideally 6 to 7 hours) Give some time for your brain and hippocampus to process your memory.
References: Image : Google
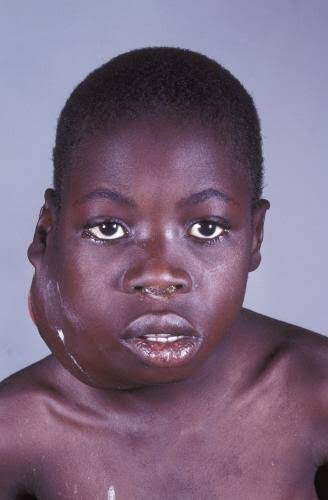
It is also called as ‘African jaw lymphoma’. It is a lymphoreticular cell malignancy. In the African form jaw involvement is 75% and in cases of the American form, abdomen involvement is more common. It is a B-cell neoplasm.
Etiology
• Epstein-Barrvirus(EBV)which also causes nasopharyn- geal carcinoma and infectious mononucleosis is considered to be the etiological factor. There are higher EBV antibody levels in patients of Burkitt’s lymphoma.
Clinical Features
Oral Manifestations
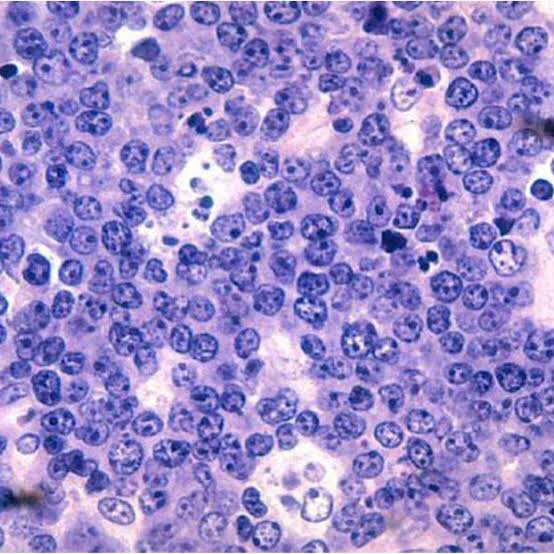
Histology
Shows characteristic starry sky appearance.

• Radiological diagnosis—moth eaten appearance is seen with loss of lamina dura around the teeth.
• Laboratorydiagnosis—monotonous sea of un differentiated monomorphic lymphoreticular cells, usually showing abundant mitotic activity. There is also hyperchro- matosis and loss of cohesiveness. Characteristic ‘starry sky’ appearance is seen.
Management
• Cytotoxicdrugs—cytotoxicdrugs like cyclophosphamide 40 mg/kg in single IV administration and repeated about 2 weeks later. Vincristine and methotrexate have been successful in some cases.
• Multiagent chemotherapy—combination of drugs such as cyclophosphamide, vincristine and methotrexate give better results than any single drug. Majority of patients show dramatic response to the therapy. The swelling regresses and the displaced teeth return to their normal position within 1 to 2 weeks.
REFERENCE- SHAFER’S TEXTBOOK OF ORAL PATHOLOGY AND ANIL GHOM TEXTBOOK OF ORAL MEDICINE
Intrinsic Stains
Pre-eruptive Causes
These are incorporated into the deeper layers of enamel and dentin during odontogenesis and alter the development and appearance of the enamel and dentin
.Alkaptonuria: Dark brown pigmentation of primary teeth is commonly seen in alkaptonuria. It is an autosomal recessive disorder resulting into complete oxidation of tyrosine and phenylalanine causing increased level of homogentisic acid.
Hematological disorders
• Erythroblastosis fetalis: It is a blood disorder of neonates due to Rh incompatibility. In this, stain does not involve teeth or portions of teeth developing after cessation of hemolysis shortly after birth. Stain is usually green, brown or bluish in color.

• Congenital porphyria: It is an inborn error of por- phyrin metabolism, characterized by overproduction of uroporphyrin. Deciduous and permanent teeth may show a red or brownish discoloration. Under ultraviolet light, teeth show red fluorescence.

• Sickle cell anemia: It is inherited blood dyscrasia characterized by increased hemolysis of red blood cells. In sickle cell anemia infrequently the stains of the teeth are similar to those of erythroblastosis fetalis, but discoloration is more severe, involves both dentitions and does not resolve with time.
Amelogenesis imperfecta: It comprises of a group of conditions, that demonstrate developmental alteration in the structure of the enamel in the absence of a systemic disorders. Amelogenesis imperfecta (AI) has been classified mainly into hypoplastic, hypocalcified and hypomaturation type.

Fluorosis: In fluorosis, staining is due to excessive fluoride uptake during development of enamel. Excess fluoride induces a metabolic change in ameloblast and the resultant enamel has a defective matrix and an irregular, hypomineralized structure



Posteruptive Causes

– Dentin deposition: Secondary and tertiary dentin deposits, pulp stones cause changes in the color of teeth.
• Functional and parafunctional changes: Tooth wear may give a darker appearance to the teeth because of loss of tooth surface and exposure of dentin which is yellower and is susceptible to color changes by absorption of oral fluids and deposition of reparative dentin.
Extrinsic Stains
Daily Acquired Stains
Plaque: Pellicle and plaque on tooth surface gives rise to yellowish appearance of teeth.
Food and beverages: Tea, coffee, red wine, curry and colas if taken in excess cause discoloration.
Tobacco use results in brown to black appearance of teeth.
Poor oral hygiene manifests as:
Swimmer’s calculus:
– It is yellow to dark brown stain present on facial andlingual surfaces of anterior teeth. It occurs due toprolonged exposure to pool water.
Gingival hemorrhage.
Chemicals
• Chlorhexidine stain: The stains produced by use of chlorhexidine are yellowish brown to brownish in nature.
Metallic stains: These are caused by metals and metallic salts introduced into oral cavity in metal containing dust inhaled by industry workers or through orally administered drugs.

Stains caused by different metals
• Copper dust—green stain
• Iron dust—brown stain
• Mercury—greenish black stain • Nickel—green stain
• Silver—black stain.
Reference- Nisha garg textbook of endosontics and Anil Ghom textbook of oral medicine
Image Characteristics
CONTRAST RESOLUTION

Film based IOPA – 20 lp / mm.
Digital receptors 7 lp / mm.
Film > CCD > PSP
Detector Latitude
It is the ability of the image receptor to capture a range of x-ray exposures as different densities.
Photostimulable phosphor receptors have larger latitudes and have a linear response to five orders of magnitude of x-ray exposure.

Detector Sensitivity
REFERENCE-WHITE AND PHAROAH 5TH EDITION
Diagnosis
• Clinical diagnosis—skin lesion with lesion present on oral mucosa which is atrophic and erythematous will suspect lupus erythematous. Oral and nasopharyngeal ulceration is major diagnostic criteria for SLE.
Laboratory diagnosis—L.E. cell inclusion phenomenon with surrounding pale nuclear mass apparently devoid of lymphocytes. Anemia, leukopenia and thrombocyto- penia, with sedimentation rate increased. Serum gamma globulin increased and Coomb’s test is positive.
Positive lupus band test—it shows deposition of IgG,IgM or complement component in skin.
REFERENCE- ANIL GHOM TEXTBOOK OF ORAL MEDICINE; BURKIT TEXTBOOK OF ORAL MEDICINE AND GOOGLE[SLIDE SHARE]




