Correct and early diagnosis of a lesion / abnormality in the oral cavity is very crucial as these could be vital indicators to some of the underlying systemic diseases or other chronic conditions. Most of the oral conditions show a peculiar pattern of occurrence only on specific sites.Hence,knowledge of these common sites can help to some extent in proper identification, differentiation from other similar conditions and treatment planning.A few of such conditions and findings has been mentionedhere.
Sources:Shafers textbook of oral pathology ,burkets oral medicine ,www.aurametrix.weebly.com
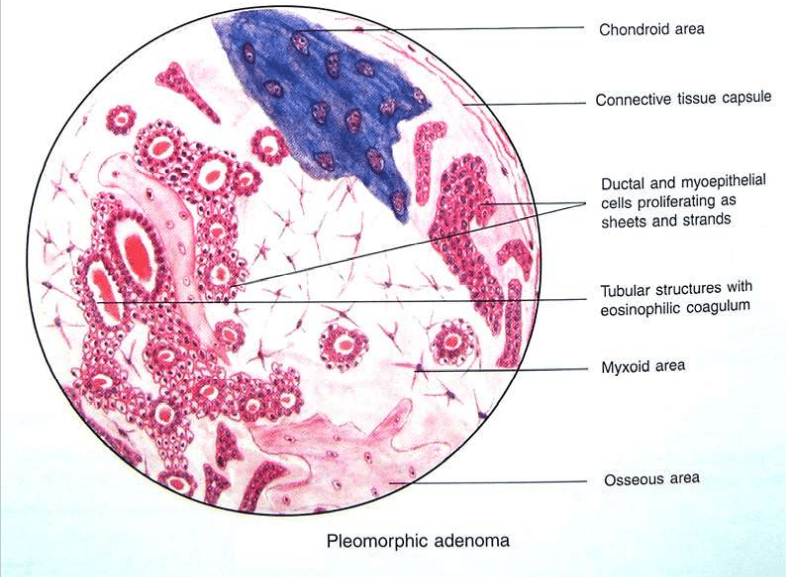
Name suggested by Willis. Most common neoplasm of salivary gland tumor. Benign neoplasm- consisting of cells exhibiting the ability to differentiate to epithelial (ductal and nonductal) cells and mesenchymal (chondroid, myxoid, osseous) cells. Other names:
Branchioma,
enclavoma,
teratoma,
cyindroma,
myxochondrocarcinoma.
Salivary gland tumor origin: EPITHELIAL
Shows cytogenic abnormalities in chomosomes- 12q13-15. Putative pleomorphic adenoma gene(PLAG1) has been mapped to chromosomes 8q12
Histogenesis:-
Currently, numerous theories centre around the myoepithelial cell and the reserve cell in the intercalated duct.
Ultrastructural studies have confirmed the presence of both ductal and myoepithelial cells in pleomorphic adenomas.
It follows that possibly either or both may play active roles in the histogenesis of the tumour.
Hubner and his associates:- have postulated that the myoepithelial cell is responsible for the morphological diversity of the tumour, including the production of the fibrous, mucinous, chondroid and osseous areas.
Regezi and Batsakis:- postulated that the intercalated duct reserve cell can differentiate into ductal and myoepithelial cells, and the latter, in turn, can undergo mesenchymal metaplasia, since they inherently have smooth muscle-like properties. Further differentiation into other mesenchymal cells then can occur.
Batsakis:- has discussed salivary gland tumourigenesis, and while still implicating the intercalated duct reserve cell as the histogenetical precursor of the pleomorphic adenoma, stated that the role of the myoepithelial cell is still uncertain and that it may be either an active or a passive participant histogenetically.
Finally, Dardick and his associates have questioned the role of both ductal reserve and myoepithelial cells. They stated that a neoplastically altered epithelial cell with the potential for multidirectional differentiation might be histogenetically responsible for pleomorphic adenoma.
CLINICAL FEATURES:-
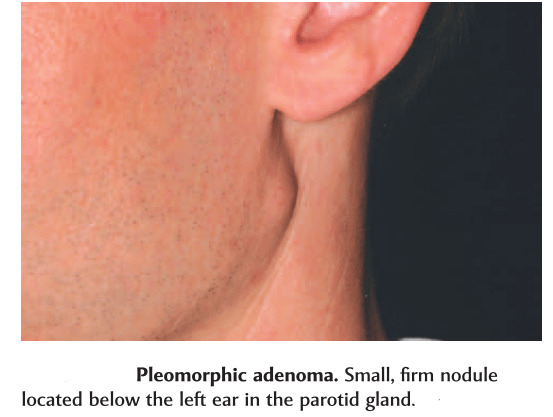
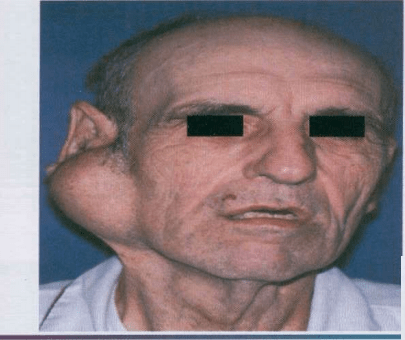
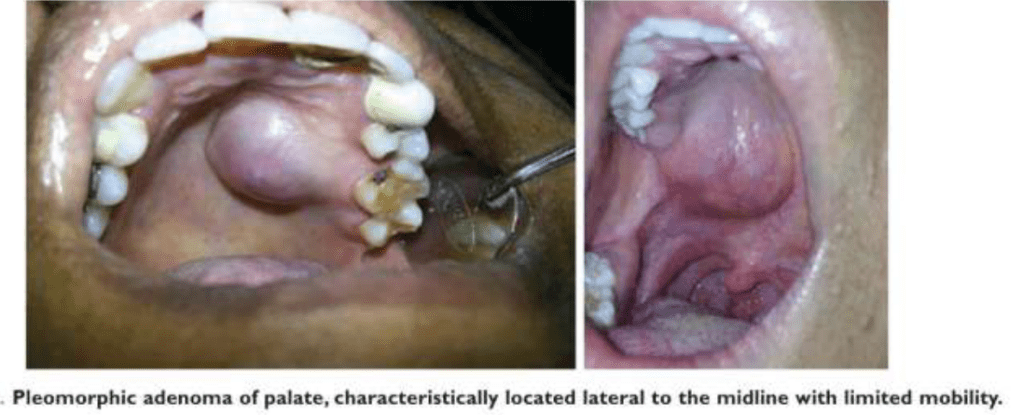
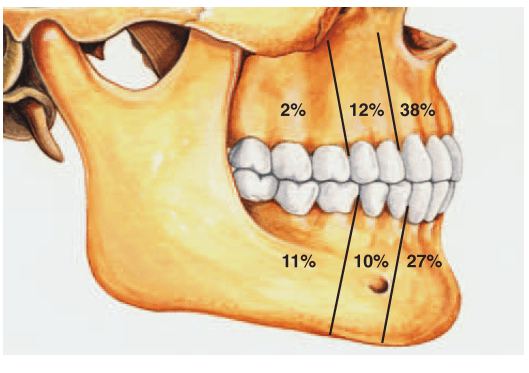
Most common tumor. Rate of occurance: 60-70%- parotid glands 40-60%- submandibular glands 40-70%- minor salivary glands seldomly- sublingual glands Age: 30-50 years Sex: female> male – 3:1 – 4:1 In parotid- presents in the lower lobe of the superior lobe as a mass over the angle of the mandible, below and infront of the ear.
Clinical presentation: painless, slow growing, firm mass, initially small in size and begins to increase in size. Initially movable but with continued growth become more nodular and less movable. Recurrent tumor- multinodular, fixed on palpation. Palate – intraorally common site. Seldom ulcerated- unless secondarily traumatized.
Slowly growing tumor of The parotid gland.
HISTOPATHOLOGY:-
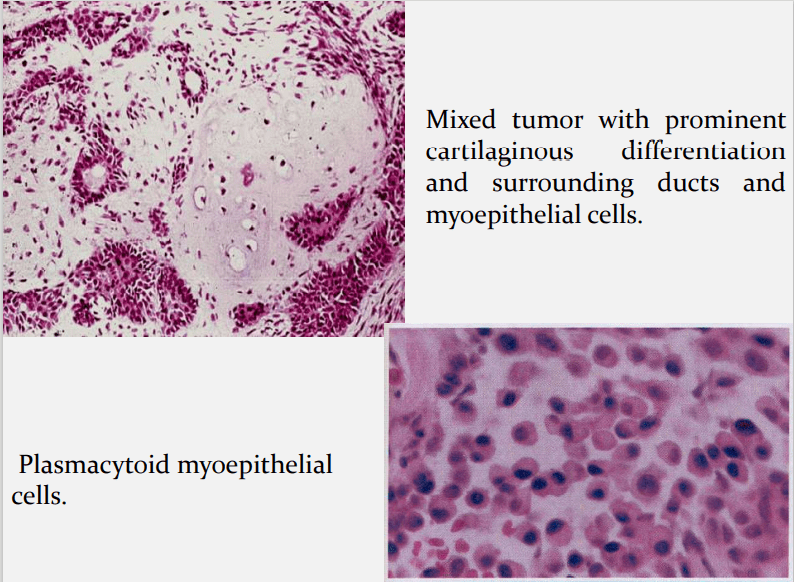
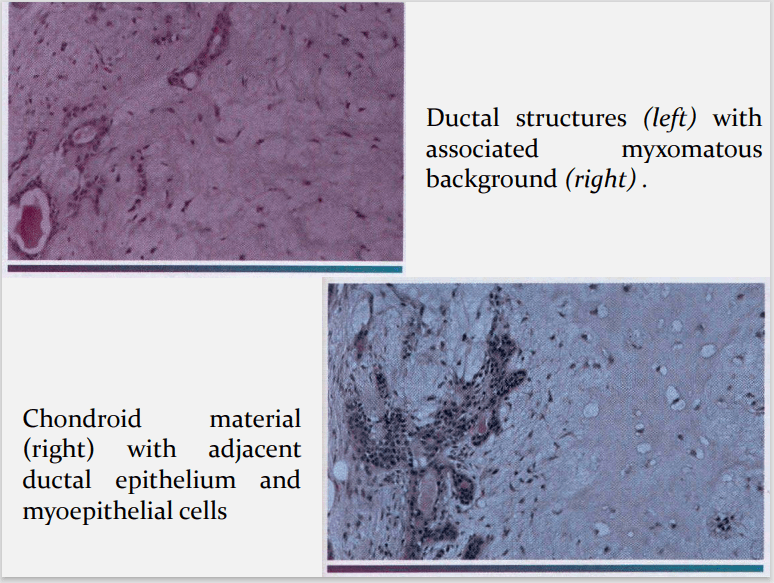
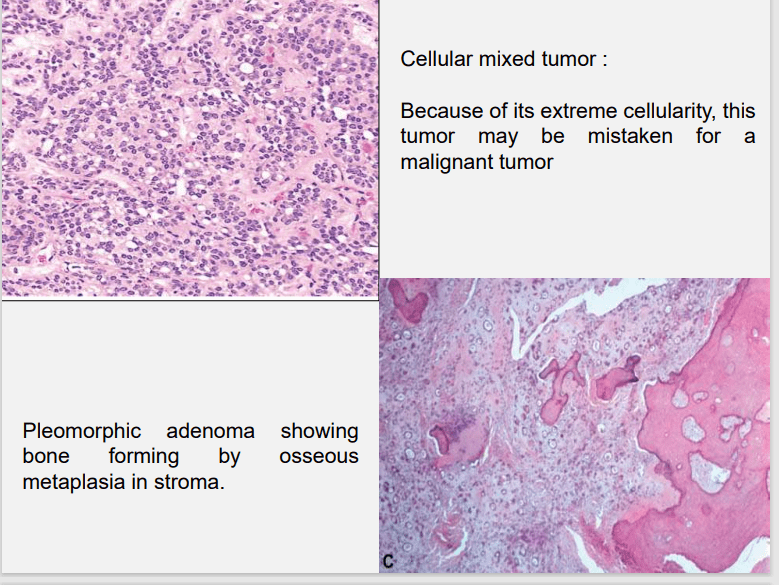
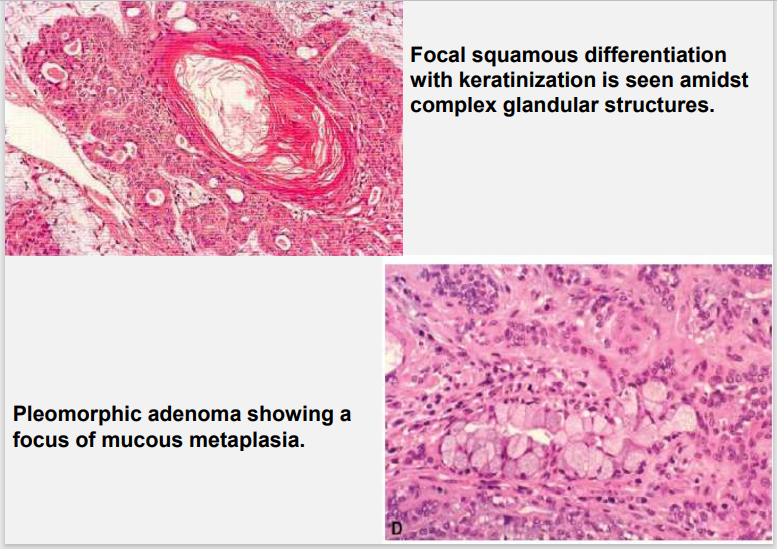
HALLMARK: Morphologic Diversity. Charecterized by- Variable, Diverse, Structural & histologic patterns. It demonstrate glandular epithelium and mesenchyme like tissue and the proportion of each component varies widely. Typically a well-circumscribed encapsulated tumor The epithelium often forms ducts and cystic structures or may occur as islands or sheets of cells , anastomosing cords and foci of Keratinizing squamous cells and spindle cells .
Foote and Frazell (1954) categorized PA into: a) Primarilly myxoid (36%) b) Myxoid and cellular component in equal proportions (30%) c) Predominantly cellular (22%) d) Extremely cellular (12%)
Myoepithelial cells are major component of PA. Have variable morphology- sometimes appearing as angular or spindled, some with eccentric nucleus resembling plasma cells. Are responsible for characteristic mesenchyme like changes. Vacuolar degeneration of myoepithelial cells can produce a chondroid appearance. the stroma exhibits areas of an eosinophilic hyalinized change, fat or osteoid also is seen.
Surgical excision Superficial parotidectomy with preservation of the facial nerve Local enucleation should be avoided – resulting in seeding of the tumor bed. Deep lobe of the parotid- total parotidectomy is usually necessary also with preservation of the facial nerve.
Submandibular tumors – Total removal of the gland with the tumor. Malignant degeneration is a potential complication, resulting in a carcinoma ex pleomorphic adenoma. The risk of malignant transformation is probably small, but it may occur in as many as 5% of all cases.
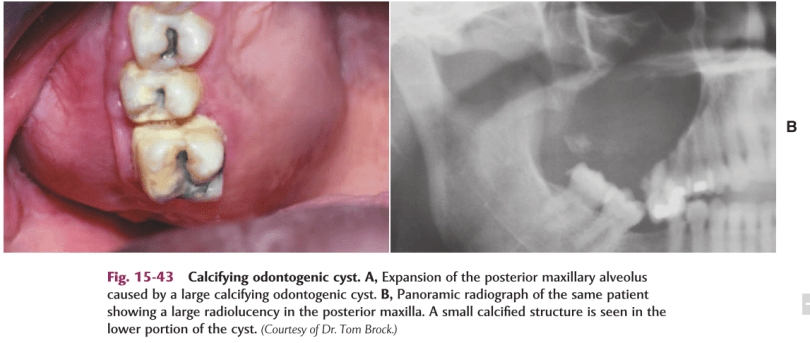
DEF:-Calcifying odontogenic cyst (COC), previously known as Gorlin cyst, is a rare, well-circumscribed, solid or cystic lesion derived from odontogenic epithelium that resembles follicular ameloblastoma but contains ‘ghost cells’ and spherical calcifications.
It Has many features of odontogenic tumor, therefore it is placed in the category of tumors in the latest WHO classification of odontogenic cysts and tumors.
In the latest WHO publication on odontogenic tumours (Prætorius and Ledesma-Montes, 2005) it was classified as a benign odontogenic tumour and was renamed calcifying cystic odontogenic tumour (CCOT).
CLINICALFEATURES:-
Age : Wide range, peak in 2nd decade.
Sex : Equal.
Site : Anterior segment of both jaws
Calcifying odontogenic cysts that are associated with odontomas tend to occur in younger patients, with a mean age of 17 years.
PATHOGENESIS:-
COC is a unicystic process and develops from the reduced dental epithelium or remnants of dental lamina.
The cyst lining has the potential to induce formation of dentinoid or even odontoma in adjacent CT wall.
CLASSIFICATION OF THE ODONTOGENIC GHOST CELLLESIONS:-
Group 1 : ‘Simple’ cysts Calcifying odontogenic cyst (COC)
Group 2 : Cysts associated with odontogenic hamartomas or benign neoplasms: calcifying cystic odontogenic tumours (CCOT).
Group 3 : Solid benign odontogenic neoplasms with similar cell morphology to that in the COC, and with dentinoid Formation
.Group 4 : Malignant odontogenic neoplasms with features similar to those of the dentinogenic ghost cell tumour Ghost cell odontogenic carcinoma.
SIGNS &SYMPTOMS:-
Swelling is the commonest complaint, seldom associated with pain.
Intraosseous lesions can cause hard bony expansion and resulting facial asymmetry.
Displacement of teeth can also occur.
RADIOLOGICALFEATURES:-
Intraosseous lesions produce well defined lucency which is usually unilocular.
Irregular calcified masses of varying sizes may be seen within the lucency.
Displacement of root/roots with or without root resorption and expansion of cortical plates also seen.
*Radiograph of a calcifying odontogenic cyst with well-demarcated margins extending from the right to the left premolar regions of the mandible. Numerous calcifications are present, some suggestive of small denticles.
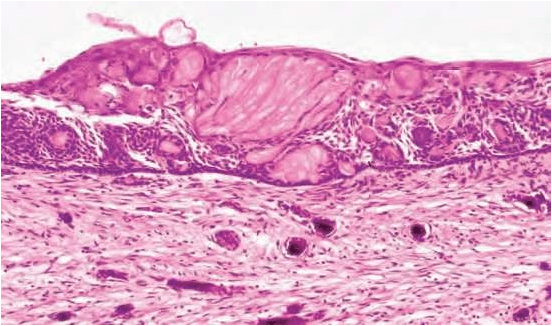
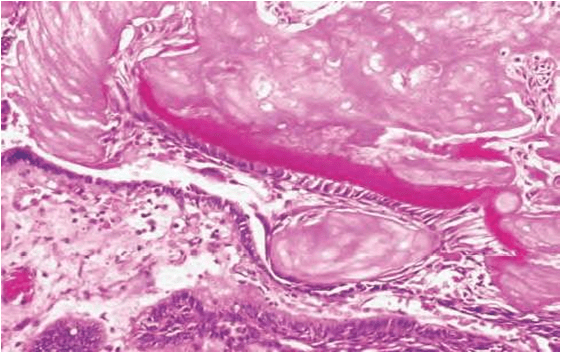
HISTOLOGICALFEATURES:-
Lining is usually thin about 6 – 8 cell thick, may be thickened in other areas.
Lining shows characteristic odontogenic features with reversely polarized basal cell layer.
TYPICALLY – GHOST CELLS may be seen in thicker areas of lining.
Ghost cells are enlarged, ballooned, ovoid, eosinophilic cells with well
defined cell boundaries.
5.Some times many cells may fuse.
6.They represent abnormal keratinization and frequently calcify.
7.Tubular dentinoid and even complex odontome may be found in connective tissue wall close to epithelial lining.
Histological features of a calcifying odontogenic cyst with clusters of fusiform ghost cells and focal calcifications, lying in a stratified squamous epithelium.In this calcifying odontogenic cyst, there are sheets of ghost cells and a focal area in which there has been induction of a strip of dysplastic dentine (dentinoid).
DIFFERENTIALDIAGNOSIS:-
Based on radiographic appearance, following lesions must be included in the provisional diagnosis –
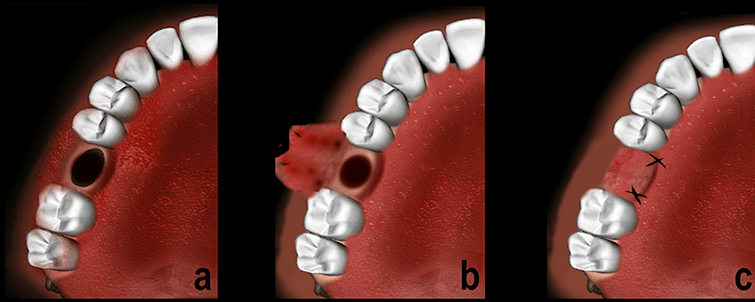
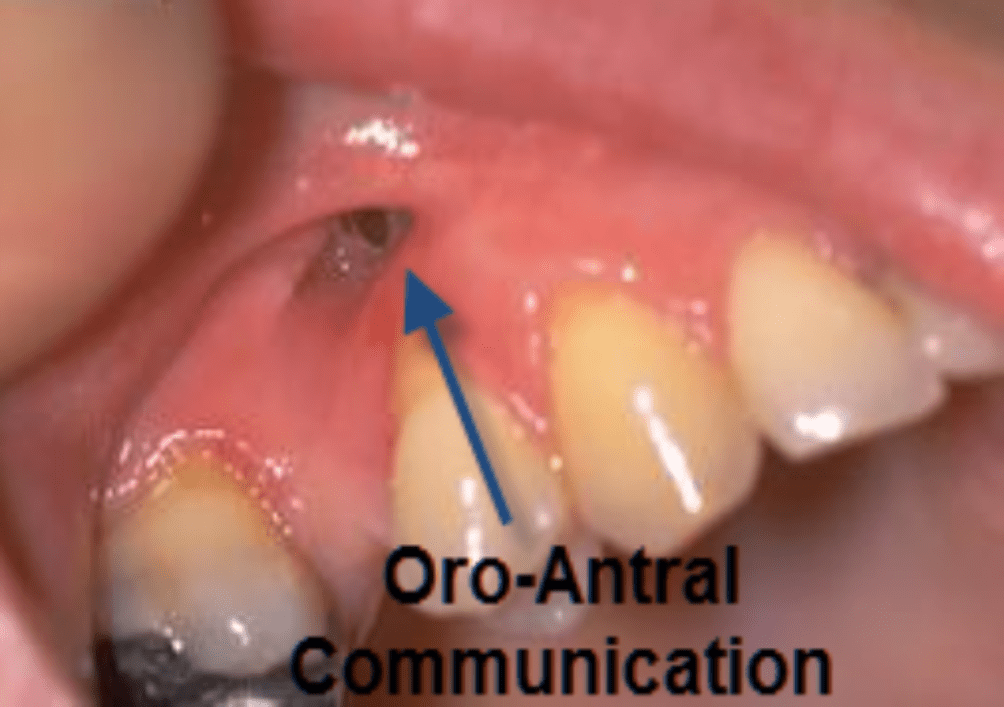
This technique is very similar to buccal advancement technique where the gingiva is close to the oroantral defect is mildly advanced to approximate it.
May be done for small sized defects.
It is not possible to get too much of advancement, as the palatal tissue is very rigid and thick.
In this,the palatal tissue surrounding the OAC, is reflected +may be advanced downwards and sutured to the buccal tissue to cover the detect.
Not a very successful procedure.
ROTATIONAL ADVANCEMENT FLAP or ASHLEY’S FLAP OPERATION:
• It is posteriorly based flap which gets its supply from the greater palatine artery. • Local anesthesia is infiltrated on the palatal aspect. Infilteration is also given on the buccal side of the oroantral defect. • Removal of fistula tract and clearing any signs pathology. • The flap is outlined with surgical marking an excess of what appears to be required to rotate the flap. • Incision is placed to the bone making sure the palatal pedicle is kept intact. • A full thickness mucoperiosteal flap is reflected with care taken to visualize the greater palatine vessels. • A small amount of tissue along the margin of the defect on the buccal aspect is also reflected to enable suturing. • The flap is reflected and rotated to fit the defect. There are chances of ending of the tissue when it is turned to cover the oroantral opening. • The flap is sutured to the buccal flap ensuring a good water tight seal. • The raw surface of the palate is left to granulate only. • A small gauze soaked in Whitehead’s varnish may be placed on that raw surface for a few days.
REFERENCES:
Textbook of Oral & Maxillofacial Surgery, Chitra Chakravarthy (2nd Edition)
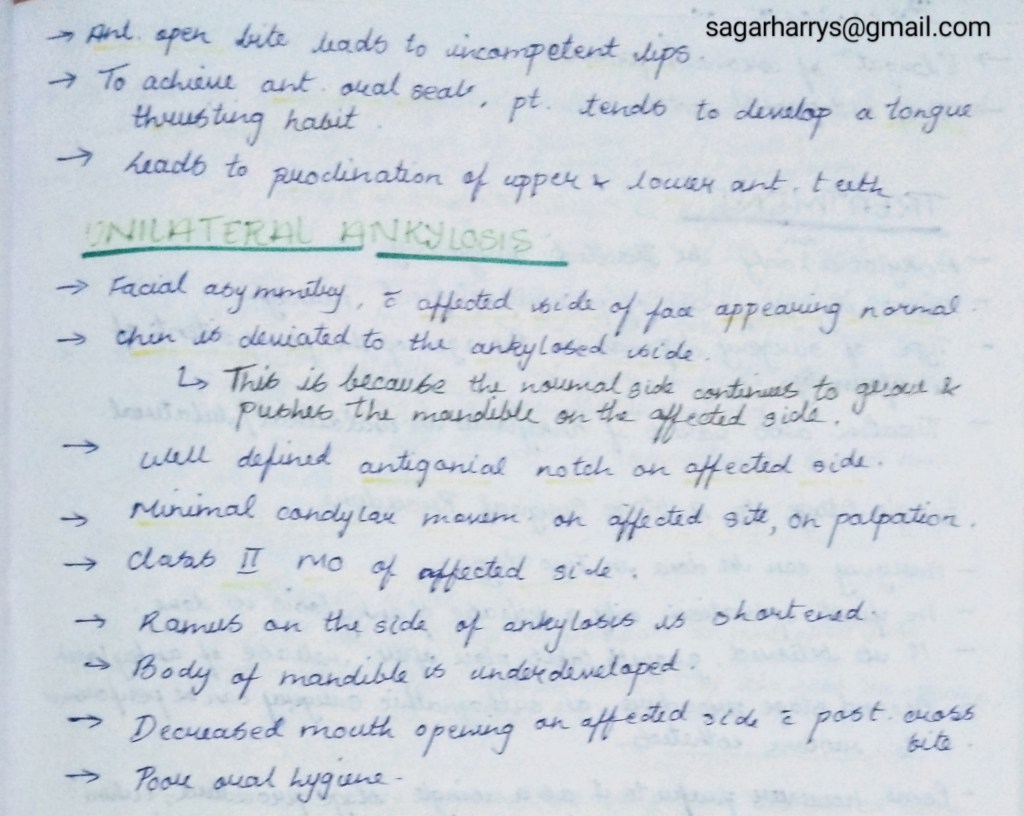
Type of surgery depends on age of the patient & extent of deformity.
Treatment also varies if ankylosis is unilateral/bilateral.
SINGLE STAGE V/S 2-STAGE SURGICAL PROCEDURES:
Surgery can be done in two stages.
In the first operation, only a release of ankylosis is done.
It is believed that growth takes place after release of ankylosis.
Second stage procedure,an orthognathic surgery can be performed to restore esthetics.
Some, however prefer to it as a single stage procedure,where release of ankylosis + esthetic correction is done in a single stage operation in adults.
SURGICAL PROCEDURES:
There are 3 types:
Condylectomy.
Gap Arthroplasty.
Interpositional Arthroplasty.
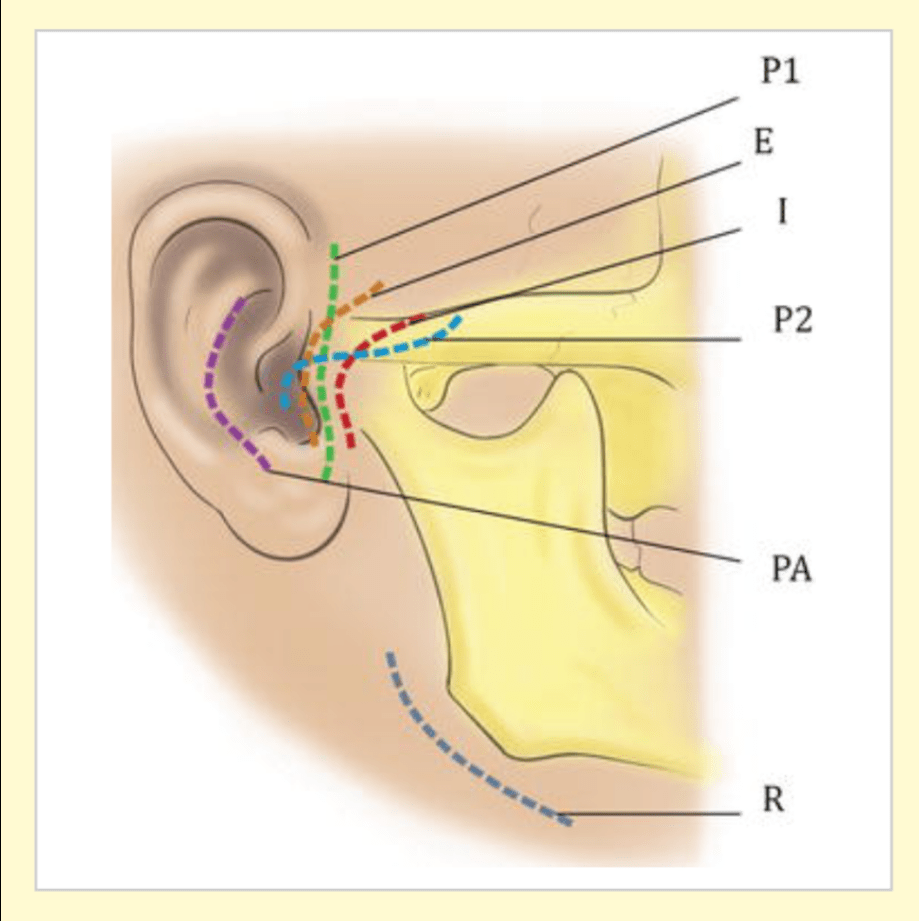
TMJ APPROACHES:
SURGICAL APPROACHES TO THE TMJ: P1 and P2— preauricular approaches; PA-postauricular approach; I—inverted hockey stick approach; E -endaural approach. R-retromandibular approach.
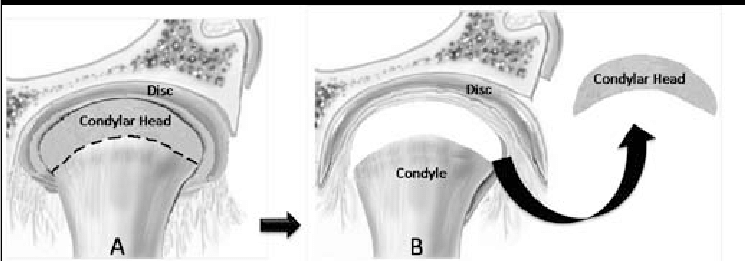
1. CONDYLECTOMY:
CONDYLECTOMY
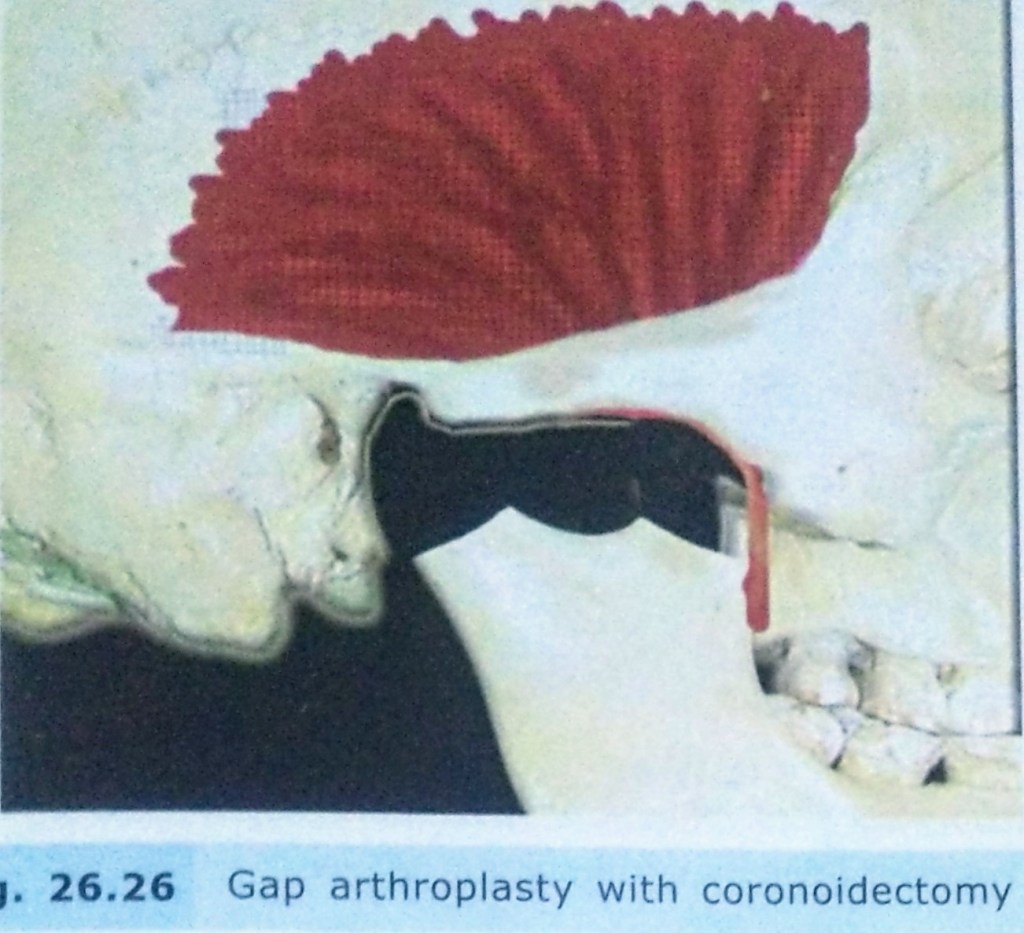
2. GAP ARTHROPLASTY:
GAP ARTHROPLASTY
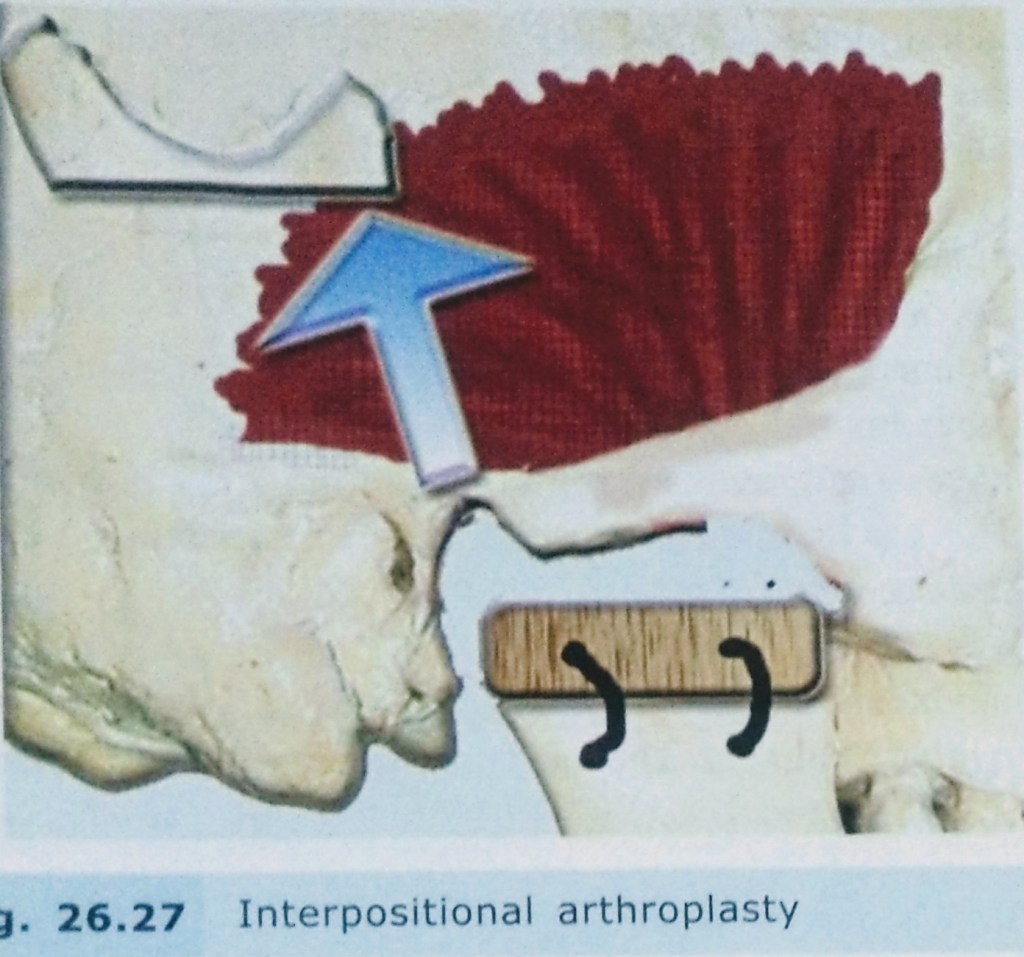
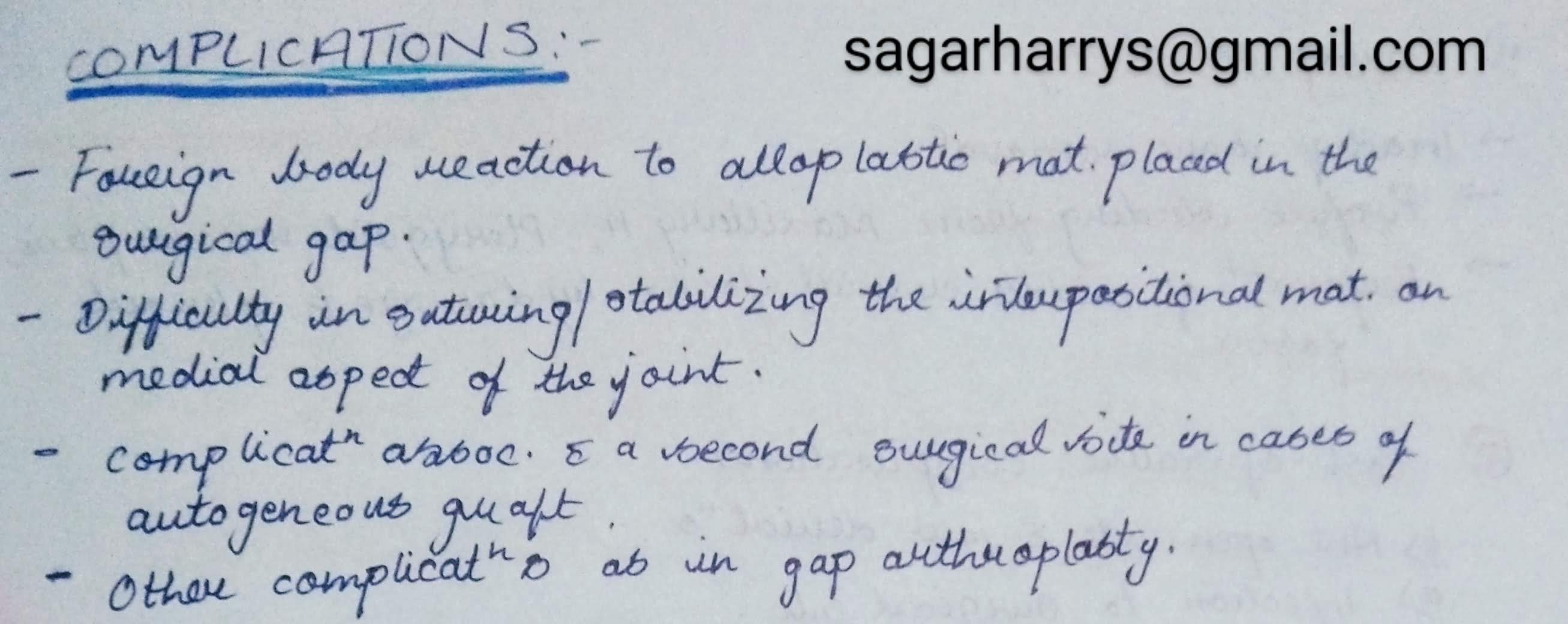
3. INTERPOSITIONAL ARTHROPLASTY:
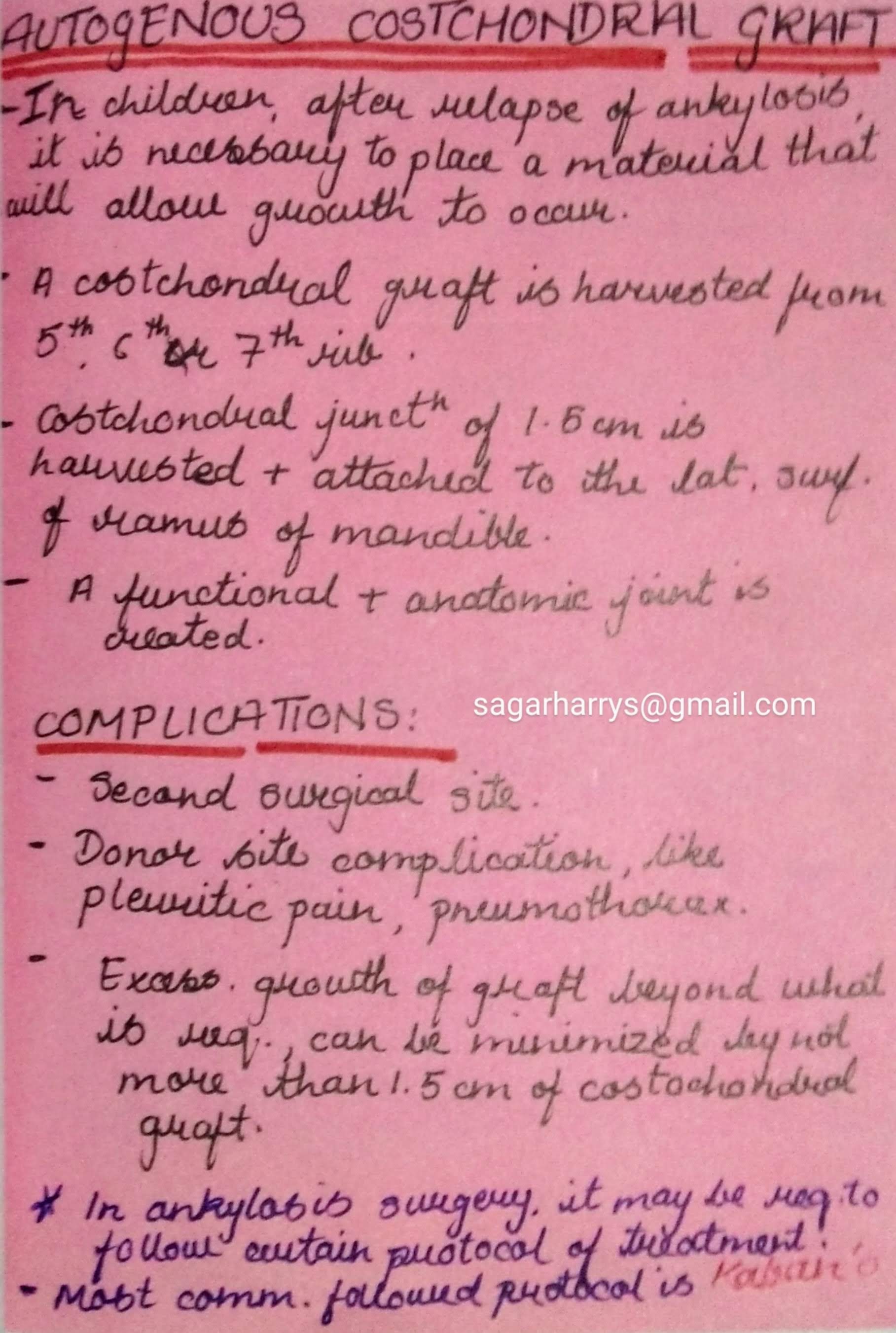
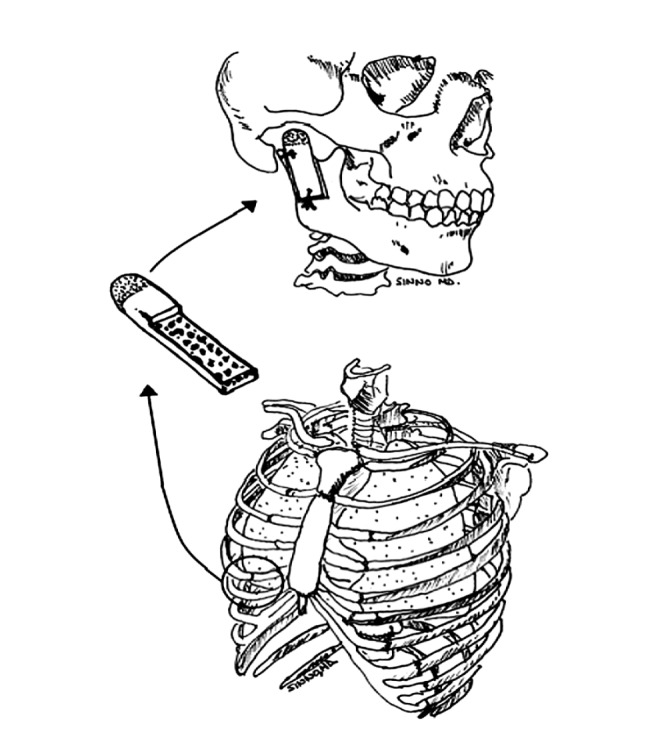
AUTOGENOUS COSTCHONDRAL GRAFT
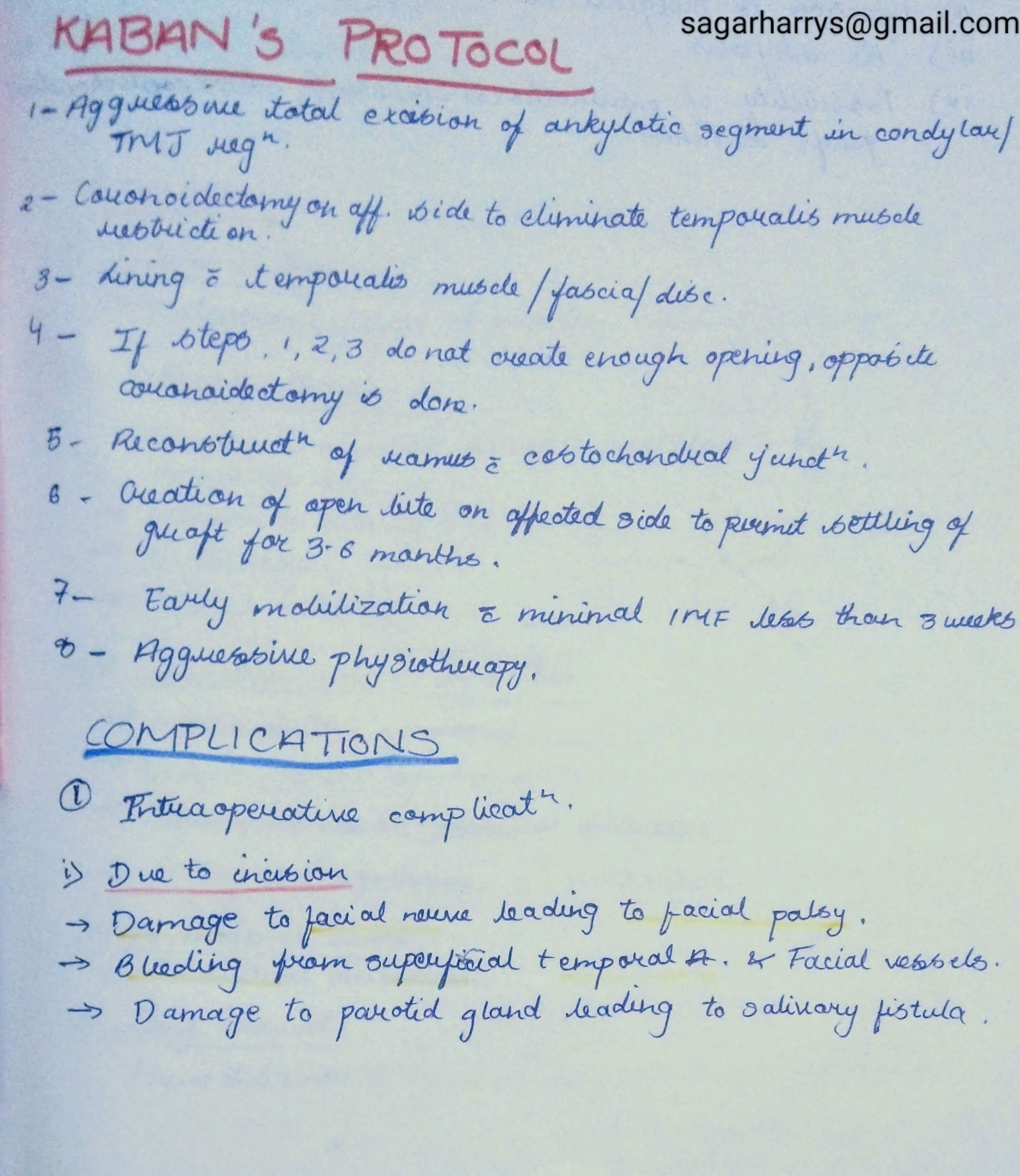
KABAN’S PROTOCOL:
REFERENCES:
Textbook of Oral & Maxillofacial Surgery, Chitra Chakravarthy (2nd Edition)