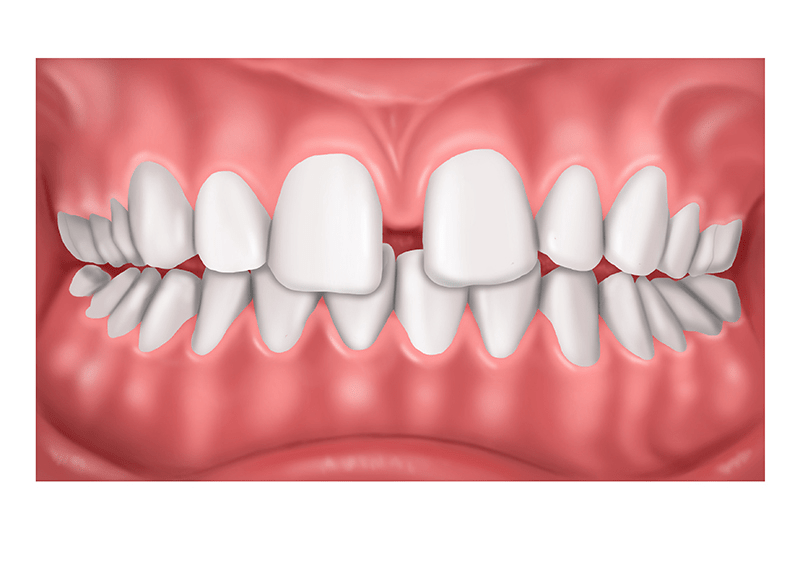
- Causes
- Mesiodens
- High frenal attachment
- Tooth are procline
- Tooth material arch length discrepancy
- Midline pathology
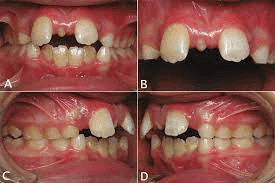

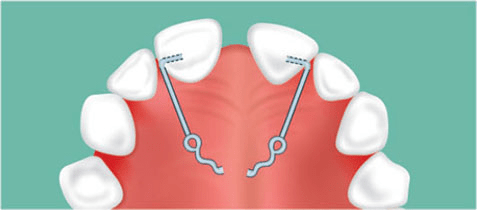
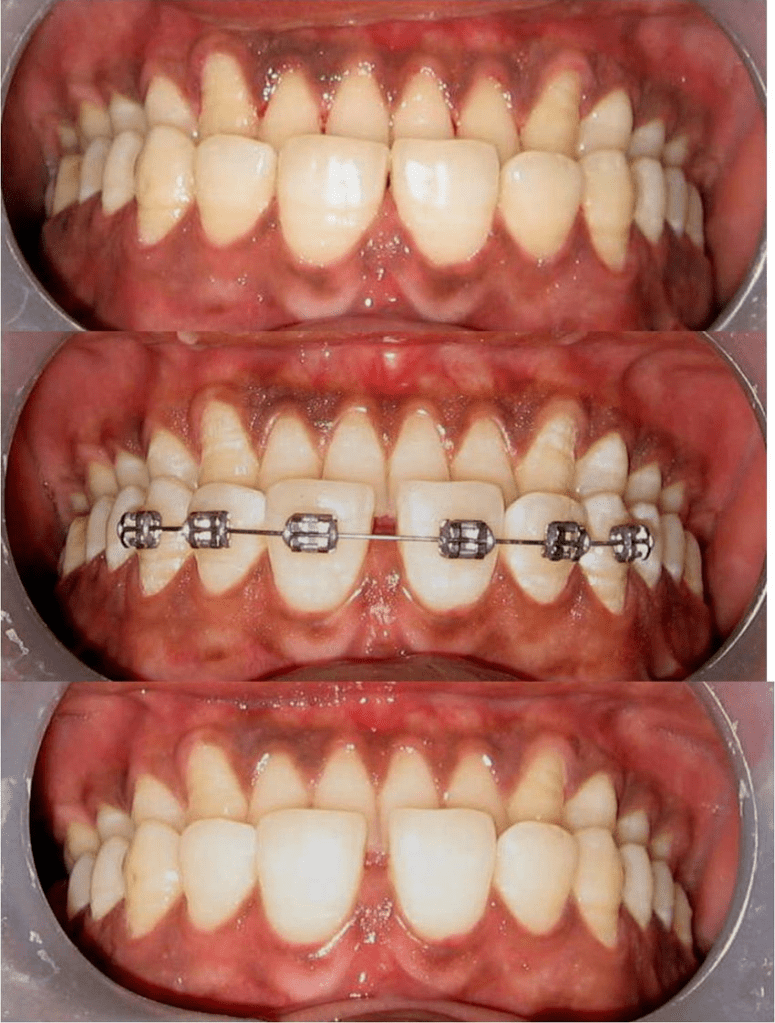
- How to correct midline diastema?
- Composite restoration
- Finger springs = draw
- Fixed appliance = keychain
- Permanent retention
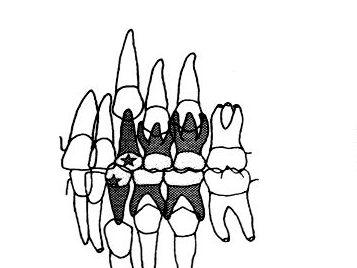
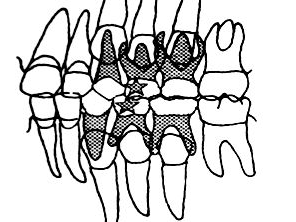
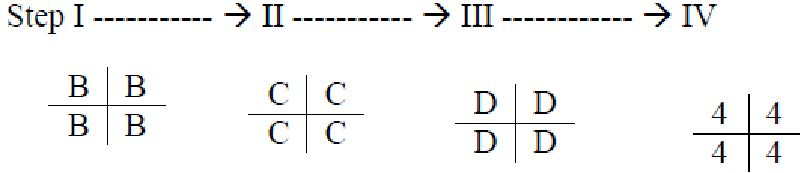
Defined as correctly timed, planned removal of certain deciduous and permanent teeth in mixed dentition cases with dentoalveolar disproportion



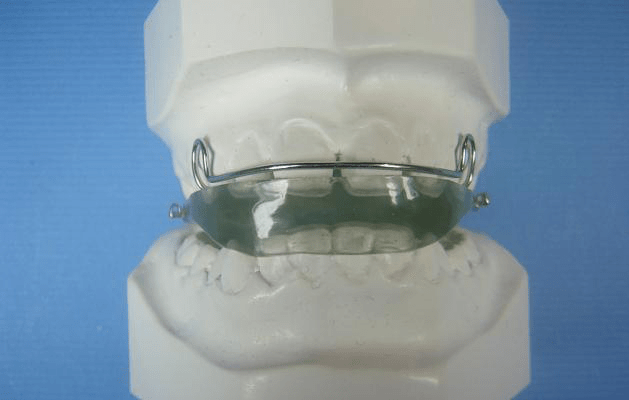
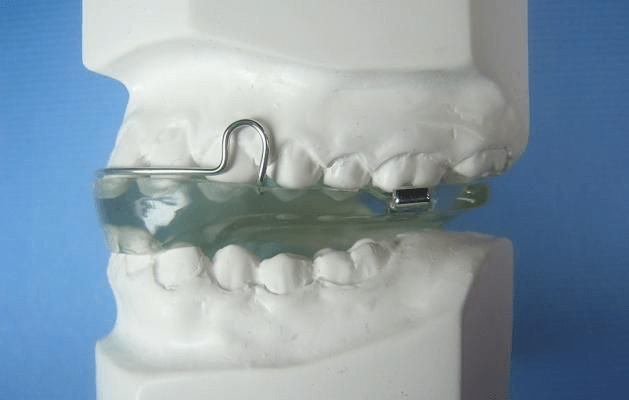
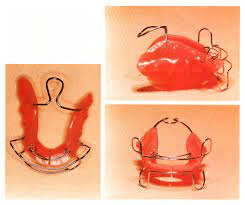
DEFINITION = Functional appliances are defined as ‘loose fitting or passive appliances which harness the natural forces of the orofacial musculature that are transmitted to the teeth and alveolar bone through the medium of appliance’.
ACTIVATOR 4m**
Mechanism of action 2m
Indications 2m

Contraindications
Advantage
Disadvantage = pt compliance
TYPES of activator
FABRICATION STEPS
MODIFICATIONS
BOW ACTIVATOR




References-ortho bhalajhi

References- Bhalajhi orthodontics



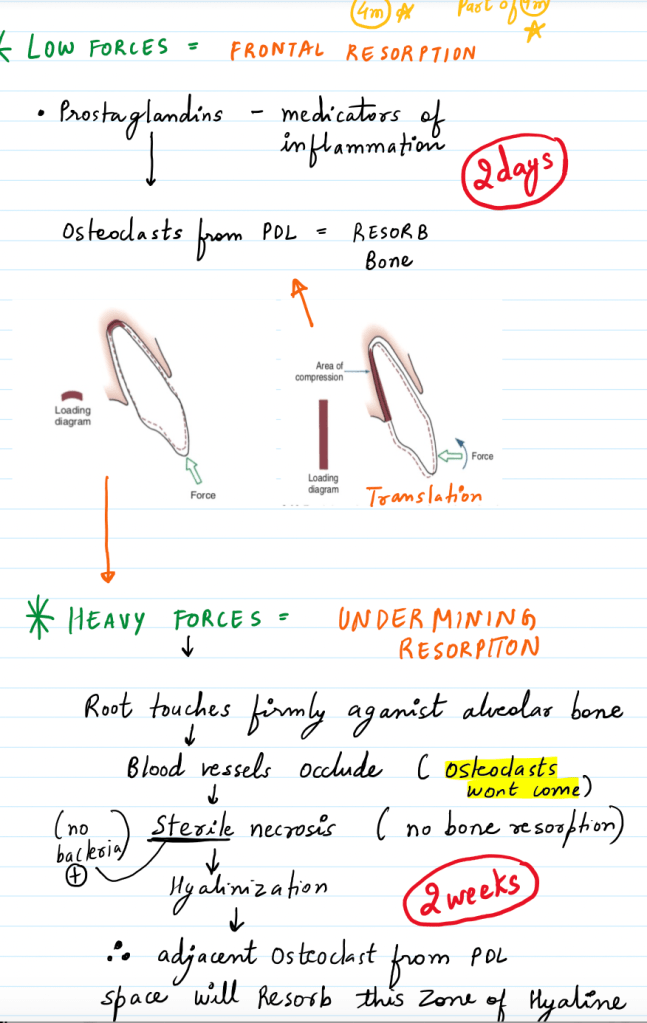
Continuous force- active force that decreases little in magnitude betwwen appointments.
Intermittent force- active force that decays to zero before next appointment.
Interrupted force- inactive for intervals of time between appointments

Reference- orthodontics bhalajhi
Can be categorized into 3 categories-
1. Tipping- single force applied results into movement of crown in direction of force and movement of root in opposite direction.
A) Controlled tipping- When tooth tips about centre of rotation at apex. Lingual movement of crown with minimal movement of root in opposite direction.
B) Uncontrolled Tipping- when movement of tooth occurs about centre of rotation close to centre of resistance. Crown moves in lingual direction and root in opposite direction.
2.Torquing – reverse tipping characterized by lingual movement of root.
3. Bodily movement- All points on tooth will move equal distance in the direction of applied force. Line of action of force is through centre of resistance.
3. Intrusion- bodily displacement of tooth in apical direction along longitudinal axis of tooth.
4. Extrusion- bodily displacement of tooth in coronal direction along longitudinal axis of tooth.
5. Rotational- labial or lingual movement of tooth around long axis
6. Uprighting- when crowns are tipped in mesiodistal direction roots tipped in opposite direction. Tipping the roots back to get parallel orientation is called uprighting.
Reference- ortho bhalajhi
