Anterior open bite has always been one of the most challenging malocclusions to treat. Patients often present with esthetic concerns, speech difficulties, and compromised function. While orthognathic surgery is a definitive option for severe skeletal open bites, not all patients are candidates—or willing—for surgery. Fortunately, nonsurgical strategies can offer promising results when case selection is appropriate.
🔍 Understanding the Problem
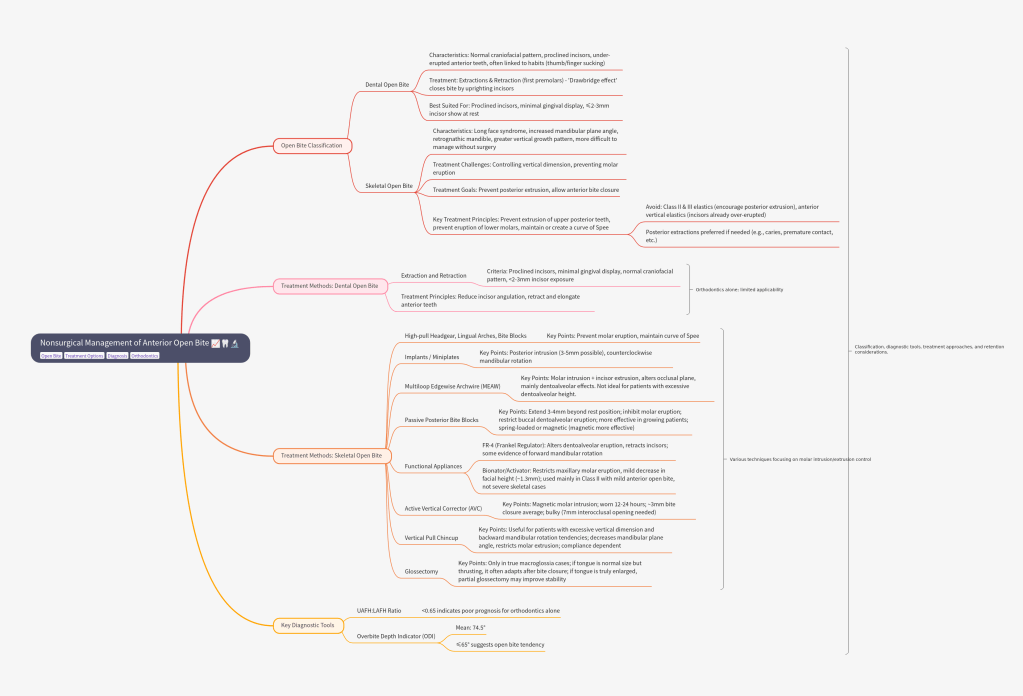
Open bite malocclusion can be dental or skeletal in origin:
Dental open bite: ▸ Normal craniofacial pattern ▸ Proclined incisors, under-erupted anterior teeth ▸ Often linked to habits like thumb/finger sucking
Skeletal open bite: ▸ Long face syndrome, ↑ mandibular plane angle, retrognathic mandible ▸ Greater vertical growth pattern ▸ More difficult to manage without surgery
Key Diagnostic Tools
UAFH : LAFH ratio (<0.65 → poor prognosis for orthodontics)
Extractions & retraction (first premolars) → “drawbridge effect” closes the bite by uprighting incisors.
Best suited for patients with: ✅ Proclined incisors ✅ Minimal gingival display ✅ ≤2–3 mm incisor show at rest
B. Skeletal Open Bite (Nonsurgical Options)
Skeletal open bite is much harder to correct nonsurgically than dental open bite. The central challenge lies in controlling vertical dimension—particularly by preventing or reducing molar eruption.
Posterior extractions preferred if needed (e.g., caries, premature contact, etc.)
👉 Clinical insight: For every 1 mm molar intrusion, you can achieve about 3 mm anterior bite closure through mandibular counterclockwise rotation.
Method
Key Points
High-pull headgear, lingual arches, bite blocks
Prevent molar eruption; maintain curve of Spee.
Implants / Miniplates
Posterior intrusion (3–5 mm possible); counterclockwise mandibular rotation.
Multiloop Edgewise Archwire (MEAW) Multilooped .016 × .022 SS wires + heavy anterior elastics
Molar intrusion + incisor extrusion; alters occlusal plane; mainly dentoalveolar effects. Not ideal in patients with already excessive dentoalveolar height.
Passive Posterior Biteblocks extend 3–4 mm beyond rest position
Inhibit molar eruption; Restrict buccal dentoalveolar eruption → allow mandibular autorotation forward, hence more effective in growing patients; can be spring-loaded or magnetic (more effective; ~3 mm improvement vs 1.3 mm for spring type)
Functional Appliances – Open bite is worsened by faulty orofacial muscle posture.
FR-4 (Frankel regulator): Alters dentoalveolar eruption, retracts incisors. Some evidence of forward mandibular rotation.
Bionator/Activator: Restricts maxillary molar eruption, mild decrease in facial height (~1.3 mm). Used mainly in Class II with mild anterior open bite, not severe skeletal cases.
Active Vertical Corrector (AVC) – using samarium cobalt magnets embedded in acrylic.
Magnetic molar intrusion; worn 12–24 hrs; ~3 mm bite closure avg, bulky (7 mm interocclusal opening needed)
Vertical Pull Chincup
Useful for patients with excessive vertical dimension and backward mandibular rotation tendencies. ↓ mandibular plane angle, restricts molar extrusion; compliance dependent.
Glossectomy
Only in true macroglossia cases. If tongue is normal in size but thrusting, it often adapts after bite closure → surgery not needed. If tongue is truly enlarged relative to oral cavity → partial glossectomy may improve stability.
🔄 The Retention Challenge
One of the biggest hurdles in open bite management is long-term stability.
Studies show relapse rates of 35–43%.
Relapse is often due to dentoalveolar rebound rather than skeletal relapse.
Retention strategies:
Long-term/fixed retainers
Retainers with occlusal coverage to limit molar eruption
🎤 “So here’s the thing — most people pick a career because their parents told them to, or because they panicked after Class 12. But Dr. Akansha Kashyap? Nope. She picked dentistry like it was a love affair between science and art — and guess what? She got the gold medal to prove it. 🏅✨
She’s the kind of dentist who can fix your smile in the morning and sell you a handmade art piece in the evening. Honestly, if she wasn’t drilling cavities, she’d probably be designing album covers. 🎨🦷
In this interview, she spills about: 💡 How to juggle academics without losing your mind (or your hobbies) 🌟 Why mentors + creativity = survival kit in dentistry 🖊️ And a piece of advice so good, you’ll want to embroider it on your scrubs.
So… why are you still here? Go read the full interview — it’s like fluoride for your brain. 🧠💎
Anterior open bite is one of the trickiest malocclusions we deal with in orthodontics. It’s not just about teeth — skeletal, dental, functional, and even habitual factors play a role.
🔹 Traditional Approaches
For decades, open bites in adults were often corrected by:
Extruding anterior teeth orthodontically (which works dentoalveolarly but doesn’t do much for facial esthetics in skeletal cases).
Orthognathic surgery (Le Fort I osteotomy, sometimes two-jaw surgery) to reposition the maxilla.
These surgical approaches improve facial esthetics but come with a catch — relapse.
Denison et al. found a 21% relapse at 1-year post-surgery.
Proffit et al. reported 7–12% overbite reduction within 3 years after Le Fort I surgery.
🔹 The Game Changer: Skeletal Anchorage
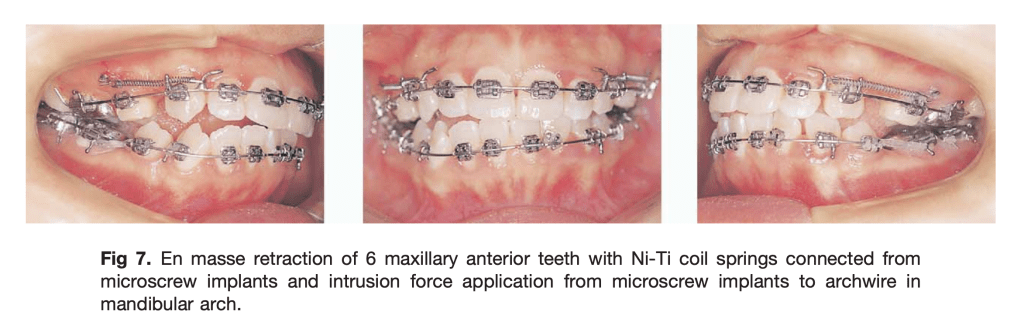
With the introduction of absolute anchorage (miniscrews, miniplates), things got exciting. Now, orthodontists could correct open bites without surgery, by intruding the posterior teeth and letting the mandible autorotate upward and forward.
Kuroda et al.: Skeletal anchorage makes open-bite treatment simpler than surgery.
Sugawara et al.: Used miniplates to intrude mandibular molars; reported ~30% relapse after 1 year.
Lee & Park: Miniscrew intrusion of maxillary molars → only 10.4% relapse in molars and 18.1% relapse in overbite at 1 year.
🛠️ How Was Intrusion Done?
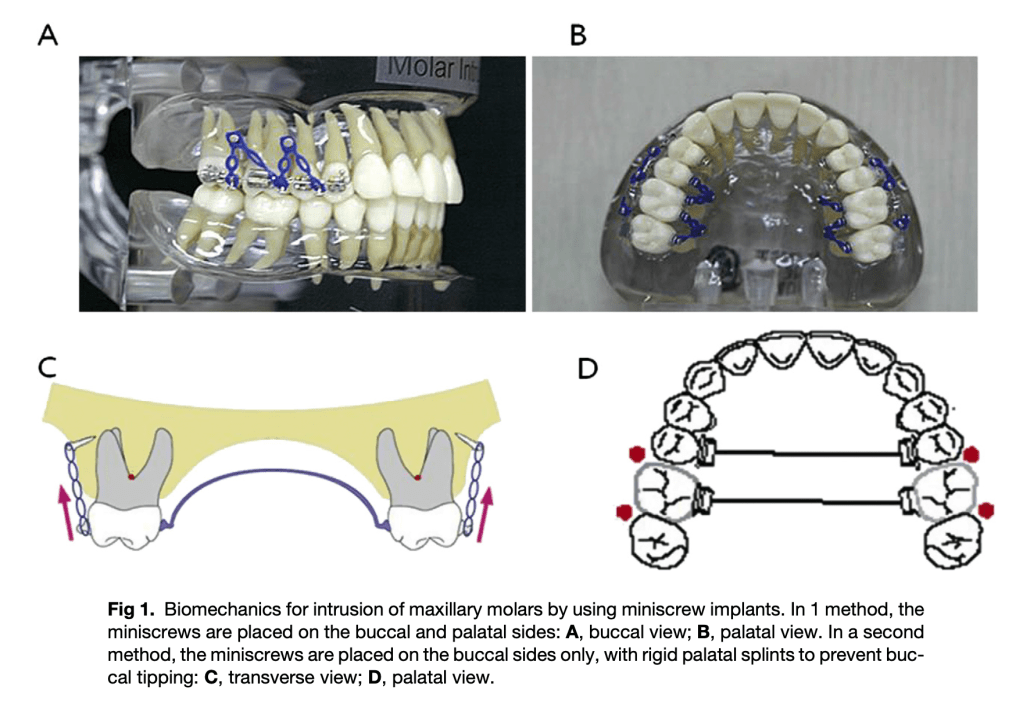
Two different miniscrew protocols were used:
1️⃣ Buccal + Palatal Screws
Screws placed between roots of 2nd premolar–1st molar and 1st–2nd molar.
Intrusive force applied with elastomeric chains after 1–2 weeks.
2️⃣ Buccal Screws Only
Screws placed on buccal side at the same sites.
Rigid transpalatal arch (TPA) added to prevent buccal tipping.
Interpretation: It’s not just teeth—it’s also muscles & soft tissue adaptation trying to return to “old balance.”
🔹 Role of Retention & Soft Tissue
Tongue posture, perioral muscles, and habits play a huge role.
Myofunctional therapy after treatment improves stability.
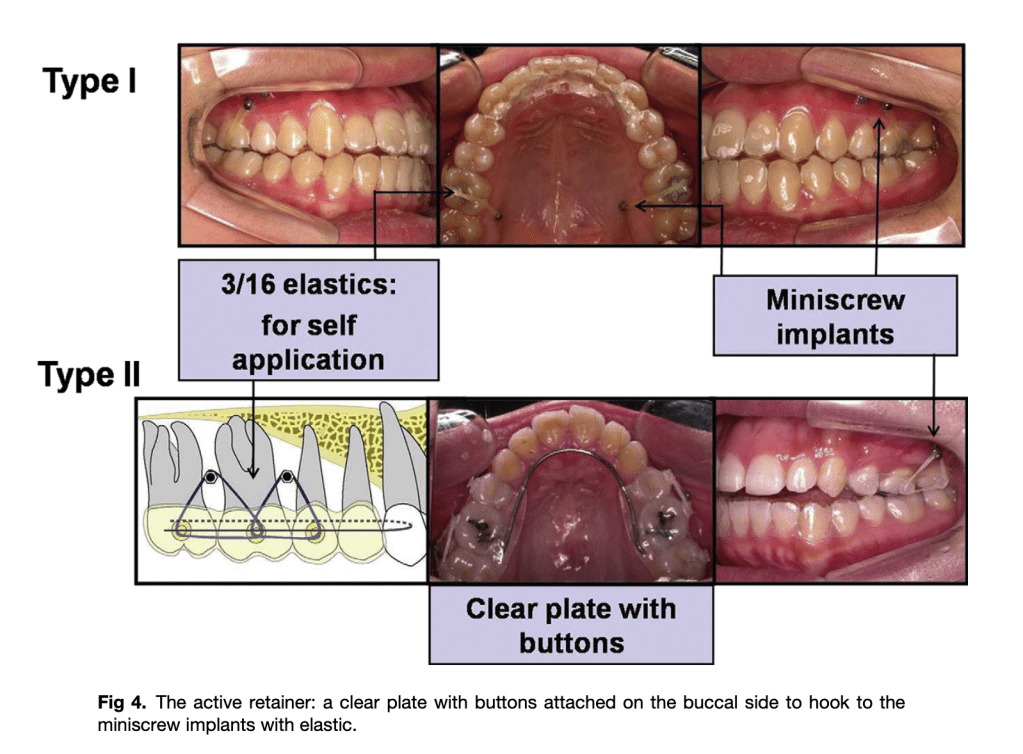
Standard retainers (lingual + circumferential) aren’t enough for intruded molars — because intrusion is inherently less stable than tipping or mesiodistal movement.
Authors suggest an “active retainer”: clear retainer with buccal buttons that can be hooked to miniscrews with elastics to hold molars in place.
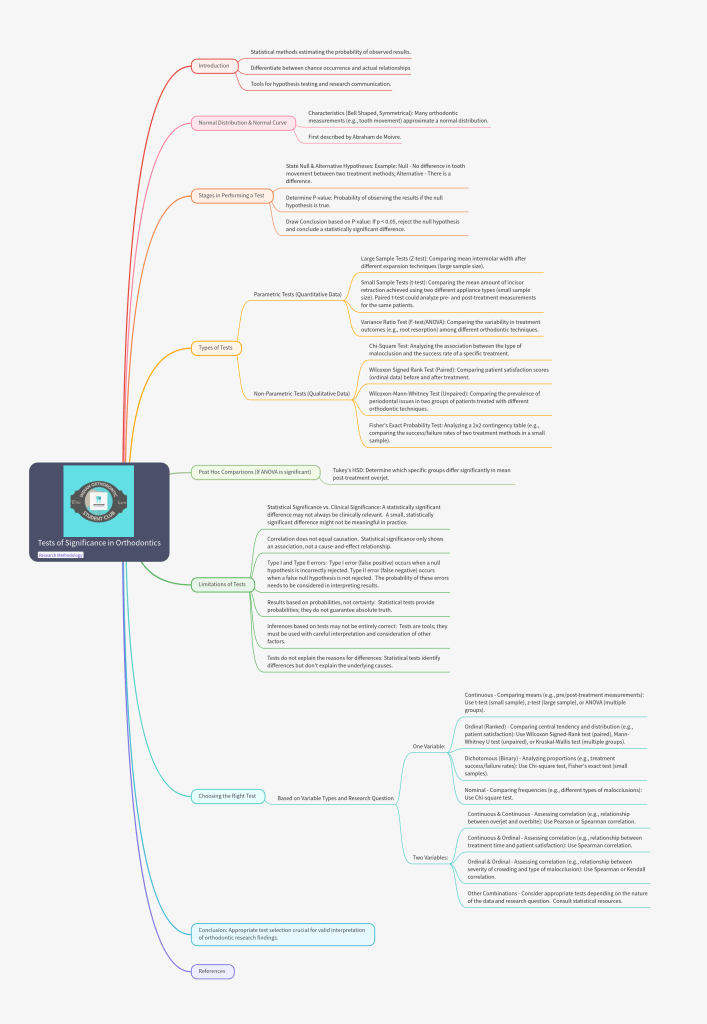
Unlock the complexities of statistical analysis in clinical research with our detailed “Tests of Significance” mindmap! This structured visual guide distills everything you need to know about parametric and non-parametric tests, normal distribution, step-by-step procedures, and the essential criteria for choosing the right test.
In this issue, Oral Pathologist Dr. Shivani Bhandari opens up about her inspiring path—from the first spark of ambition in her school days to navigating academic pressure, personal loss, and carving her own niche in the dental world.
💡 You’ll find:
Honest stories of resilience and motivation when life tests you the hardest.
Practical advice on balancing studies, hobbies, and responsibilities.
A refreshing reminder that dentistry is more than a profession—it’s a platform to innovate, teach, create, and inspire.
If you’re a dental student or young professional, this magazine isn’t just for reading—it’s for redefining what your future could look like.
👉 Dive in. Get inspired. Start shaping your own unique path in dentistry.
Managing skeletal anterior open bite (AOB) is one of the trickiest problems you’ll see in clinic. Decisions about which teeth to extract — or whether to extract at all — can change the vertical facial pattern, molar position, and ultimately whether the mandible rotates closed (helpful) or stays/re-rotates open (problematic). Understanding how extraction pattern, tooth movement, and growth stage interact helps you plan smarter treatments and set realistic expectations.
The study in one line
A prospective cephalometric study compared vertical/rotational changes in AOB patients treated with three extraction patterns: first premolars (E4), second premolars (E5), and first molars (E6) — and found that extraction choice (plus how posterior teeth move) influenced mandibular rotation.
1. Extraction Choice & Mandibular Rotation
Extraction Pattern
Skeletal Open Bite Involvement
Effect on Mandibular Rotation
1st Premolars (E4)
Anterior teeth only
No significant rotation.
2nd Premolars (E5)
Extends to posterior teeth
Closing rotation
1st Molars (E6)
Extends to posterior teeth
Greatest closing rotation
The logic behind those findings comes down to three biomechanical factors:
Where the extraction space is (anterior vs. posterior in the arch)
How molars move to close that space (translation vs. extrusion)
How that movement interacts with mandibular rotation mechanics
The more teeth you move forward, the harder it is to prevent some extrusion of molars during protraction (especially without TADs or intrusion mechanics).
This shorter movement path makes vertical control easier — fewer teeth to drag along, less tendency for extrusion.
Reduced extrusion allows the posterior occlusal contacts to move out of the “palatomandibular wedge” and encourages mandibular closing rotation (SN–GoGn, SGn–NBa decrease).
E6: Large forward movement of molars with minimal extrusion → maximum rotation.
Posterior occlusal “block” is eliminated quickly, and molars protract mostly horizontally rather than extruding.
With posterior teeth moving forward and out of the wedge, the mandible is free to rotate up and forward the most.
3. Cephalometric Change Patterns
Variable
E4
E5
E6
SN–GoGn
↔ (no change)
↓
↓↓ (largest decrease)
SGn–NBa
↔
↑
↑↑
ANS–Me / Na–Me
↑↑ (largest increase)
↑
↑ (smallest)
Upper Molar–Palatal Plane
↑↑
↑
↑
Lower Molar–Mand. Plane
↑↑ (largest)
↑
↑
4. Clinical Tips
For AOB limited to anterior teeth: First premolar extraction may not help rotation—consider vertical control strategies.
Use gable bends, TADs for anchorage/vertical control, intrusion mechanics if needed.
Avoid mechanics or auxiliaries that encourage molar extrusion during space closure.
For AOB involving posterior teeth: Second premolar or first molar extraction preferred to facilitate mandibular closing rotation.
Minimize posterior tooth extrusion during protraction to enhance rotation.
Treat after peak pubertal growth spurt – less natural extrusion tendency — greater chance of controlled molar protraction and closing rotation.
5. Pearls for exams & case presentations
When presenting a case, include: vertical pattern, extent of AOB, growth indicators (hand–wrist/CS stage), extraction rationale, and how you’ll control vertical molar movement.
Don’t equate “extraction = guaranteed closing rotation.” The pattern of tooth movement (extrusion vs. translation) and growth stage are decisive.
When a maxillary lateral incisor is missing, substituting the canine into its place can produce excellent esthetic and functional results — but only if torque control is done right. One of the most common errors? Inadequate palatal root torque in the relocated canine.
Why Torque Matters
The canine crown is bulkier, and without enough palatal root torque, its prominence can disrupt smile esthetics and compromise occlusion. The right bracket choice helps counteract this.
Bracket Options & Prescriptions (MBT*)
Bracket Choice
Torque / Tip
Key Advantages
Notes
Maxillary Central Incisor
+17° torque / 4° tip
Maximum palatal root torque
Enameloplasty needed; add up to +4° distal root tip
Maxillary Lateral Incisor
+10° torque / 8° tip
Good torque & tip control; easy placement
Enameloplasty needed
Flipped Maxillary Canine
+7° torque / 8° tip
Torque & tip control without reshaping
May not give enough torque
Flipped Mandibular 2nd Premolar
+17° torque / 2° tip
Max torque without enameloplasty
Remove bracket posts after bonding
*Modified for Roth or Damon prescriptions if needed.
Torque Tips
“1 to 5 Rule”: Every .001″ slot–wire play ≈ 5° torque loss
.017″×.025″ in .018″ slot → 5° loss
.019″×.025″ in .022″ slot → 10–15° loss
This is why an .018 slot system with .017×.025 wire tends to have better torque control than a .022 slot with .019×.025 wire, assuming same bracket prescription.
If you want to minimize torque loss, you either:
Use the largest possible wire for that slot
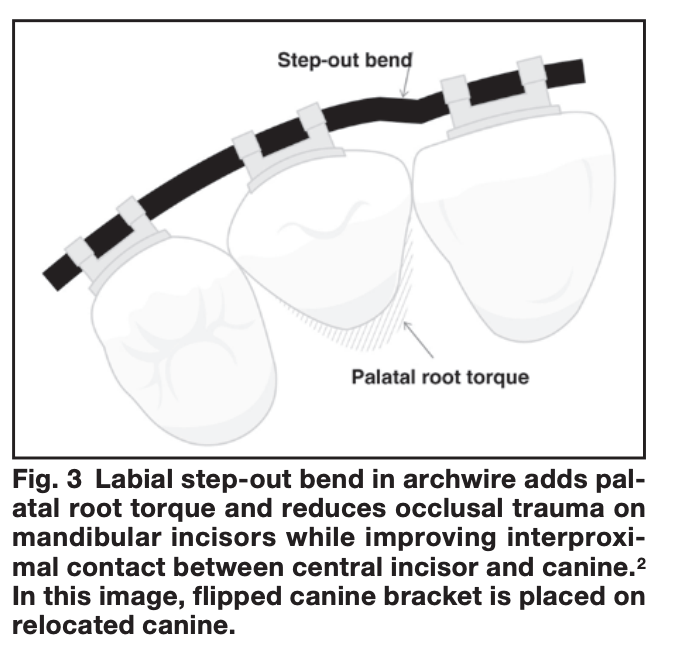
Or add auxiliary torque (e.g., torquing springs, step-out bends)
Labial step-out bends shift the canine root palatally, improving torque and interproximal contact while minimizing occlusal interference.
Example 1: .017″ × .025″ wire in a .018″ slot
Slot height = 0.018″
Wire height = 0.017″
Difference (play) = 0.001″
Torque loss = 0.001″ × 5° = ≈ 5° loss
So even with a nearly full-size wire, you can’t get 100% torque expression — there’s some rotational freedom before the wire contacts the slot walls.
Example 2: .019″ × .025″ wire in a .022″ slot
Slot height = 0.022″
Wire height = 0.019″
Difference (play) = 0.003″
Torque loss = 0.003″ × 5° = ≈ 15° loss
Why the guide says 10–15° instead of exactly 15°:
Theoretical loss = 15° (from math)
In practice, clinical torque loss is often slightly less because:
Residual tip in the tooth means the wire contacts sooner than expected
Manufacturing tolerances (slots often oversized, wires slightly undersized or rounded)
The wire may seat differently under ligation forces
Other Factors Influencing Torque
Archwire material (SS > TMA > NiTi for high torque)
Bracket material
Type of ligation
Interbracket distance
Tooth morphology & biology
Clinical Pearls
Delay enameloplasty if unsure → choose flipped mandibular 2nd premolar for torque & base fit.
Canine extrusion improves gingival architecture but monitor occlusion.
For high torque (>24°), beta titanium is safer than SS for bends.
Beta titanium offers a balance between torque delivery and flexibility, making it preferable for large bends compared to the stiffness of stainless steel.