Group 1- Cleft of soft palate only Group 2 – Cleft of hard and soft palate extending no further extending than involving incisive foramen, (secondary palate only) Group 3 – Complete unilateral cleft, extending from uvula to incisive foramen in the midline, then deviating the one side and usually extending through the alevolus at the position of the future lateral incisor Group 4- Complete bilateral cleft, extending forward through incisive foramen to alevolus. Premaxilla, suspended from the nasal septum . Asian population have highest frequency often
CLINICAL FEATURES:-
Incidence- 1in 500,With african population the lowest at 1in 250. Cleft lip alone more common in males. Isolated Cleft palate more common in female. 50% are syndromic, and are born with other congenital abnormalities.Cleft lip appear as unilateral / bi lateral. Line of cleft start on lateral part of upper lip and continues through philtrum of alveolus between lateral incisor and canine. When cleft lip continues from incisive foramen through palatal suture middle in palate,cleft lip with palate (unilateral/bilateral) present . . Cleft palate appears with involving soft palate only, involving uvula (bifid uvula),isolated cleft palate also. .Patient have significant physical and physiological effects like, difficulty in eating and drinking with regurgitation of food to nose. . Speech problem . Ear infection: Malposition of Eustachian tubes result in middle ear infection .Cosmetic deformities.
MANAGEMENT
Management of Cleft lip and palate require, multidisciplinary coordinated approach by specialist including maxillofacial surgeon, pediatric surgeon, anesthetist, Prosthodontist, Orthodontist, Speech pathologist, otolaryngology ,audiologist etc..
Management is aimed at closure and correction of lip and palate, secondary correction of palatal fistulae, orthodontic management of malocclusion, Orthognathic surgery, Rhinoplasty,and providing prosthesis for patients.
Pre operative criteria selected by physicians for surgery is Millards Rule of 10’s 1) 10lb weight 2) 10mg/l of haemoglobin 3) 10 weeks of age
SURGICAL MANAGEMENT 1) Primary : Closure of lip & palate 2) Secondary : Closure of palatal fistula, Pharygoplasty ,Bone grafting, orthodontic management Rhinoplasty and Scar revision.
Reference: Oral and Maxillofacial surgery, Balaaji. Textbook of general surgery for dental students, SRB
Cleft palate and Cleft lip comprises the complex of Orofacial clefts . Both comprises congenital malformations affecting oro-facial region. Failure of fusion of nasal and maxillary process leads to cleft of primary palate which can lead to unilateral and bilateral. Cleft of secondary palate is medial, Varies from bifid uvula to complete cleft palate up to incisive foramen.
Etiology:- Clinically, Isolated Cleft palate and Cleft lip with or without Cleft palate has been established.
Factors playing role in Development of Orofacial cleft comprises
1)Heredity (40%of cleft lip and 20% cleft lip appear genetically- single gene/polygenic mutation, Monozygotic twins far likely to get) 2)Nutritional disturbances (experimentally proved in rat fed on abnormal dietary regimen caused cleft palate) mostlty- Riboflavin,Folic Acid Deficiency.
3) Physiologic, Emotional stress, Traumatic also thought to cause 4) Circulating Alcohol ,Drugs ,toxins. 5)Environmental Factors– Teratogens (phenytoin, methotrexate, Corticosteroid, Sodium Valproate) 6)Syndromic Clefting Treacher collins syndrome Pierre Robin Syndrome Stickler syndrome Oro Facial Digital syndrome Trisomy of 13,18 Van Der Voude syndrome ( lip pit syndrome, autosomal dominant , deletion of 1q32 , clinically presenting with cleft lip and palate and medial pits on lower lips on vermillion border.Also include ankyloglossia,high arch palate ,maxillary hypodontia and sygnathia)
EMBRYOGENESIS AND CLEFTING
During sixth and seventh weeks of development upper lips forms when median nasal process merges each each other and fuses with maxillary process of 1st branchial arches. Mid portion of upper lip is derived from median nasal process, lateral derived from maxillary process. Lateral nasal process involved in ala of nose. Primary palate is formed from merging of median nasal process to form intermaxillary segment, which give rises to premaxilla (bone including 4 incisor teeth). Secondary palate make up 90% of palate formed from maxillary process of first branchial arches.Defective fusion of median nasal process with maxillary process forms cleft lip. Failure of palatal shelves to fuse result in cleft palate 45% are Cleft lip with palate 30% Cleft palate alone 25% with isolated cleft lip
Vander Woude syndrome with lower lip pits.Van der Woude Syndome with lip pits , Cleft lip and palate.
Reference:- Textbook of maxillofacial surgery- Balaji. Textbook of embryology- Inderbir Singh. Neville Oral pathology. Images credits : Image 1 – Internet medscape (https://emedicine.medscape.com/article/950823-overview
Anitschkow cell: Modified macrophages with nuclei having caterpillar apperance ( linear bar of chromatin with peripheral radiating chromatins . Found in Recurrent Apthous stomatitis, Iron deficiency Anemia, megaloblastic Anemia, children receiving chemotherapy.
Langerhans cells : Bone marrow derived antigen presenting cells found in epidermis positive for CD1a and Bierbeck Granules. Increased in Langerhans cell histocytosis and decreased in Psoriasis etc.. Named after Paul Langerhans
Tzank Cells: Enlarged , Balooned up degenerating keratinocytes with enlarged vesicular hyperchromatic nucleus, basophilic cytoplasm and diminished nucleoli and perinuclear halo appearance. Named after Arnault Tzank. Found in Herpes Simplex infection, Herpes Zoster, Pemphigus vulgaris, Varicella.
Langhans Giant cells: They are formed by the fusion of epithelioid cells and contain multiple nuclei arranged in a horseshoe-shaped pattern in the cell periphery or are arranged circumferentially. Named after Theodor Langhans. Found in granulomatous lesions like Tuberculosis, tuberculous Leprosy.
Downey cells : Atypical lymphocytes, abundant pale blue cytoplasm and irregular chromatin . Found in infectious mononucleosis. Named after Hal Downey.
Warthin Finkeldy Giant cells : Giant cells with upto 100 nuclei, cytoplasmic and nuclear inclusions. Pathognomic of measels infection. Named after Warthin and Finkeldy.
Reed–Sternberg cells: They are named after Dorothy Reed Mendenhall and Carl Sternberg. They are large cells that either are multinucleated or have a bilobed nucleus (having an “owl’s eye” appearance) with prominent eosinophilic nucleoli.Reed–Sternberg cells are giant cells found in Hodgkin’s lymphoma (HL).
Gaucher Cells : Glucocerebroside laden macrophages containing tubular cytoplasmic inclusions. (Crumbled tissue paper apperance) Hallmark of gaucher disease. Staining positive for Wright and PAS stain.
Rushton bodies : Peculiar linear , curved- hyaline homogeneous structure found in wall of ODONTOGENIC cysts like periapical cyst, dentigerous cyst etc..
Ghost cells: Well defined, eosinophilc, elliptoid fused epithelial cells with blurred apperance. Found in Ghost cell odontogenic tumor, Calcifying epithelial odontogenic cyst, odontoma, craniopharyngioma etc..
Rusells bodies : Large eosinophilc immunoglobulin containing inclusion bodies found in plasma cells. Distented endoplasmic reticulum staining positive for PAS, CD38 etc. Found in chronic inflammations. Aggregate Is called Mott bodies.
Asboe-Hansen sign (also known as indirect Nikolsky sign) refers to the extension of a blister to adjacent unblistered skin when pressure is put on the top of the intact bulla.
Auspitz’s sign is the appearance of punctate bleeding spots when psoriasis scales are scraped off, named after Heinrich Auspitz.This happens because there is thinning of the epidermal layer overlying the tips of the dermal papillae and blood vessels within the papillae are dilated and tortuous, which bleed readily when the scale is removed.
Button-hole sign: Neurofibromatosis. invagination of a nodule when pressed with a finger, a characteristic of neurofibromatosis
Carpet tack lesions: Discoid lupus erythematosus. There are follicular hyperkeratotic plugs causing a carpet tack appearance as they project from the undersurface of the scale when it is removed from advanced lesions.
Charcot’s triad: Seen in multiple sclerosis, characterized by intention tremor, nystagmus, dysarthria
Crowe’s sign: Found in Neurofibromatosis. Presence of axillary freckling in people with neurofibromatosis type I.
Gorlin sign: Ehler -Danlos Syndrome. Ability to touch the tip of the nose with tongue and touch the elbow with the tongue
Higomenakis’s sign: Congenital syphilis. A unilateral enlargement of the sternoclavicular portion of the clavicle, seen in congenital syphilis
Millian sign: Erysipelas. Involvement of the ear (Milian’s ear sign) is a distinguishing feature for erysipelas since this region does not contain deeper dermis tissue.
Nikolsky’s sign: Epidermolysis bullosa, pemphigus, Severe Steven –Johnson syndrome etc. Application of lateral oblique pressure to skin yeild formation of new blisters.
Oil drop sign: Psoriasis. A translucent discolouration in the nail bed that resembles a drop of oil beneath the nail plate.
Reference: Neville Textbook of oral Pathology. Cawsons essential oral pathology Regezi and Batsakis Oral pathology
Rest is necessary for the prompt healing of wounds. Ambulatory patients should be directed to go home & remain quiet for several hours, preferably sitting in a comfortable chair or, if lying down, keeping the head elevated on several pillows.
Only liquids and soft solids should be eaten the first day. They may be warm or cold but not extremely hot.
Food intake should not begin until several hours after surgery to avoid disturbing the blood clot.
If the extractions were limited to one side, chewing can be done on the unoperated side, but when local anesthesia has been used, chewing should be avoided until sensation has returned.
Fluids should be taken in greater amounts than usual to prevent dehydration from limited food intake.
A normal diet should be resumed as soon as possible, since this facilitates healing.
Some degree of postoperative pain accompanies many exodontic procedures and begins after the effects of anesthetic have left. This is considered a normal response to the unavoidable trauma of surgery.
In most cases, such pain lasts no more than 12 to 24 hours, although a traumatic periostitis may persist for several days.
Ordinarily this type of pain can be controlled by the use of cold packs (30 minutes per hour) during the first 24 hours & the proper administration of analgesic drugs.
For mild pain, as after a routine extraction, one of the antipyretic analgesics is usually adequate.
For moderate pain, such as after removal of an impacted tooth, a drug such as codeine or meperidine (Domerol) should be used.
Narcotics are needed only in rare instances.
The combination of a sedative drug with an analgesic agent can also be used but barbiturate alone should never be used to relieve pain as it can result in mental disorientation in a patient suffering from extreme pain.
The degree of swelling that occurs is generally in direct proportion to the degree of surgical trauma.
The application of cold to the operated site helps diminish postoperative swelling. If a rubber ice bag is not available, the ice can be placed in a plastic bag.
Cold can be applied intraorally by holding an ice cube in the mouth.
Pressure dressings can also be beneficial in limiting postoperative swelling.
Once swelling has reached the maximum (usually after 24 to 48 hours), cold is no longer effective, and heat, in the form of moist compresses, should be applied. It too should be used only 30 minutes per hour. The area should be lubricated with petroleum jelly to avoid burning the skin.
Intraoral heat is achieved by the use of hot isotonic saline rinses.
The following fundamental rules apply to every surgical procedure, concerning the incision and flap:
1) The incision must be carried out with a firm, continuous stroke, not interrupted strokes. During the incision, the scalpel should be in constant contact with bone. Repeated strokes at the same place,many times, impair wound healing.
2) Flap design and incision should be carried out in such a way that injury of anatomic structures is avoided, such as: the mental neurovascular bundle, palatal vessels emerging from the greater palatine foramen and incisive foramen, infraorbital nerve, lingual nerve, submandibular duct, parotid duct, hypoglossal venous plexus, buccal artery (of concern when incision of an abscess of the pterygomandibular space is to be performed), facial nerve and facial artery and vein, which are of concern basically for the drainage of abscesses performed with extraoral incisions.
3)Vertical releasing incisions should begin approximately at the buccal vestibule and end at the interdental papillae of the gingiva.
4) Envelope incisions and semilunar incisions, which are used in apicoectomies and removal of root tips, must be at least 0.5 cm from the gingival sulcus.
5) The elliptic incision, which is used for the excision of various soft tissue lesions, comprises two convex incisions joined at an acute angle at each end, while the depth of the incision is such that there is no tension when the wound margins are sutured.
6) The width of the flap must be adequate, so that the operative field is easily accessible, without creating tension and trauma during manipulation.
7) The base of the flap must be broader than the free gingival margin, to ensure adequate blood supply and to promote healing.
8) The flap itself must be larger than the bone deficit so that the flap margins, when sutured, are resting on intact, healthy bone and not over missing or unhealthy bone, thus preventing flap dehiscence and tearing.
9) The mucosa and periosteum must be reflected together. This is achieved (after a deep incision)when the elevator is continuously kept and pressed firmly against the bone.
10) When the incision is not made along the gingival sulcus, for esthetic reasons, and especially in people with broad smiles, the scar that will result must be taken into consideration, particularly on the labial surface of the front teeth.
11) During the surgical procedure, excessive pulling and crushing or folding of the flap must be avoided, because the blood supply is compromised and healing is delayed.
Types of Flaps Various types of flaps have been described in oral surgery, whose name is based mainly upon shape. The basic flap types are: trapezoidal, triangular, envelope, semilunar, flaps created by and incisions, and pedicle flaps.
Trapezoidal Flap The trapezoidal flap is created after an incision, which is formed by a horizontal incision along the gingivae, and two oblique vertical releasing incisions extending to the buccal vestibule. The vertical releasing incisions always extend to the interdental papilla and never to the center of the labial or buccal surface of the tooth. This ensures the integrity of the gingiva proper, because if the incision were to begin at the center of the tooth, contraction after healing would leave the cervical area of the tooth exposed. A satisfactory surgical field is ensured when the incision extends at least one or two teeth on either side of the area of bone removal. The fact that the base of the resulting flap is broader than its free gingival margin ensures the necessary adequate blood supply for the healing process. The trapezoidal flap is suitable for extensive surgical procedures, especially when the triangular flap would not provide adequate access.
Advantages. Provides excellent access, allows surgery to be performed on more than one or two teeth, produces no tension in the tissues, allows easy reapproximation of the flap to its original position and hastens the healing process. Disadvantages. Produces a defect in the attached gingiva (recession of gingiva).
Triangular Flap This flap is the result of an L-shaped incision, with a horizontal incision made along the gingival sulcus and a vertical or oblique incision. The vertical incision begins approximately at the vestibular fold and extends to the interdental papilla of the gingiva. The triangular flap is performed labially or buccally on both jaws and is indicated in the surgical removal of root tips, small cysts, and apicoectomies.
Advantages. Ensures an adequate blood supply, satisfactory visualization, very good stability and reapproximation; it is easily modified with a small releasing incision, or an additional vertical incision, or even lengthening of the horizontal incision. Disadvantages. Limited access to long roots, tension is created when the flap is held with a retractor, and it causes a defect in the attached gingiva.
Envelope Flap This type of flap is the result of an extended horizontal incision along the cervical lines of the teeth. The incision is made in the gingival sulcus and extends along four or five teeth. The tissue connected to the cervical lines of these teeth and the interdental papillae is thus freed. The envelope flap is used for surgery of incisors, premolars and molars, on the labial or buccal and palatal or lingual surface, and is usually indicated when the surgical procedure involves the cervical lines of the teeth labially (or buccally) and palatally (or lingually), apicoectomy (palatal root), removal of impacted teeth, cysts, etc.
Advantages. Avoidance of vertical incision and easy reapproximation to original position. Disadvantages. Difficult reflection (mainly palatally), great tension with a risk of the ends tearing, limited visualization in apicoectomies, limited access, possibility of injury of palatal vessels and nerves, defect of attached gingiva.
Semilunar Flap This flap is the result of a curved incision, which begins just beneath the vestibular fold and has a bowshaped course with the convex part towards the attached gingiva. The lowest point of the incision must be at least 0.5cm from the gingival margin, so that the blood supply is not compromised. Each end of the incision must extend at least one tooth over on each side of the area of bone removal. The semilunar flap is used in apicoectomies and removal of small cysts and root tips.
Advantages. Small incision and easy reflection, no recession of gingivae around the prosthetic restoration, no intervention at the periodontium, easier oral hygiene compared to other types of flaps. Disadvantages. Possibility of the incision being performed right over the bone lesion due to miscalculation, scarring mainly in the anterior area, difficulty of reapproximation and suturing due to absence of specific reference points, limited access and visualization, tendency to tear.
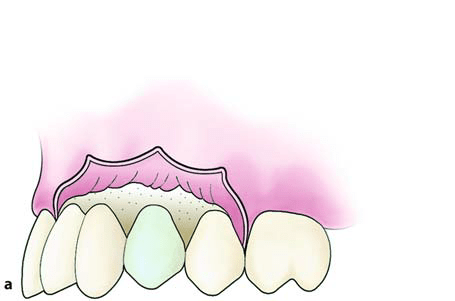
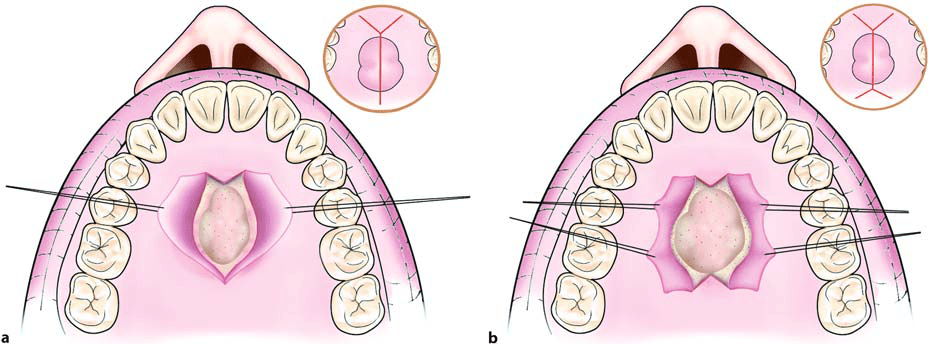
Flap Resulting from Y-shaped Incision.An incision is made along the midline of the palate, as well as two anterolateral incisions, which are anterior to the canines. This type of flap is indicated in surgical procedures involving the removal of small exostoses.
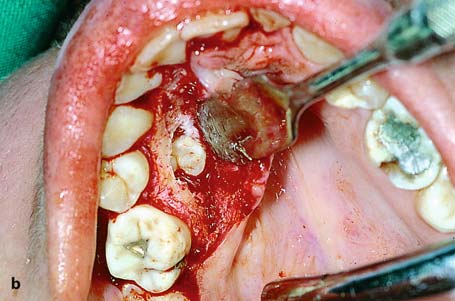
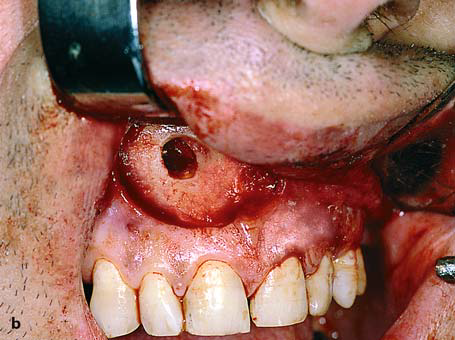
Flap Resulting from X-shaped Incision. This type of flap is used in larger exostoses, and is basically an extension of the -shaped incision. The difference is that two more posterolateral incisions are made, which are necessary for adequate access to the surgical field. This flap is designed such that major branches of the greater palatine artery are not severed.
Pedicle Flaps The three main types of pedicle flaps used for closure of an oroantral communication are: buccal, palatal, and bridge flaps.
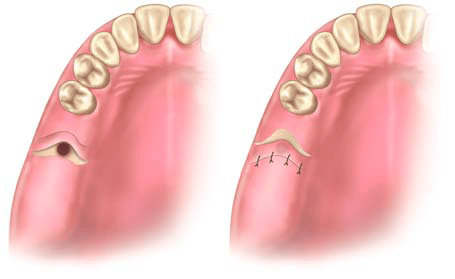
Buccal Flap. This is a typical trapezoidal flap created buccally, corresponding to the area which is to be covered, and is usually used on dentulous patients. It is the result of two oblique incisions that diverge upwards, and extend as far as the tooth socket. After creating the flap, the periosteum is incised transversally, making it more elastic so that it may cover the orifice that results from the tooth extraction. The oblique buccal flap is a variation of the buccal flap. It is the result of an anteroposterior incision, so that its base is perpendicular to the buccal area, posterior to the wound. The flap is rotated about 70°-80° and is placed over the socket. Both cases require that, before placing the flap, the wound margins must be debrided.
Palatal Flap. This type of flap is used in edentulous patients so that the vestibular depth is maintained. The resulting palatal mucoperiosteal flap is rotated posteriorly and buccally, always including the vessels that emerge from the corresponding greater palatine foramen. After rotation, the flap is placed over the orifice of the socket, the wound margins are debrided, and the flap is sutured with the buccal tissues. A gingival dressing is applied for a few days at the void created and healing is achieved by secondary intention.
Pedicle Bridge Flap. This flap is palatobuccal and is perpendicular to the alveolar ridge. After creation, the flap is rotated posteriorly or anteriorly, to cover the orifice of the oroantral communication, without compromising the vestibular fold. This type of flap is used only on edentulous parts of the alveolar ridge.