Clasps are the retentive components of the removable appliances.

Mode of action-
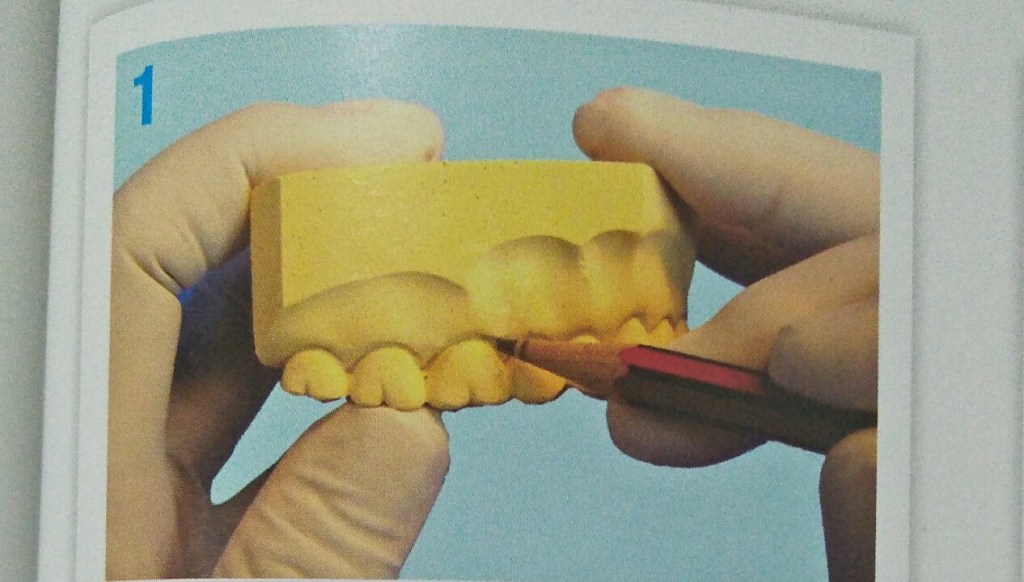
- Clasps act by engaging certain areas of teeth called the undercuts.
- Two types of undercuts are found in natural dentition
- Buccal and lingual cervical
- Mesial and distal proximal
- Adams clasp engages the mesial and distal proximal undercuts.
Adams clasp also called as universal clasp, liverpool clasp and modified arrowhead clasp.
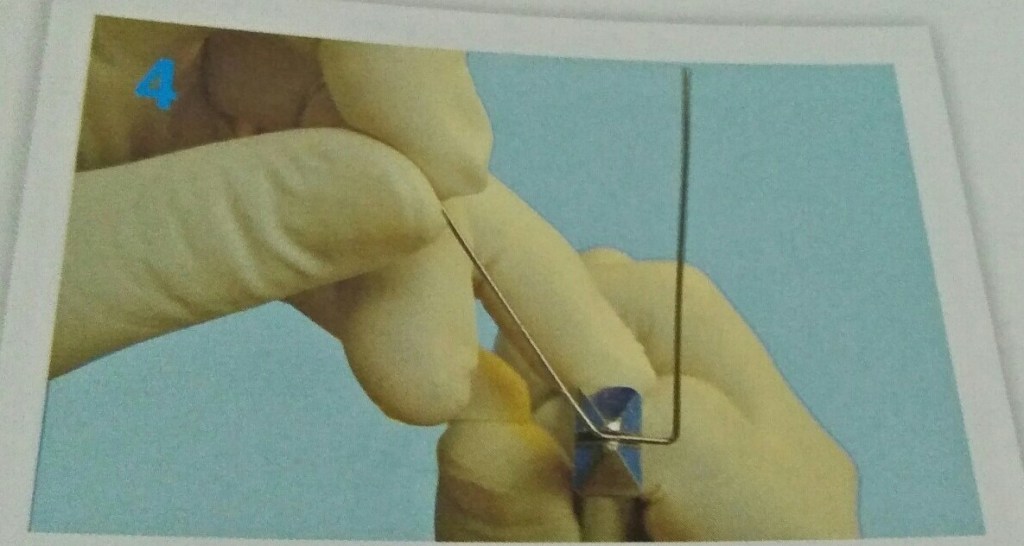
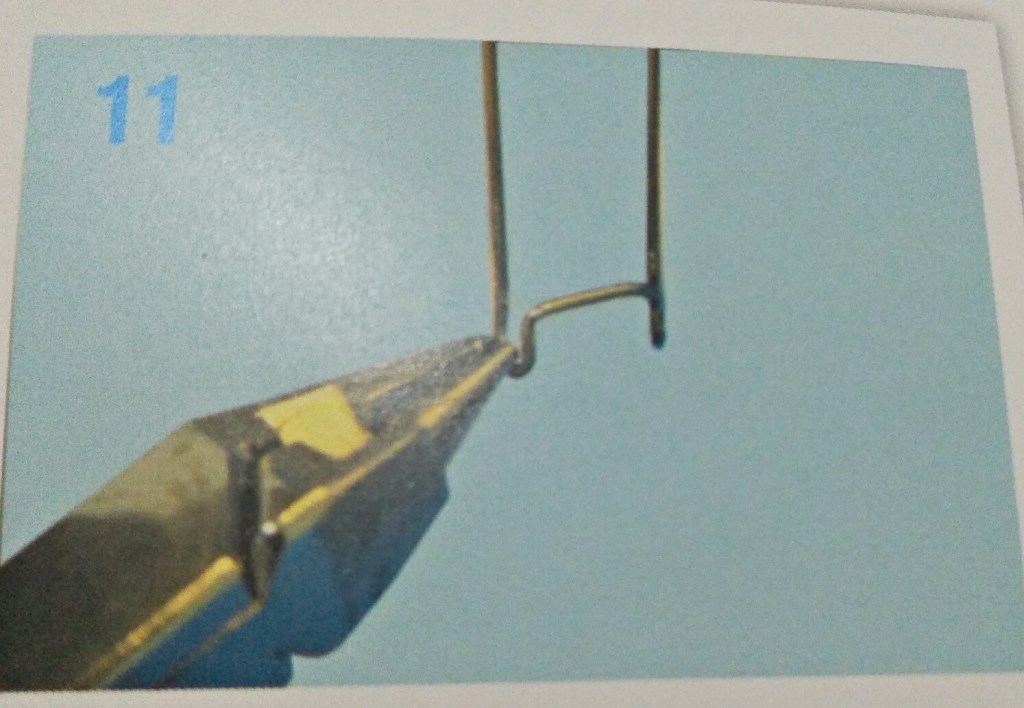
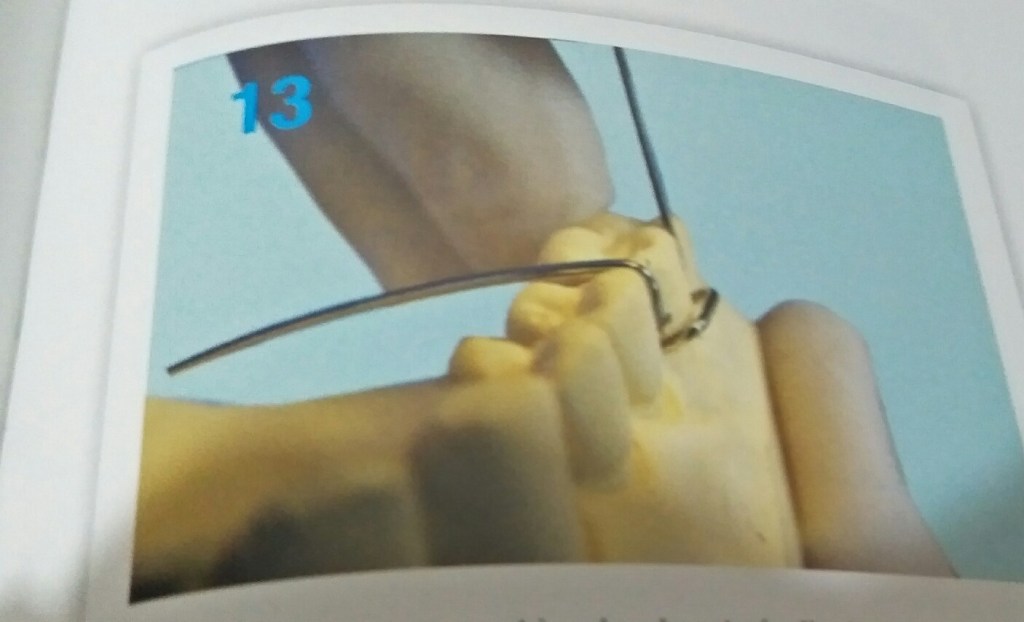
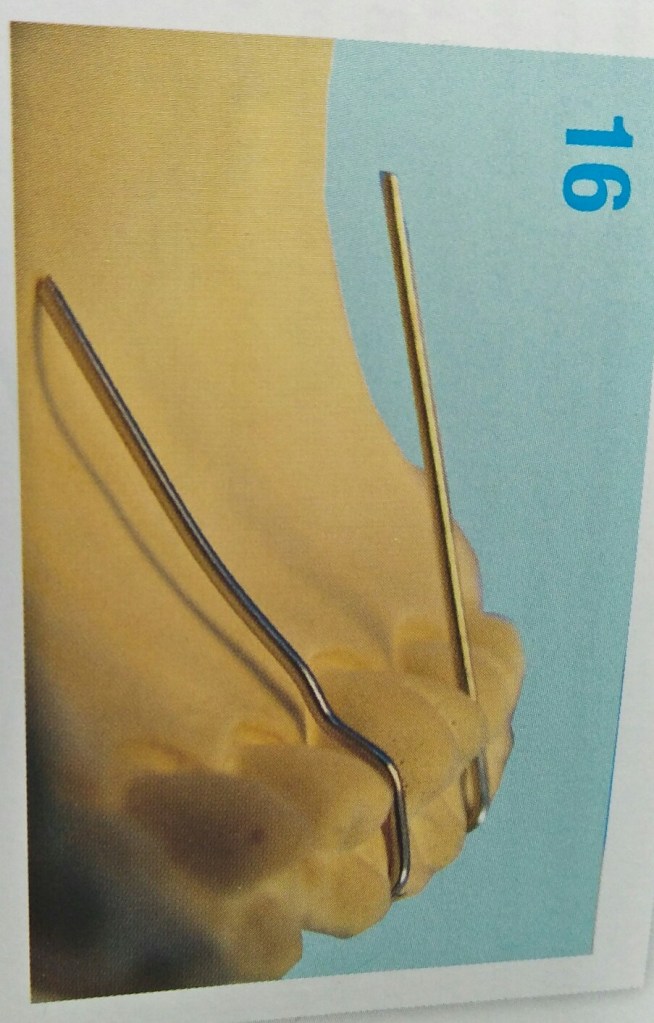
Parts of adams clasp-
- Two arrowheads
- Bridge
- Two retentive arms
Advantages of adams clasp-
- Rigid and offers excellent retention
- Fabricated on deciduous and permanent dentition
- Can be fabricated on fully or partially erupted tooth
- Can be used on molars, premolars and incisors.
- Small and occupies minimum space
- Can be modified in many ways.
- Universal pliers can be used for fabricating.
Modifications of adams clasp-
- Adams with single arrowhead
- Adams with J hook
- Adams with incorporated helix
- Adams with additional arrowhead
- Adams on incisor and premolars
- Adams with distal extension
Reference- Bhalajhi 7th edition