
Muscles of face bring about different types of facial expressions, hence the name muscles of facial expression, the actions of many of them are implied by their names.

CHARACTERISTICS:
MUSCLES AROUND THE ORIFICE OF EYE
🔹️Orbicularis oculi
Consists of three parts:
It closes the eye tightly during intense sunlight and also for winking.
2. Palpebral part: arises from medial palpebral ligament and sweeps laterally over the upper and lower eyelids to be inserted into lateral palpebral ligament.
It closes the eyelids gently as in sleep or in blinking.
3. Lacrimal part: arises from posterior lacrimal crest and lacrimal fascia and passes laterally in front of tarsal plates of both eyelids to be inserted into lateral palpebral range.
It dilates the lacrimal sac , thus helping in the drainage of lacrimal fluid.
🔹️Corrugator supervision
It arises from medial end of superciliary arch, passes laterally and upwards to be inserted into the skin of eyebrow.
It drags the eyebrow medially and downwards producing vertical wrinkles on the the forehead.
🔹️Frontalis
It elevates the eyebrows and produces transverse wrinkles on the forehead.
🔹️Levator palpebra superioris
It elevates the upper eyelid.
MUSCLES AROUND NASAL CAVITY
🔹️Procerus
Arises from nasal bone, passes upwards to be inserted into the skin of lower part of the forehead.
It produces transverse wrinkles across the bridge of the nose.
🔹️Nasalis
Consists of 2 parts:
It compresses the nasal aperture.
2. Dilator naris: arises from maxilla for the margin of nasal notch and inserted into the lateral part Ala of nose.
Dilates the anterior nasal apertures.
🔹️DEPRESSOR SEPTI
It arises incisive fossa of the maxilla and is inserted into the lower mobile part of the nasal septum.
It fixes the nasal septum to allow dilation of anterior nasal aperture by dilator naris.
MUSCLES AROUND MOUTH
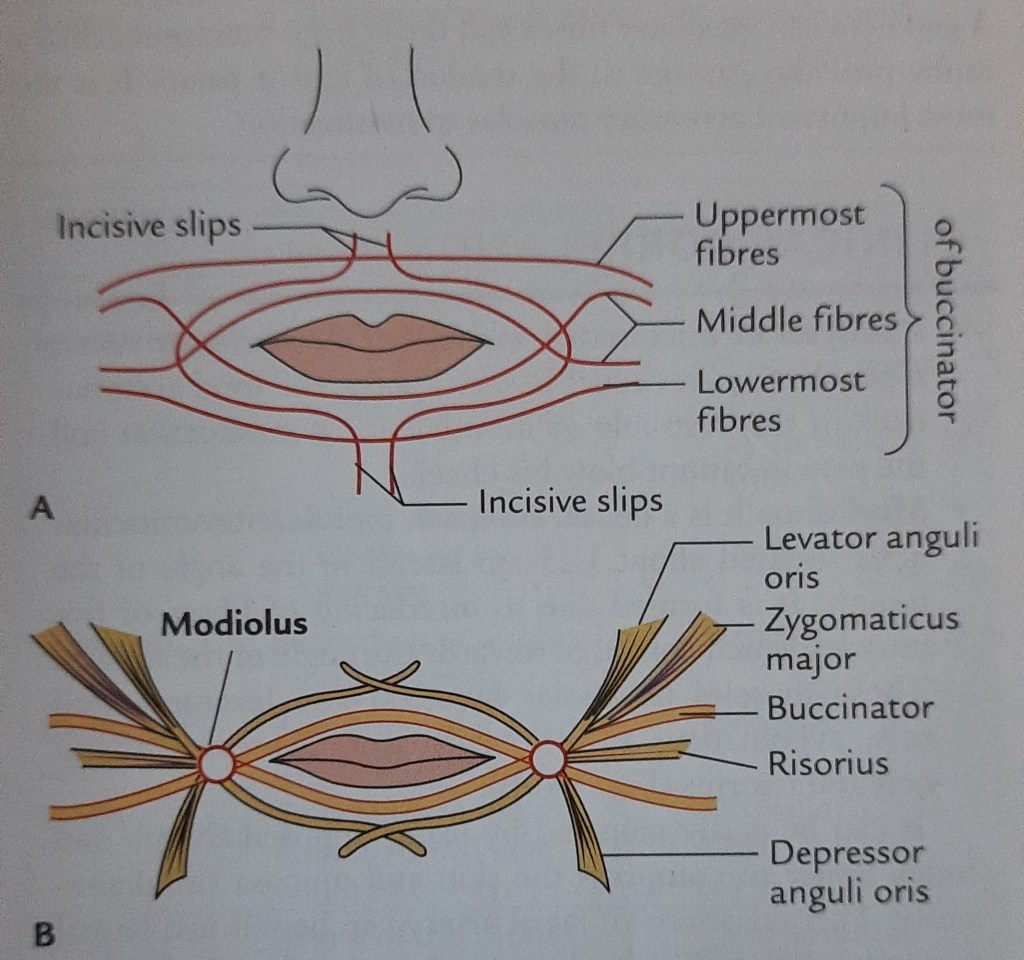
🔹️Orbicularis Oris
It has extrinsic and intrinsic portions. The major extrinsic portion is composed of interlacing fibres of the muscles which converge around the mouth for their insertion into the lips. The fibres of buccinator converge towards modulus and form chiasma.
The intrinsic portion consists of fibres running obliquely between the skin and mucous membranes of lips, incisive slips, which pass laterally into lips and interlace with fibres of peripheral part of orbicularis oris.
🔹️Nine muscles which converge around the mouth
Muscle of chin: Mentalis
Arises from incisive fossa of mandible, inserted into lower lip.
It puckers the chin and protrudes the lower lip.
REFERENCE:
Vishram Singh: Textbook of Anatomy


Anaesthetics – local & genral
….
1.Bupivacaine
Used as
👉 Percutaneous infiltration anaesthesia ,
👉 peripheral nerve block
👉Sympathetic nerve block
,
👉retrobulbar block ,
👉Cadual block
👉Lumbar epidural block
Brand names.
🙏Buloc by celon
Inj – 0.25 % & in 0.5 % ( 20ml )
.
🙏Bupivan by Sun pharma
Inj :- 0.25% (20ml)
0.5% ( 20ml )
0.5% ( 4ml )
.
🙏 Marcain by AHPL
Inj:- 0.5 % ( 20ml )
Inj :- 1 % ( 2ml )
.
👉 used in Induction & maintenance of general anaesthesia
.
🙏Fluothane by AhPL
I:vap :- 100% in ( 200 , 250 , 30, 50 ml ) soln
.
3.Isoflurane
Inhalation anaesthesia
👉 Induction & maintenance of general anaesthesia
.
🙏 Forane by abbott
Inhalant :- 100% in ( 100, 250 ml )
🙏Isorane by AhPL
I:sol :- 5mg/5ml in ( 100,250,30 ml )
.
.
,🙏Ketam by sun
Inj 10mg/ ml (10ml )
Inj 50mg / ml ( 2ml )
.
🙏Ketmin by Themis medicare
Inj 50mg /ml ( 10 ml )
Inj 50 mg/ ml ( 2ml )
.
🙏Ketsia by celon
Inj 100mg ( 2ml )
Inj 500mg ( 10ml )
Abbreviation
I sol :- inhalation solution
Ivap :- inhalation vapour
🙏Gesican 2% gelly by AHPL ( 30ml )
🙏Lidopatch by zydus cadila
T:patch- 5%
🙏Xylocaine by AstraZeneca
T:sol:- 2% 100ml
Oint :- 5% w/w ( 20mg )
Jelly :- 2% w/w ( 30mg )
..
🙏Xylocard 2 % by AstraZeneca
Inj (21.3mg/ml ) 50ml soln
.
🙏 Xylocaine viscous by astra zeneca
T:sol :- 21.3mg/ml ( 100ml )
🙏 Xylocaine topical 4% by AstraZeneca
T:sol :- 42.7mg/ml ( 30ml )
🙏Nummet by icpa
Spy :- 15% w/w ( 100g )
.
Some Combinations
Lidocaine + epinephrine
🙏 Lignosafe by stedman
( Lignocaine hcl 21.3mg & adrenaline 0.0125mg/ml )
Inj in 30ml
🙏 Xylocaine with adrenaline 2% by AstraZeneca
( Lidocaine hcl 21.3mg , adrenaline 0.005mg , nacl 6mg /ml )
Inj 30ml
.
Some other combination
🙏 Xylocaine 5% heavy ( lignocaine hcl 53.3mg/ml , Dextrose 75mg ) inj in 2ml
.
& Xylocaine soln ( same dosage as above ) T:Sol 100ml by AstraZeneca
🙏 Xylocaine spray by AstraZeneca
( Lidocaine hcl 100mg , ethanol 28.29% ) 500ml
.
🙏Xicaine by icpa
( Lignocaine 2 percent , adrenaline 0.022mg) inj 30ml
&
( Lignocaine hcl 2% , adrenaline 0.009 mg ) inj 30ml
.
🙏Asthesia by unichem
( Lidocaine 2.5% w/w , prilocaine 2.5% )
CRM (15,30,5 )g
.
Abbreviation
Crm :- cream
Tsol :- topical solution
































Black hairy tongue is a harmless temporary oral condition. It gives the tongue black and flurry appearance.
This is a condition of defective desquamation of the filiform papillae.
black tongue, lingua villosa nigra.
Usually unknown but below are some of the causes-

Age: occurs at any age
Sex: No gender predilection is seen but seen mostly in males than in females.
Site: dorsal surface and the lateral surface of the tongue.

Elongated filiform papillae with mild hyperkeratosis and occasional inflammatory cells
Debris accumulation among the papillae and candida pseudohyphae may be seen.
Recommended to maintain a good oral hygiene, use of mouth wash, regular brushing