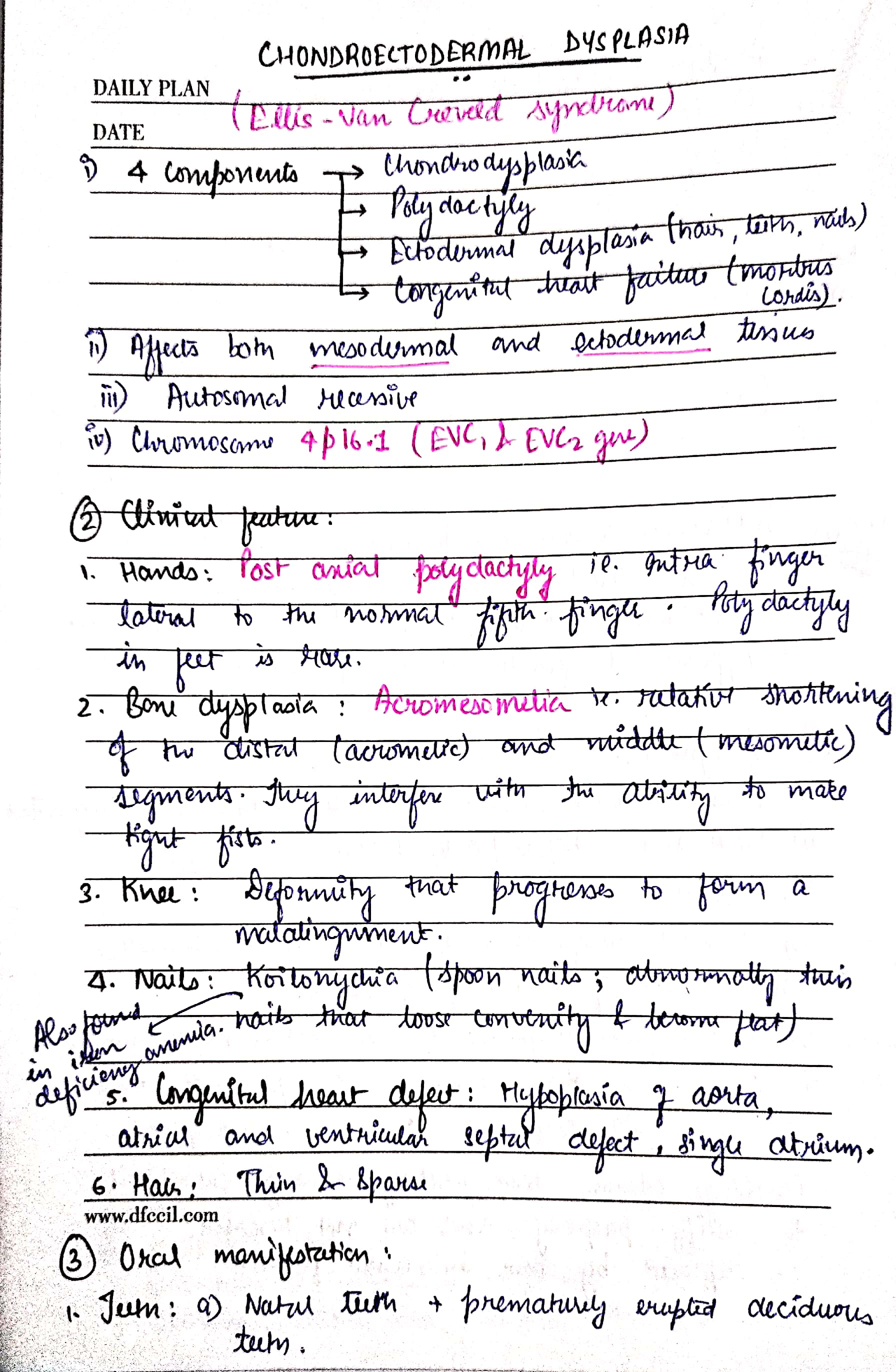
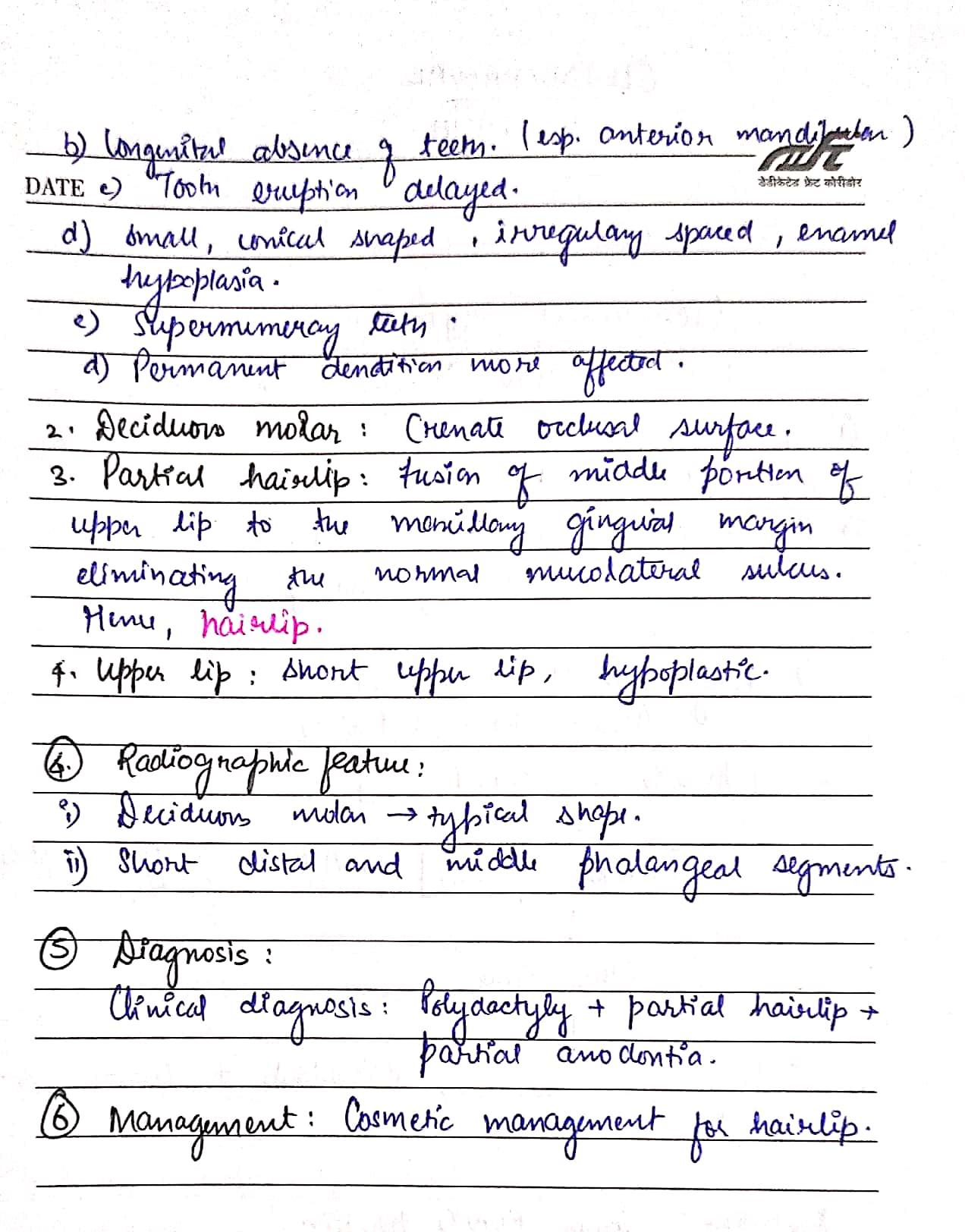
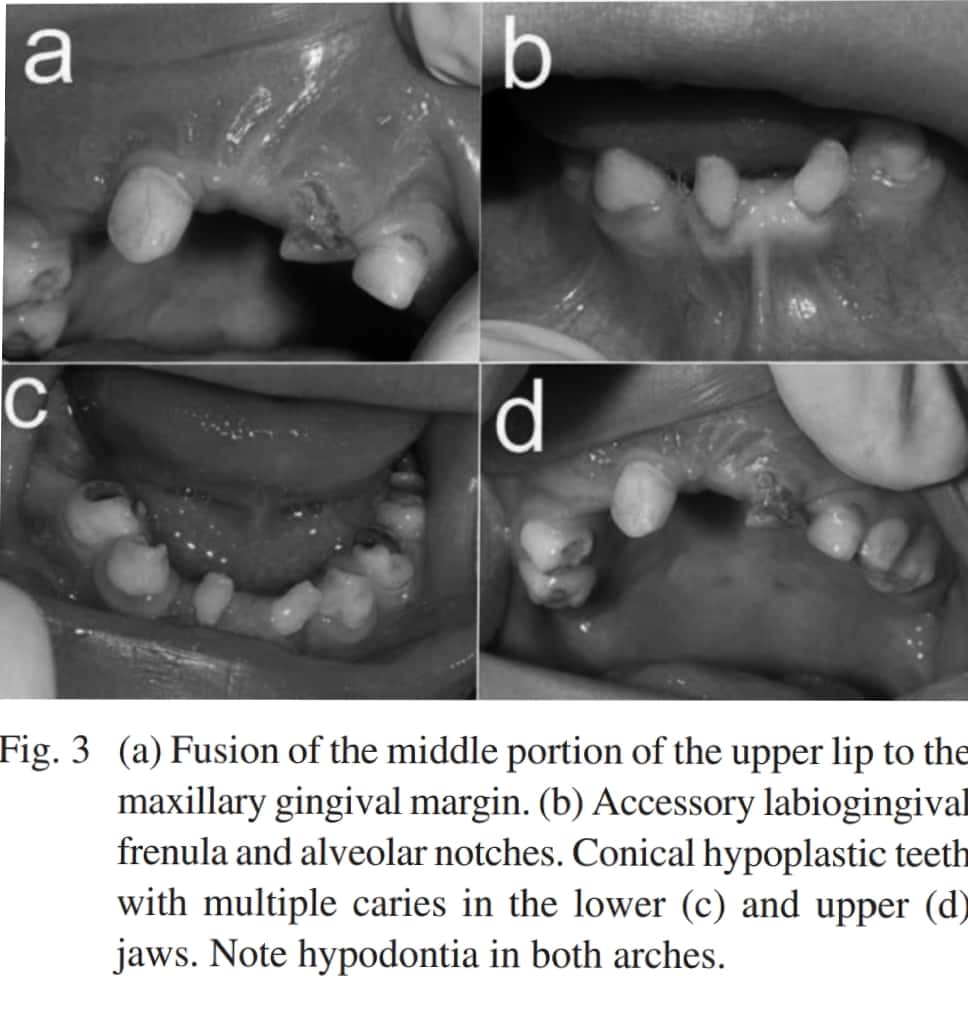
Ps. This is a good case report on Chondroectodermal dysplasia – https://api.semanticscholar.org/CorpusID:5721166
Sources – Shafer’s textbook of oral pathology
Image reference – Shafer’s textbook of oral pathology , semanticscholar.org




Ps. This is a good case report on Chondroectodermal dysplasia – https://api.semanticscholar.org/CorpusID:5721166
Sources – Shafer’s textbook of oral pathology
Image reference – Shafer’s textbook of oral pathology , semanticscholar.org
SINGLE STAGE V/S 2-STAGE SURGICAL PROCEDURES:
SURGICAL PROCEDURES:
There are 3 types:
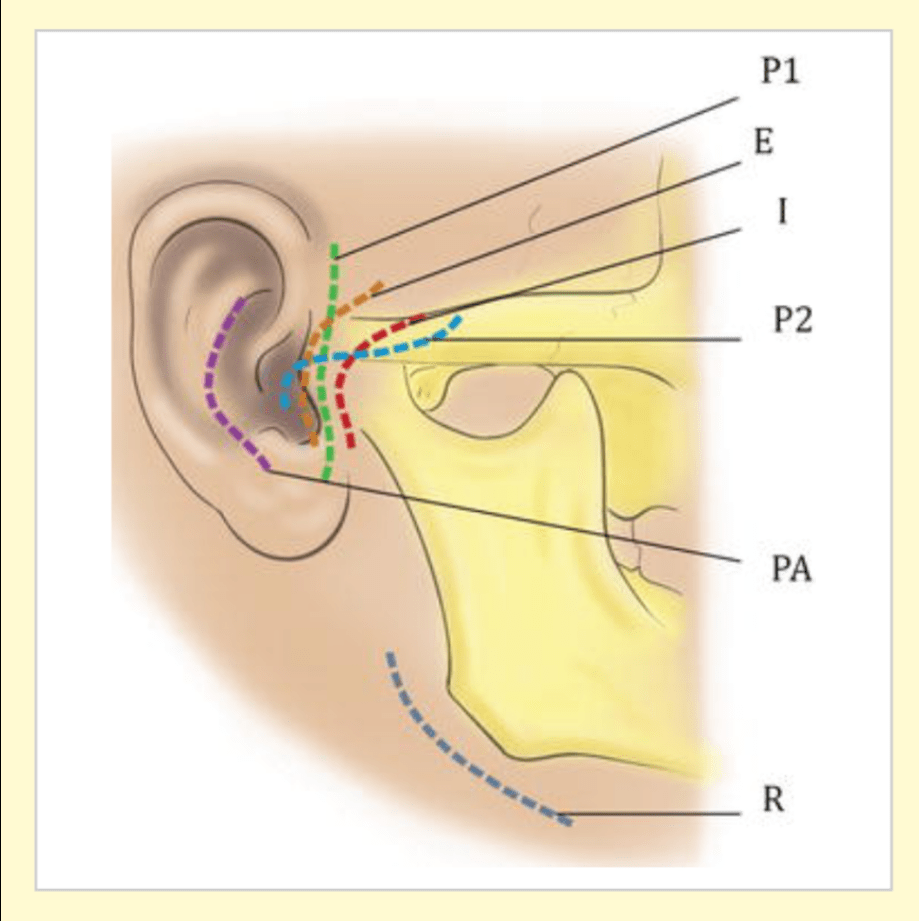
TMJ APPROACHES:
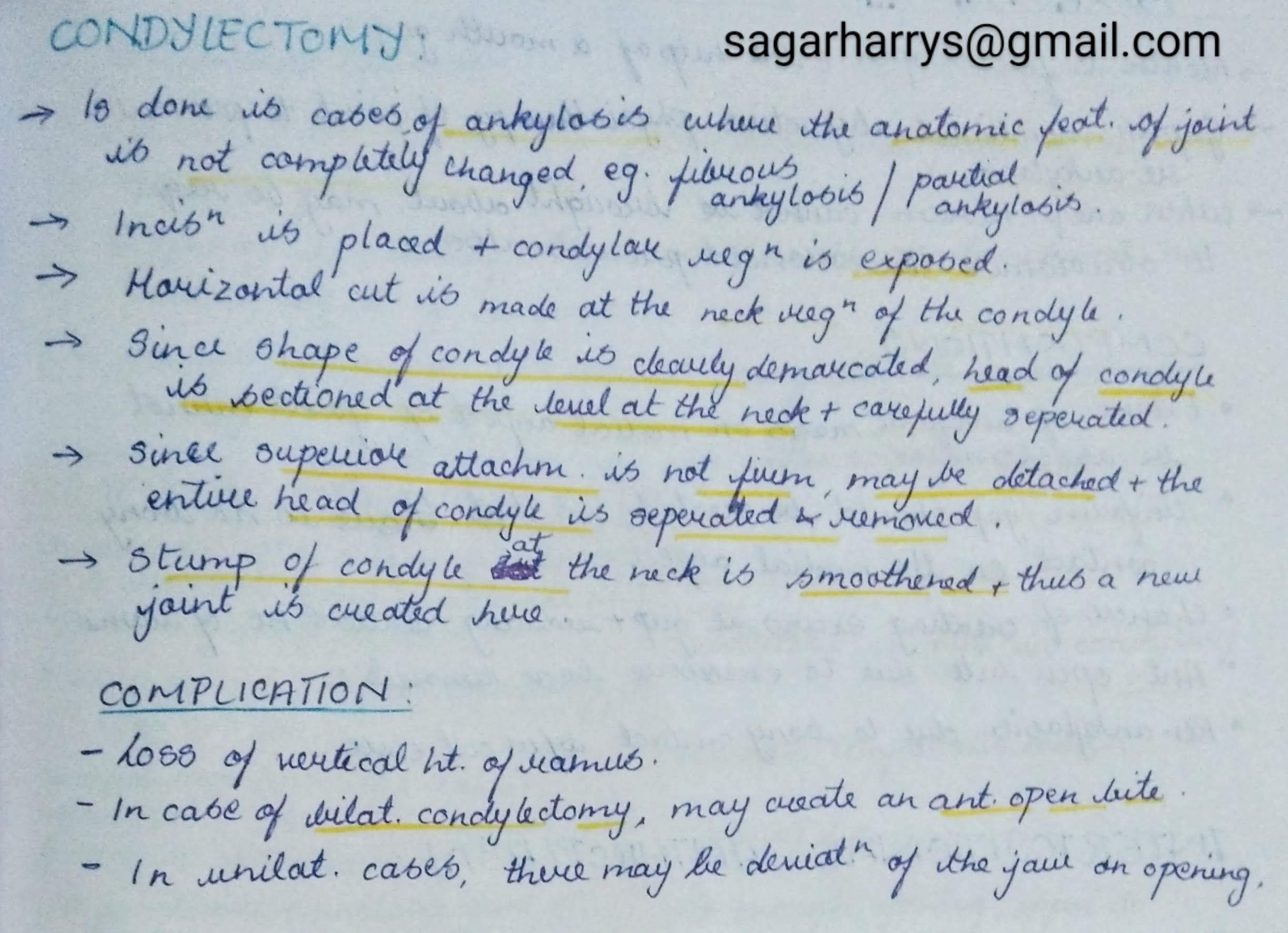
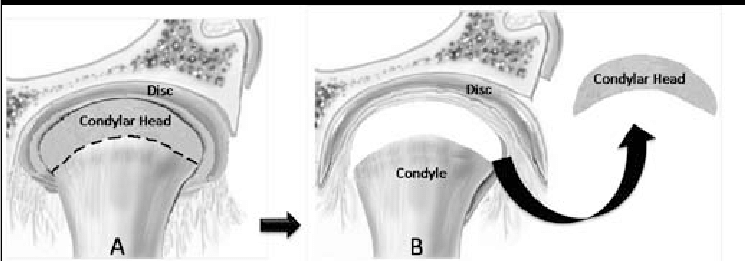
1. CONDYLECTOMY:
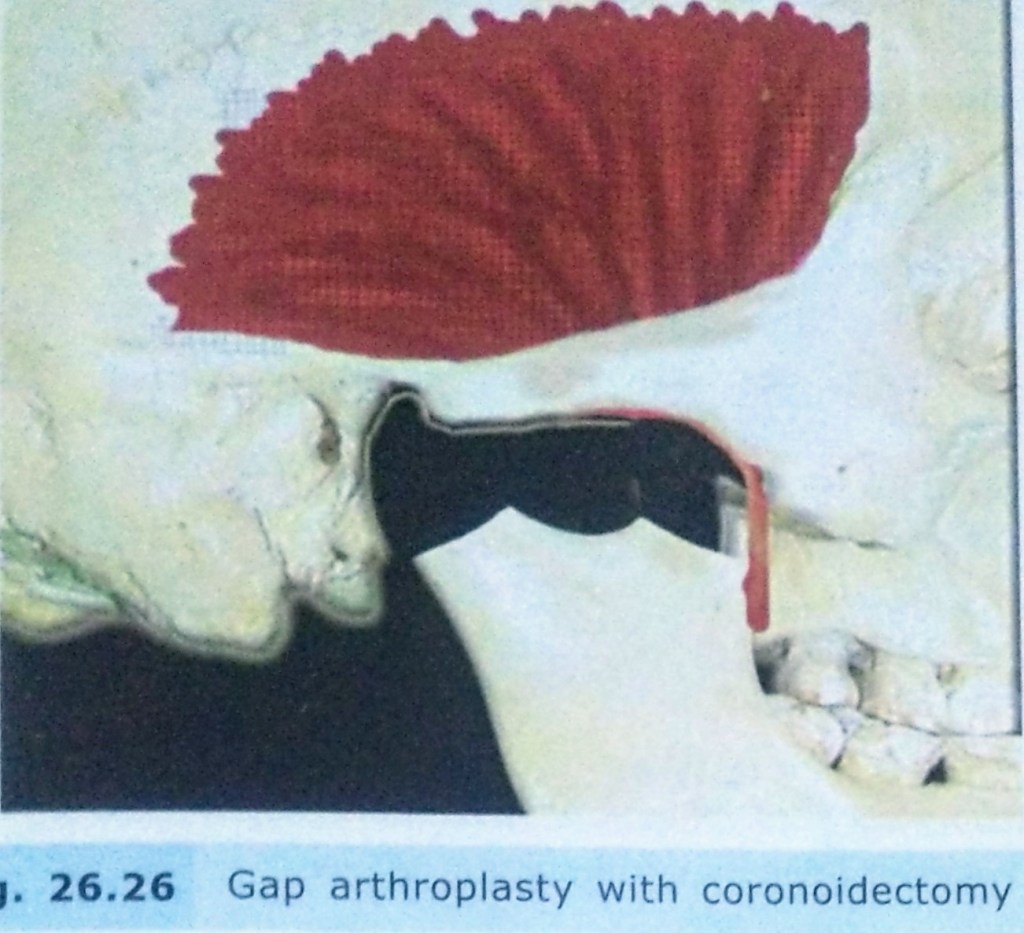
2. GAP ARTHROPLASTY:

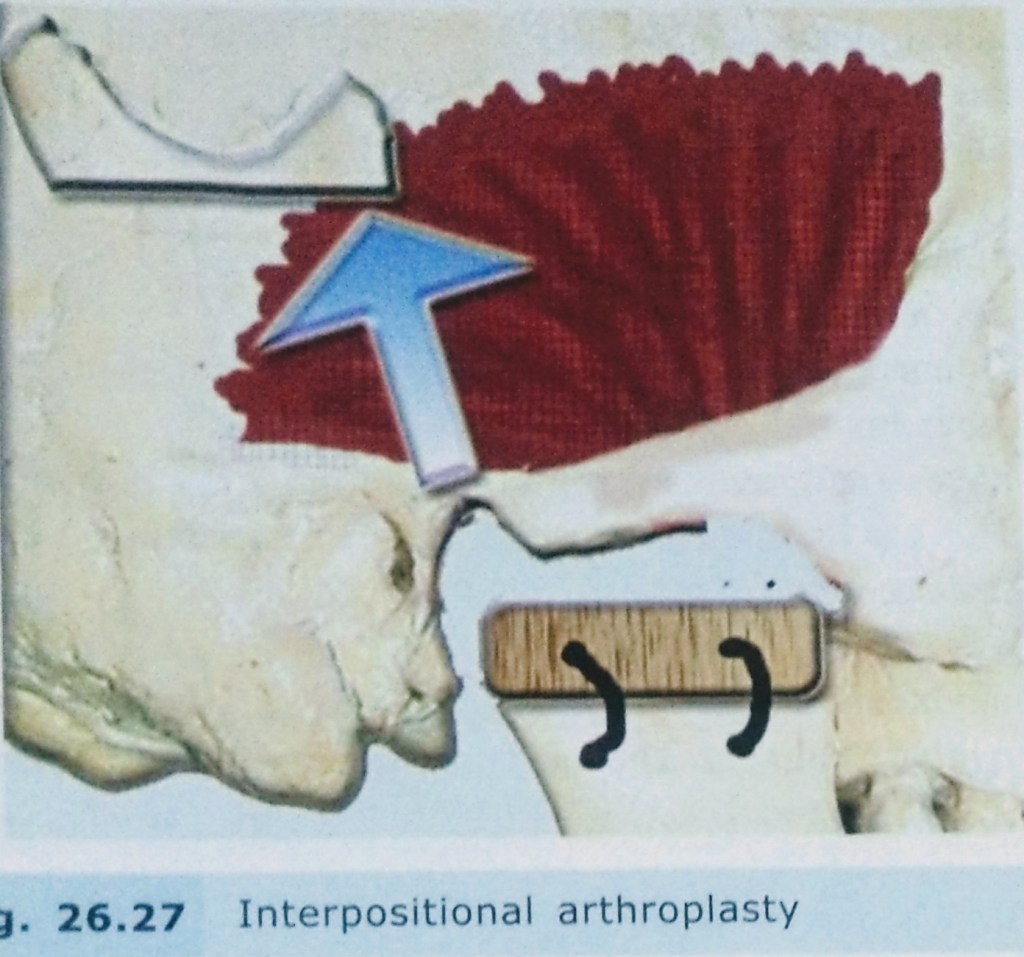
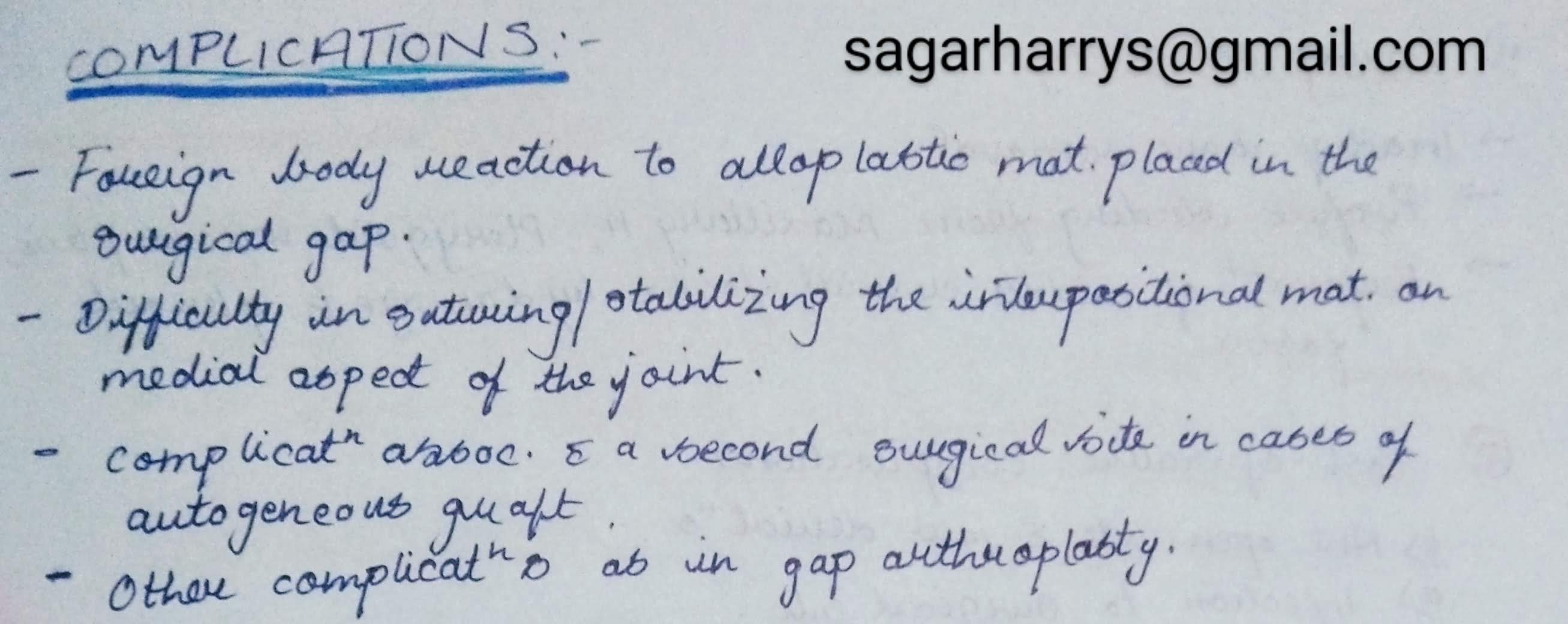
3. INTERPOSITIONAL ARTHROPLASTY:

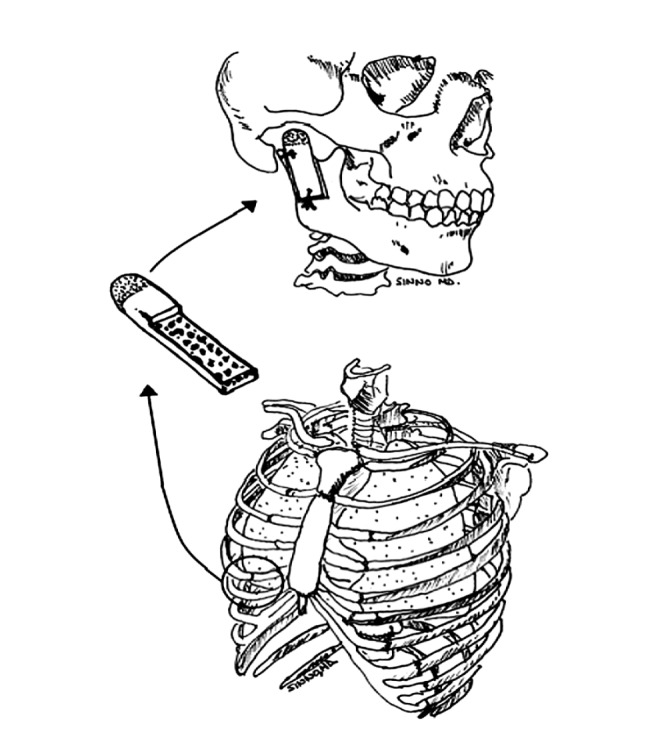
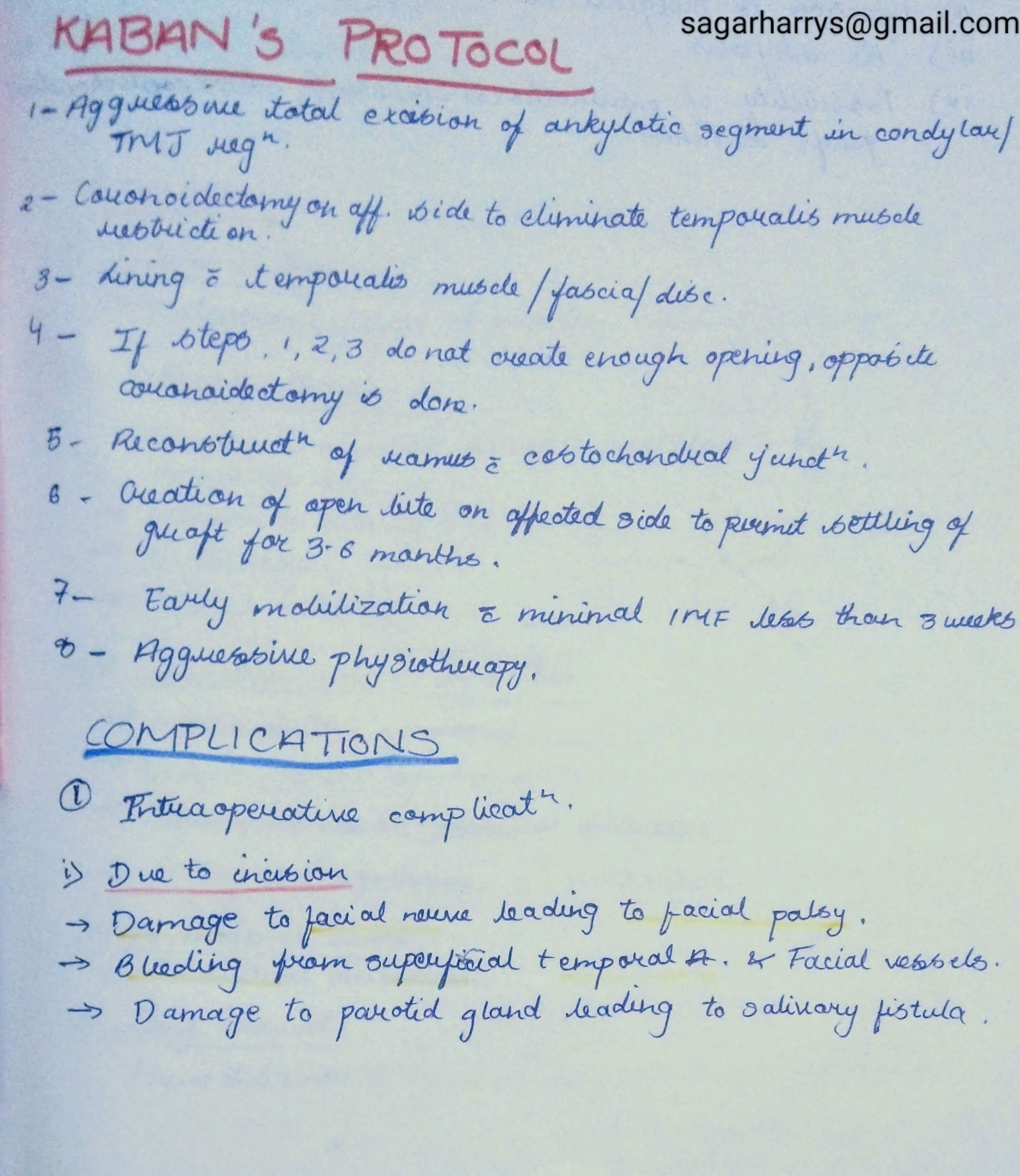
KABAN’S PROTOCOL:


REFERENCES:

CLASSIFICATION:
1. Based on type of tissue causing Ankylosis:


2. Based on the Side Involved :


3. Based on Severity of Ankylosis:
4. Based on Etiology of Trismus:
SAWHNEY’S CLASSIFICATION:

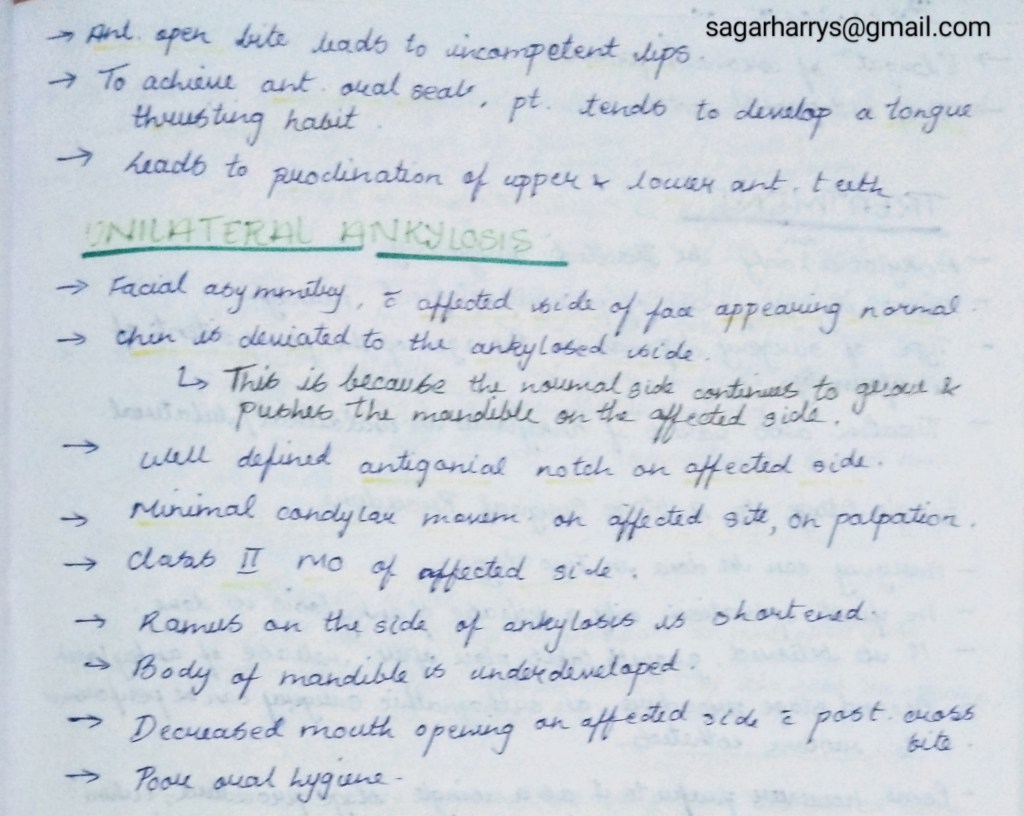
CLINICAL FEATURES:

INVESTIGATIONS:
1. Radiographs:
– OPG

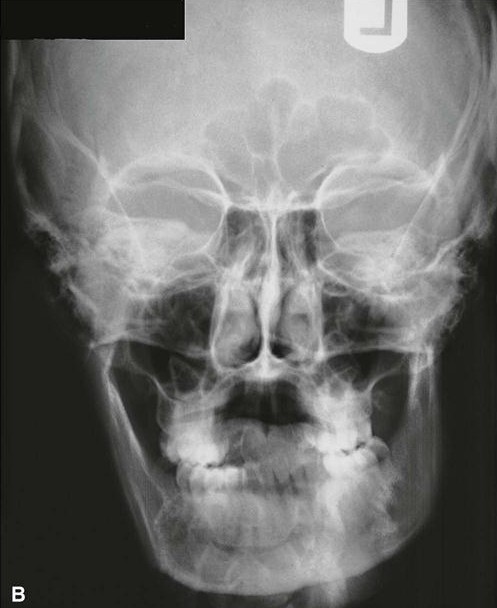
-PA VIEW:
– Lateral Oblique View of Mandible:
Ankylotic mass can seen in the Anteroposterior direction.
2. Lateral Cephalogram:

3. CT Scan:
Helpful as it gives an accurate picture of proximity of ankylotic mass to important structure,that cannot be seen in a radiograph.

RADIOGRAPHIC FEATURES:
REFERENCES:





REFERENCES:

Oral cancer is a disease with very poor prognosis because it is not recognised and treated when small and early.
INCIDENCE.
-Squamous cell (epidermoid) carcinoma comprises 90% of all oral malignant tumours and 5% of all human malignancies.
-The peak incidence in the UK and the USA is from 55 to 75 years of age, whereas in India it is from 40 to 45 years of age.
-Oral cancer is a very frequent malignancy in India, Sri Lanka and some Eastern countries, probably related to habits of betel-nut chewing and reversed smoking .
– There is a definite male preponderance.
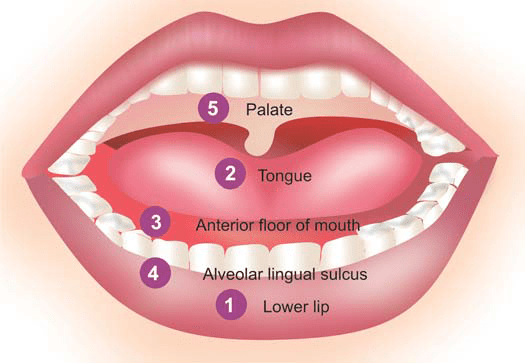
-It can occur anywhere in the mouth but certain sites are more commonly involved.
-These sites, in descending
order of frequency, are: the lips (more commonly lower),
tongue, anterior floor of mouth, buccal mucosa in the region
of alveolar lingual sulcus, and palate.
ETIOLOGY.
As with other forms of cancer, the etiology of squamous cell carcinoma is unknown. But a number of etiological factors have been implicated:
Strong association:
i) Tobacco smoking and tobacco chewing causing leukoplakia is the most important factor .
ii) Chronic alcohol consumption.
iii) Human papilloma virus infection, particularly HPV 16, 18 and 33 types.
Weak association:
i) Chronic irritation from ill-fitting denture or jagged teeth.
ii) Submucosal fibrosis as seen in Indians consuming excess of chillies.
iii) Poor orodental hygiene.
iv) Nutritional deficiencies.
v) Exposure to sunlight (in relation to lip cancer).
vi) Exposure to radiation.
vii) Plummer-Vinson syndrome, characterised by atrophy
of the upper alimentary tract.
The most common molecular alterations in oncogenes
seen in squamous cell carcinoma of the oral cavity are in
p16, p53, cyclin D, p63, PTEN, and EGFR.
MORPHOLOGIC FEATURES.
Grossly, squamous cell carcinoma of oral cavity may have the following types
i) Ulcerative type—is the most frequent type and is
characterised by indurated ulcer and firm everted or
rolled edges.
ii) Papillary or verrucous type—is soft and wart-like growth.
iii) Nodular type—appears as a firm, slow growing submucosal nodule.
iv) Scirrhous type—is characterised by infiltration into
deeper structures.

*All these types may appear on a background of leukoplakia or erythroplasia of the oral mucosa.
Enlarged cervical lymph nodes may sometimes be present.
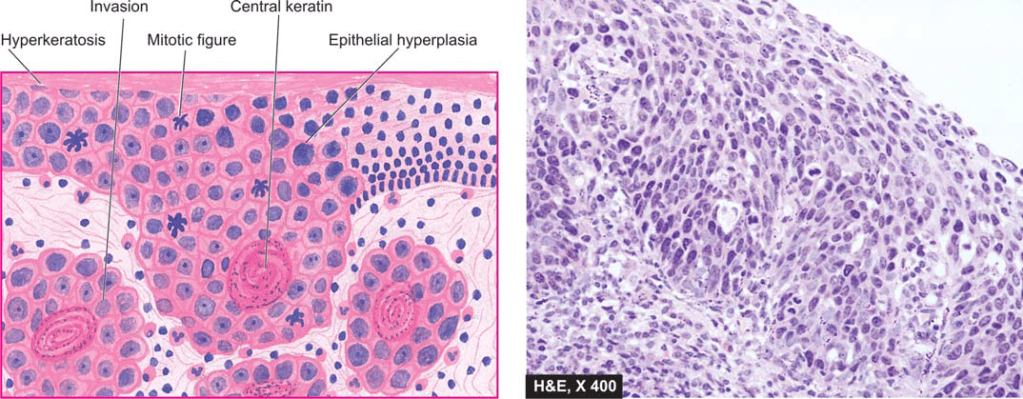
Histologically.
– squamous cell carcinoma ranges from well-differentiated keratinising carcinoma to highly undifferentiated neoplasm . -Changes of epithelial dysplasia are often present in the surrounding
areas of the lesion.
–Carcinoma of the lip and intraoral squamous carcinoma are usually always well-differentiated
source -textbook of pathology for dental students harsh mohan
A chronic, autoimmune, sub-epidermal blistering skin disease that rarely involves mucous membrane.

Age: Elderly (>60 years)
Skin Lesions:
Oral Manifestations:
Vesicles appear gingivally👇🏻

Erythematous & desquamate as result of minor frictional trauma
👉🏻 Oral lesions comprise of bullae/vesicle that rupture to form erosions and ultimately leave out ulcerations
👉🏻 Other sites:

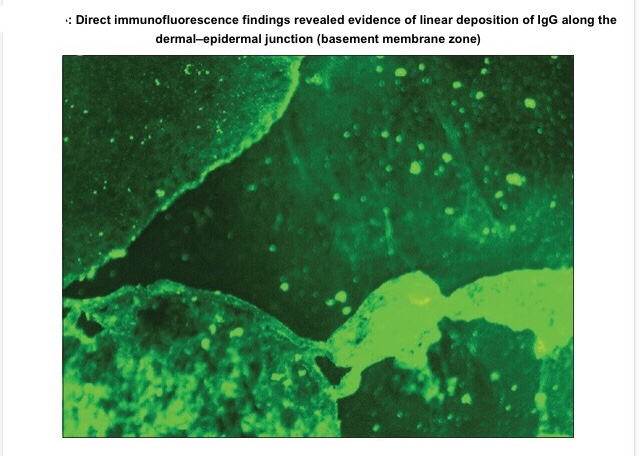
Apart from evaluating history, clinical presentation, histopathological analysis is carried out followed by direct immunofluorescence study for the differential diagnosis and confirmation of the condition.
👉🏻Histopathology:
👉🏻Direct immunofluorescence is found to be the gold standard test. Deposition pattern of different types of immunoreactants differentiates the various immune-mediated diseases. Direct immunofluorescence shows presence of IgG and C3 deposits along the basement membrane zone.
👉🏻Electron Microscopy: In bullous pemphigoid (BP), the 180 kD antigen (BPAG2) was shown by immuno-EM to be a transmembrane molecule and to possess an autoantibody binding site outside the cell, suggesting a major pathogenic role for the BPAG2 in blister formation.
• Mucous membrane pemphigoid can be differentiated from BP by its predominant involvement of mucosal surfaces and positive Nikolsky’s sign.
• Lichen planus pemphigoides is clinically differentiated by the presence of lichen planus lesions in addition to tense blisters.
• Nikolsky’s sign is present in case of pemphigus and cicatricial pemphigoid, but not in the case of BP.
👉🏻Treatment is based on the degree of cutaneous and oral involvement. Mostly, topical steroid (clobetasol propionate) gives satisfactory result in case of smaller area of skin involvement, whereas larger area of skin involvement and recurrent cases are treated satisfactorily with systemic steroids and immunosuppressive agents.
👉🏻Recommended dosage for oral prednisolone is 0.3–1.25 mg/kg body weight/day, controls disease within 1–2 weeks, followed by which the dose is tapered. Dexamethasone (100 mg in 500 mL 5% dextrose i.v. over 2–3 h for three consecutive days) is the preferred steroid for pulse therapy, either administered alone or in combination with cyclophosphamide.
Other drugs for treating BP include new antibody modulators, rituximab 375mg/m2weekly over 4 weeks and omalizumab subcutaneously 300–375 mg for every 6 weeks.
👉🏻Higher doses of systemic corticosteroids seem to be associated with higher mortality rates, which led to the addition of corticosteroid-sparing agents to the treatment of BP. The most frequently used immunosuppressive agent is azathioprine (0.5–2.5 mg/kg body weight/day). Others being cyclophosphamide, methotrexate, cyclosporine A, combination tetracycline/minocycline along with nicotinamide, and more recently, mycophenolate mofetil, a DNA synthesis inhibitor, and methotrexate, a folate antagonist.
👉🏻IVIg – A dose of 1–2 g/kg for five consecutive day cycle of 0.4 g/kg/day, although a 3-day cycle may be used in cases that are nonresponsive to conventional therapy.
Dr. Mehnaz Memon🖊
References:
DEFINITION- Leukoplakia (white plaque) may be clinically
defined as a white patch or plaque on the oral mucosa, exceeding 5 mm in diameter, which cannot be rubbed off nor can be classified into any other diagnosable disease.
–the term ‘leukoplakia’ is reserved for epithelial thickening which may range from completely benign to atypical and to premalignant cellular changes.
INCIDENCE–
1. It occurs more frequently in males than
females.
2.The lesions may be of variable size and appearance.
3. The sites of predilection, in descending orderof frequency, are: cheek mucosa, angles of mouth, alveolar mucosa, tongue, lip, hard and soft palate, and floor of the mouth.
4.In about 4-6% cases of leukoplakia, carcinomatous
change is reported.
ETIOLOGY-
1. It has the strongest association with the use of tobacco in various forms, e.g. in heavy smokers (especially in pipeand cigar smokers) and improves when smoking is discontinued, and in those who chew tobacco as in paan, paan masaala, zarda, gutka etc.
2.The condition is also known by other names such as smokers keratosis and stomatitis nicotina.
3. Other etiological factors implicated are chronic friction such as with ill-fitting dentures or jagged teeth, and local irritants like excessive consumption of alcohol and very hot and spicy foods and beverages.
4. A special variety of leukoplakia called ‘hairy leukoplakia’ has
been described in patients of AIDS and has hairy or corrugated surface but is not related to development of
oral cancer.

MORPHOLOGIC FEATURES.
1.Grossly, the lesions of leukoplakia may appear white, whitish-yellow, or redvelvety of more than 5 mm diameter and variable in appearance.
2. They are usually circumscribed, slightly elevated, smooth or wrinkled, speckled or nodular.
Histologically, leukoplakia is of 2 types:
-The subepithelial tissues usually show an inflammatory infiltrate composed of lymphocytes and plasma cells.
– The extent and degree of the epithelial changes indicate the degree of severity of the epithelial dysplasia.
-Usually, mild dysplasia may revert back to normal if the offending etiologic factor is removed, whereas severe dysplasia indicates that the case may progress to carcinoma.

source – textbook of pathology for dental students harsh mohan











Sources – Anil Ghoms textbook of oral medicine , osmosis.org
Image source – researchgate.net , Google images

🔖 Acrocephalosyndactyly. The condition is autosomal dominant i.e, one copy (out of 2) of the defective gene is sufficient to cause the abnormality in the offspring.
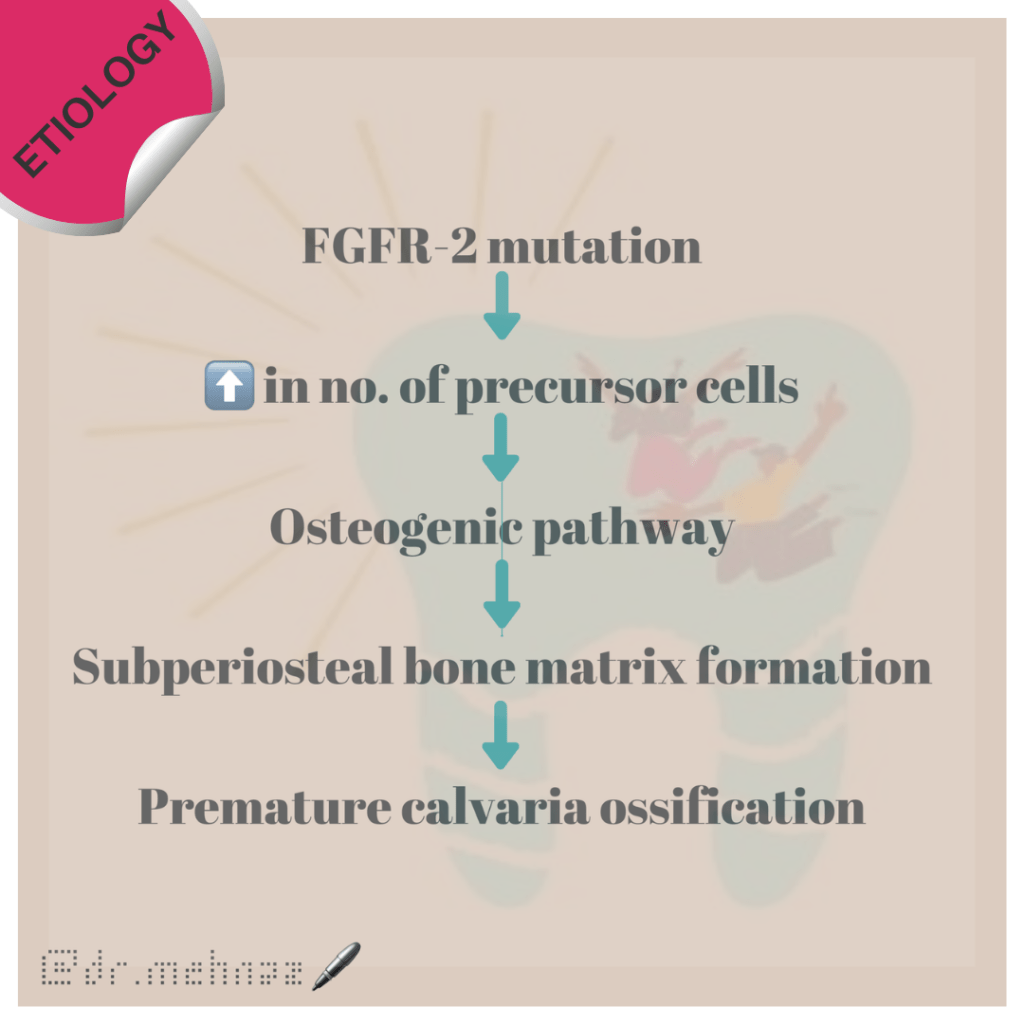
The various clinical features include:

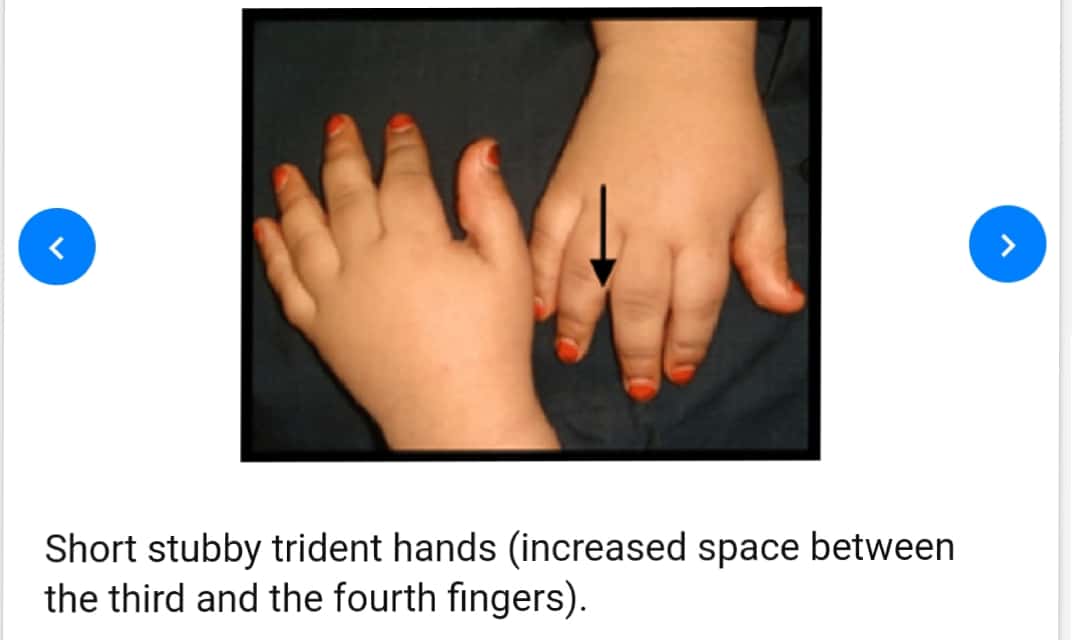
8. Partial to complete fusion of digits: 2-4th digits – MITTEN HANDS & SOCK FEET; Sole – supinated
9. Intelligence – Normal
10. ⬆️ intracranial pressure – optic atrophy, papilledema
11. Hyperhidrosis
12. Cardiovascular system: Atrial Septal defect, Ventricular septal defect, Patent ductus Arteriosus
Standard Therapies
The treatment of Apert syndrome aims at addressing the specific symptoms that may be present in the particular individual. Treatment is usually symptomatic and supportive.
Dr. Mehnaz Memon🖊
References:
