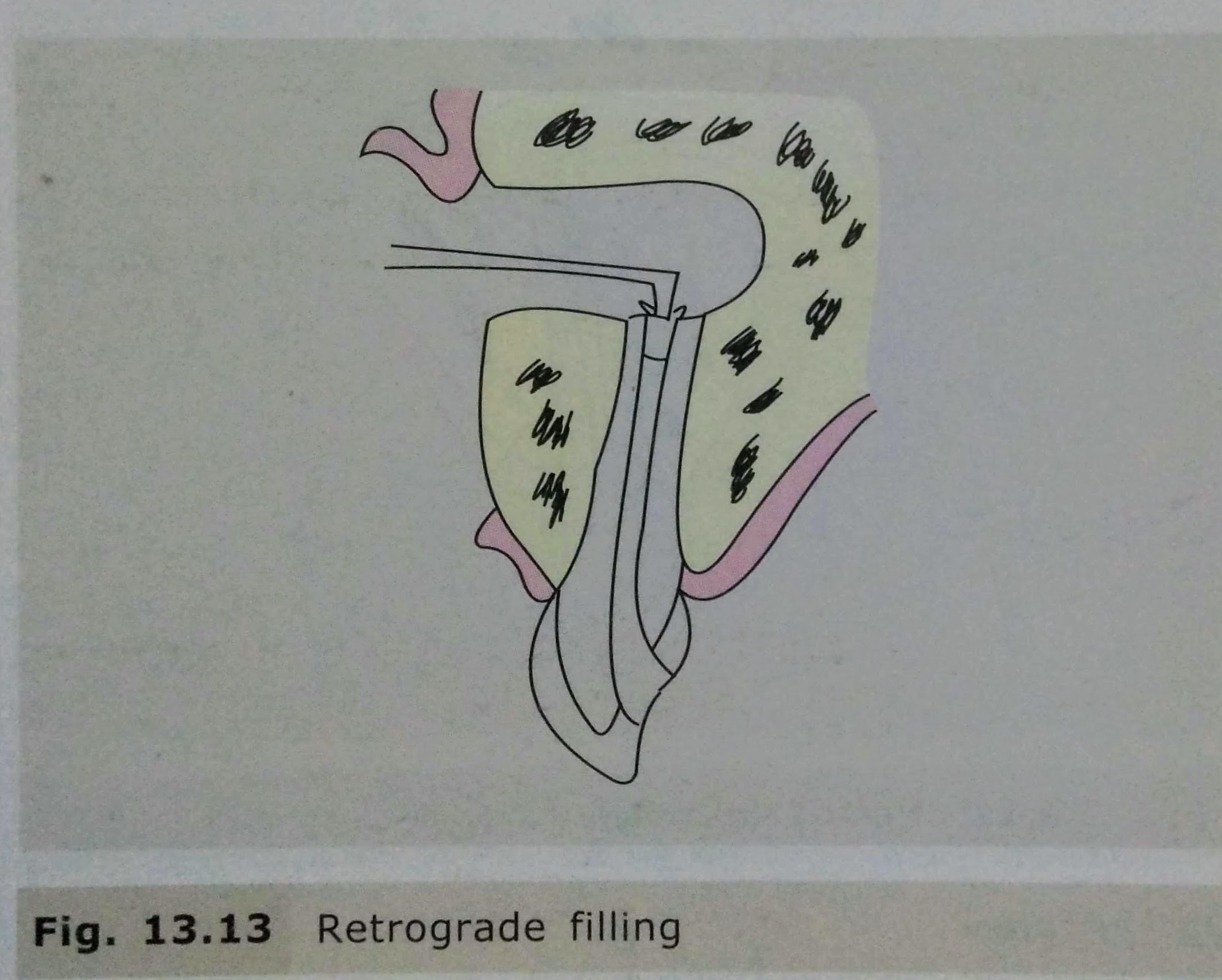
• It is the surgical resection of the apex of the root. • It is the procedure done in case of root canal treatment failure. • If an infection does not subside even after root canal treatment,it may concern enquire a surgical procedure. • In this procedure, the apical region of root is visualised by reflecting a flap and performing an osteotomy.
INDICATIONS : • Aberrant Anatomy: Dilaceration of root apex do not allow endodontic restoration of apex. • Obliteration of apex by secondary dentin. • Iatrogenic repair: A broken endodontic file which cannot be retrieved by conventional means. • Apex perforation. • Improper apical seal which cannot be removed. • Increased drainage of pus from root canal will not allow adequate apical seal. • Open apex. • Non healing periapical granuloma. • Fracture of apical third of root. • Periapical cyst/granuloma.
CONTRAINDICATIONS:
Local Contraindications: • Poor periodontal status of tooth. • Grossly decayed tooth. • Inadequate tooth length. • Acute infection. • Traumatic occlusion. • Uncooperative patients. • Close proximity of root apex to vital anatomic structures such as Maxillary antrum & Nasal floor.
Systemic Contraindications: • Poor medical status of diabetes,Bleeding disorders.etc
STEPS IN ENDODONTIC SURGERY:
Cleaning of the area involved with antiseptic solutions.
Local anaesthesia.
Design of mucoperiosteal flap & reflection of flap.
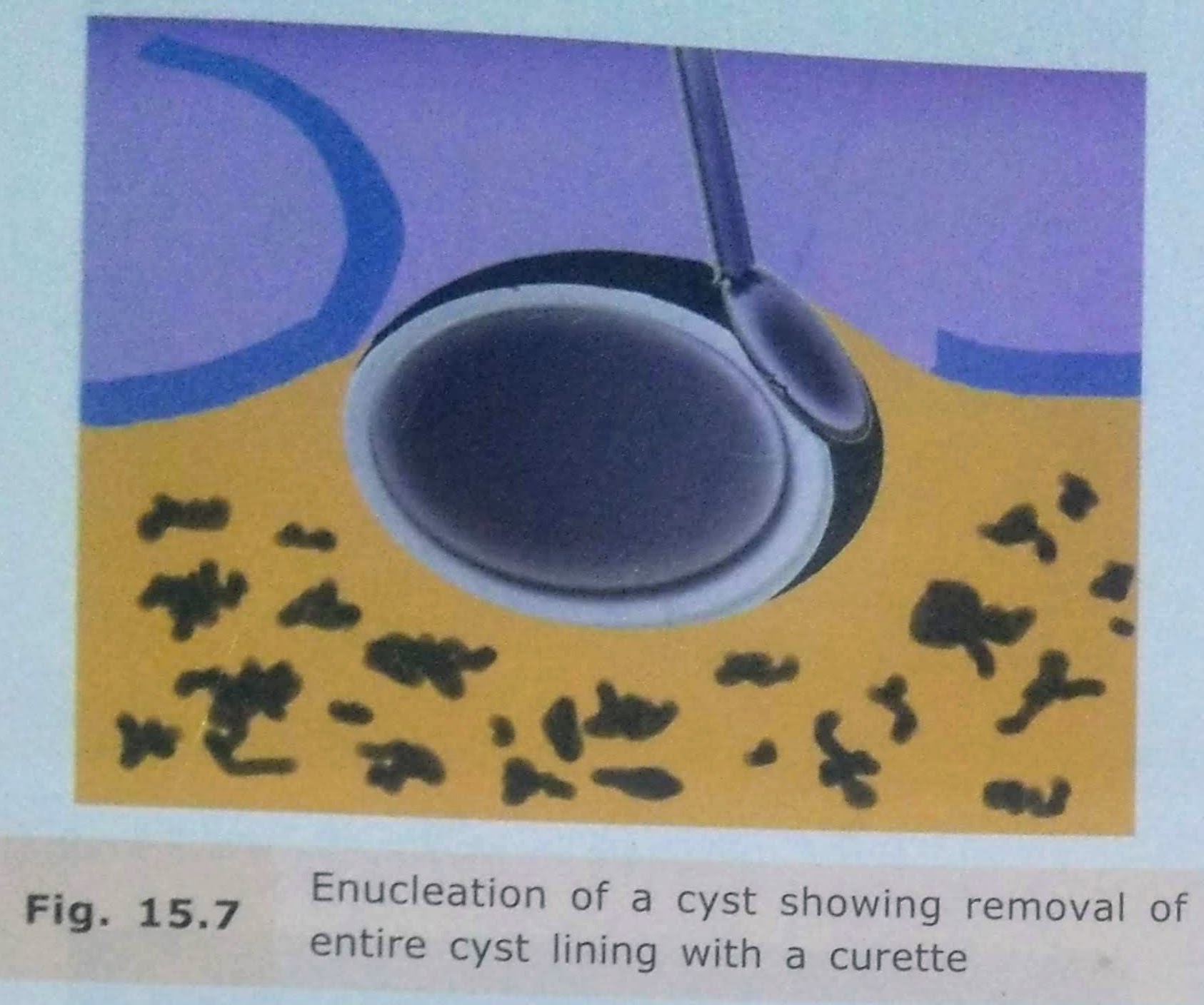
• Also known as PARTSCH II or CYSTECTOMY. • Enucleation is the surgical removal of the entire cystic lining in to-to. By definition, it means shelling out of the entire cystic lining without rupture. This surgical procedure leaves behind a hollow cavity in bone covered by oral mucoperiosteum. This gets filled up with blood clot which eventually organizes to form healthy bone.
INDICATIONS: • Is the treatment of choice for removal of cysts of jaws+ should be employed with any cyst of the jaw, that can be safely removed without sacrificing underlying structure.
ADVANTAGES:
Entire pathological tissue is removed from the lesion.
Tissue available for histopathological examination
Chances of recurrence are less.
Healing time is faster and less appointments for the patient.
Enucleation with primary closure eliminates the repeated appointments for packing medicated gauze irrigation & fabrication of plug.
DISADVANTAGES:
1.Relatively radical procedure.
2.Chances of devitalising the adjacent teeth.
3.Chances of fracture of the jaw.
4.Risk of creation of oroantral/oronasal communication
TECHNIQUES:
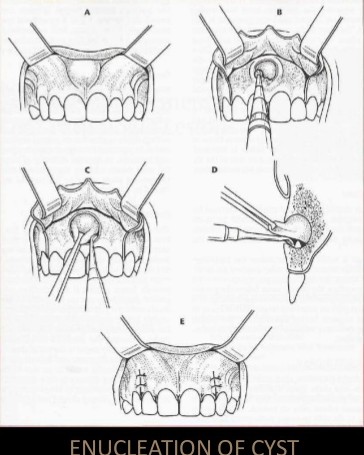
ENUCLEATION OF CYST
Enucleation with Primary Closure: • Small cysts can be removed under local anaesthesia • large cyst should be taken out under general anesthesia, as they are close to vital structures and blood vessels. • After achieving adequate anesthesia, a mucoperiosteal incision is made such that the incision rests on sound bone. • Mucoperiosteal flap is reflected taking care not to perforate rate the cystic lining. • If the bone is perforated by the cyst, the lining will be adherent to the periosteum and will be difficult to reflect it. • The cystic lining is exposed and now carefully teased away from the bone. • It is relatively easy to separate the cystic lining from the bone because there is a layer of fibrous tissue between the two which is easily separabl. • In case of infected cysts or an odontogenic keratocyst. the cystic lining is friable and more difficult to remove entirely. • Every attempt is made to remove the entire cystic lining in a single piece without perforating it. • This ensures complete removal. • After the cyst is removed completely, the cavity in irrigated thoroughly, hemostasis ensured, sharp bone debris are filed and the flap replaced and sutured.
Enucleation with Open Packing : • In case of a large cyst which was previously infected closure may not be possible • After enucleation, the wound is then packed with me impregnated with bismuth iodoform paraffin paste (BIPP) or Whitehead’s varnish.
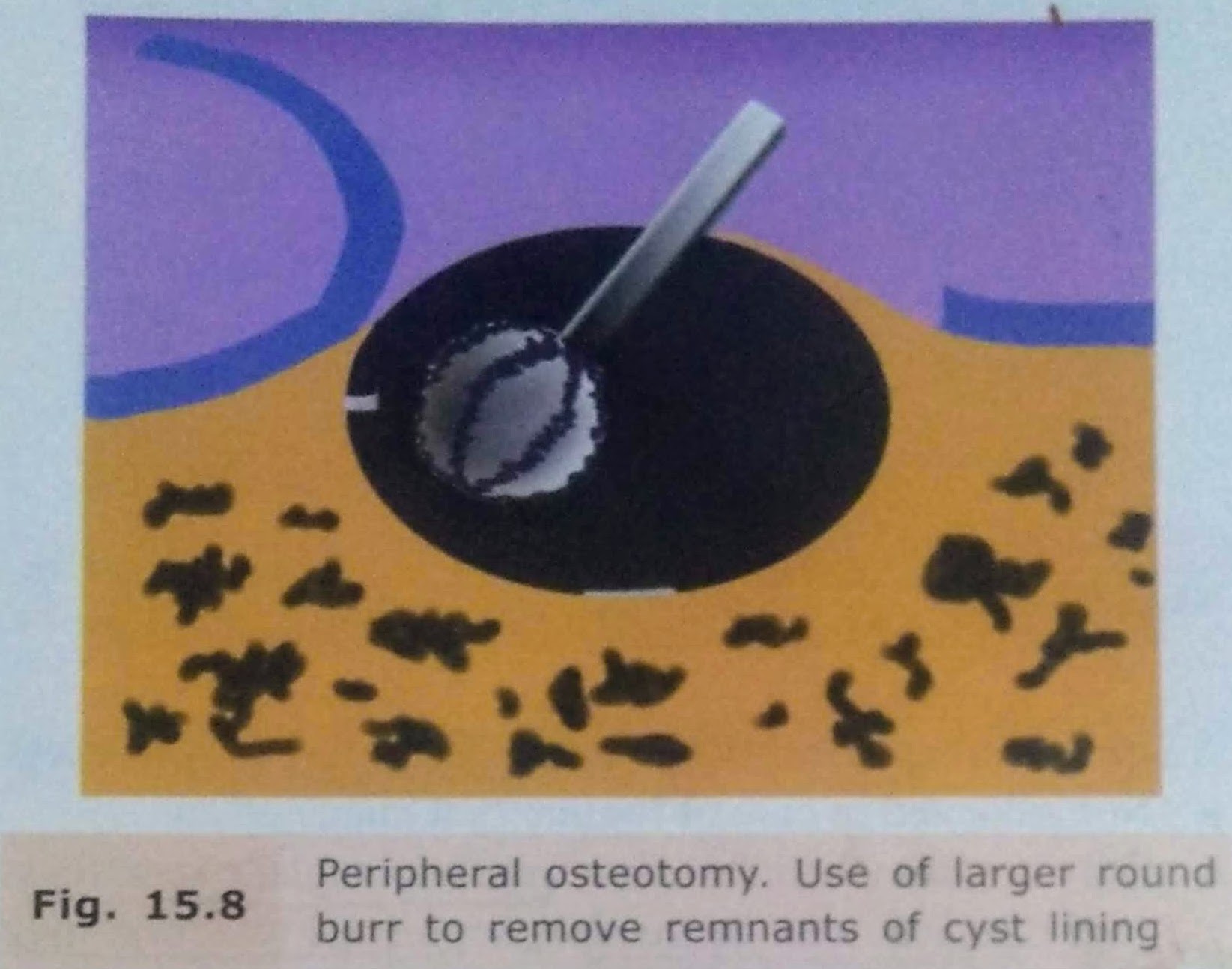
Enucleation with Peripheral Osteotomy:
In this procedure, instead of using a curette, a large round bur may be used to remove around 1-2 mm of bone around the entire periphery of the cystic cavity.
This is done to ensure that any remaining epithelial cells present in the cystic wall or bony cavity are removed.
Enucleation with Bone Curettage: • After enucleation, if there is a doubt that a part of the line has been left behind, it can be curette out. • A bone curette is used to scrape the band remove any remaining lining Enucleation with Peripheral Osteotomy • In this procedure, instead of using a curette, a large round bur may be used to remove around 1-2 mm of bone around the entire periphery of the cystic cavity. • This is done to ensure that any remaining epithelial cells present in the east wall or body cavity are removed.
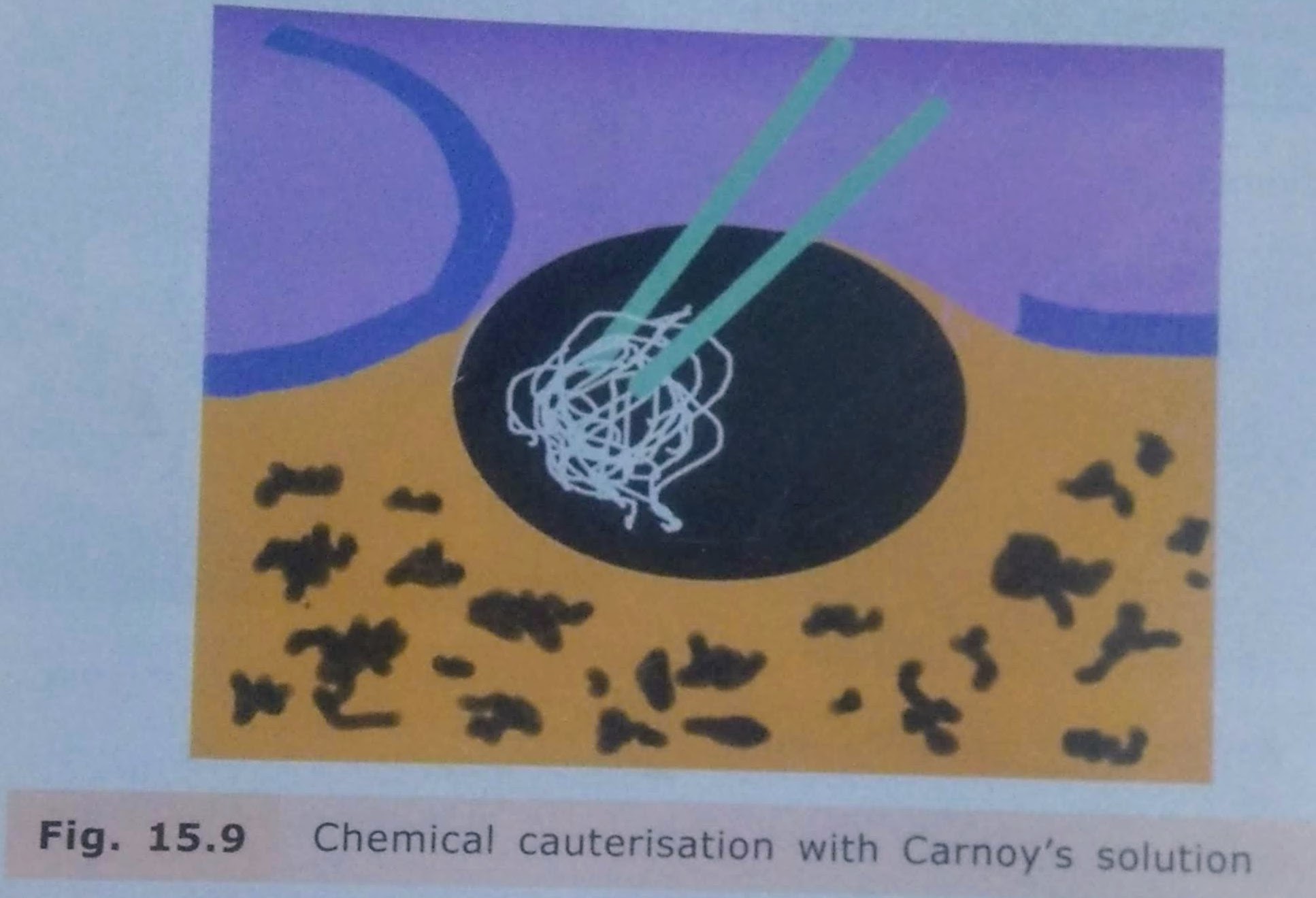
Enucleation with Chemical Cauterisation: • It is indicated mainly in cases of odontogenic keratocyst. • After enucleation, to remove any remaining lining of the cyst chemical cauterising agent Carnoy’s solution is applied along the walls of the cystic cavity. • It is left for about 5-7 minutes and then irrigated thoroughly with saline. • This solution chemically cauterizes any remaining cells of the system.
Enucleation with Bone Grafting • Bone grafting with autogenous cancellous bone grafts can be done in case of large bony defects. • The bone graft obliterates the cavity and stimulates osteogenesis. • There is, however, a risk of wound breakdown and infection of the bone graft which may lead to failure.
COMPLICATIONS: • Risk of bone fracture due to cyst. • Inferior dental nerve involvement. • Management of teeth related to cyst. • Oroantral Communication. • Hematoma formation. • Infection. • Dead Space: At surgical procedure, a hollow dead space is formed. It is usually filled up with blood clot and eventual bone formation. However, there are chances of infection of the clot, breakdown of suture line and pus discharge.
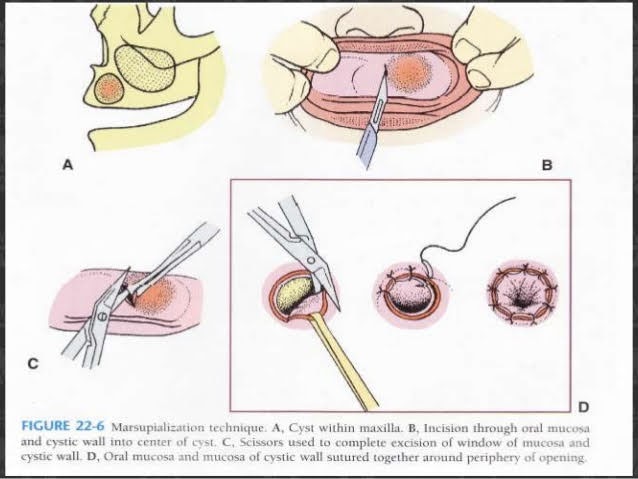
MARSUPIALIZATION: • PARTSCH(1892) described a type of compression procedure for treatment of cyst. • Also k/a PARTSCH I OPERATION & CYSTOTOMY. • In this procedure a window/fenestrations made in the bone and cystic content is evacuated. • The cyst lining is left behind. • Once the cyst contents are evacuated, the intracystic pressure reduces. • Hollow cavity is packed till it gets obliterated by bone over a period of time. • The cystic lining then becomes continuous with normal oral mucosa.
INIDICATIONS: • In extremely large cysts. • Risk of cyst opening into maxillary sinus/nose due to surgical removal of complete lesion. • In very young patients, where it will permit eruption of enclosed tooth,underlying developing tooth. • Patient with poor general condition for allowing minimal surgical procedure. • In cases, where surgical procedures may cause pathological fracture of jaws.
TECHINQUE:
1) Anaesthesia 2) Aspiration 3) Incision: Circular, oval or elliptical. Inverted U Shaped incision with broad base the buccal sulcus. Mucoperiosteum is reflected in this case. 4) Removal of bone 5) Removal of cystic lining specimen 6) Visual examination of residual cystic lining 7) Irrigation 8) Suturing of cystic cavity. • Cystic lining sutured with the edge of oral mucosa. • In Y Shaped incision the mucoperiosteal flap can be turned into cystic cavity covering the margin. • The remaining is sutured to oral mucosa.
9) Packing- Prevents food contamination & covers wound margins. Done with ribbon gauze soaked with WHITEHEAD VARNISH
COMPOSITION • Benzoin – 10g • iodoform-10g • Storax -7.5g Balsam of Tolu -5g • Solvent ether to 100ml Pack removed after 2 weeks. 10) Maintenance of cystic cavity Instruct the patient to clean and irrigate the cavity regularly with oral antiseptic rinse with a disposable syringe. 11) Use of plug: • Prevents contamination, Preserves patency of cyst orifice. • Plug should be stable, retentive and safe design. • Should be made of resilient material (to avoid irritation) like acrylic. 12) Healing: • Cavity may or may not obliterate totally. Depression remains in the process.
ADVANTAGES: • Once the cystic lining is evacuated, there is a tendency of the cystic lining to contract. This stimulates endosteal bone formation. • Marginal ingrowth of normal mucoperiosteum occurs as the cystic lining shrinks. It provides with additional bone regeneration factors. • Not much surgical skill is required. • No risk of oroantral/oronasal fistula. • No damage to adjacent vital structures. • No risk to adjacent vital tooth.
DISADVANTAGES: • Entire pathological tissue is left behind. • High chances of recurrence. • As the bony cavity is large, healing and filling up with normal bone takes longer time. • Use of cyst plug is required with repeated cleansing. • Time consuming & repeated appointment for patients.
REFERENCES:
Textbook of Oral & Maxillofacial Surgery, Chitra Chakravarthy(2nd Edition)
Sources: Textbook of oral and maxillofacial surgery , chitra chakravarthy 2nd edition. Textbook oral and maxillofacial surgery ,SM BALAJI , 3rd.edition
Sources: Textbook or oral and maxillofacial surgery . Chitra chakravarthy 2nd editionx Textbook of oral and maxillofacial surgery , Sm balaji 3rd edition
Sources: textbook or oral And maxillofacial surgery , chitra chakravarthy 2nd edition . Textbook of oral and maxillofacial surgery Sm balaji 3rd edition