Nancy 13th edition
Nancy 13th edition
Teething is a term limited by common usage to eruption
of primary dentition. Since the time of Hippocrates (460-
377 BC) teething is blamed for ailments such as fever, convulsions, bronchitis, otitis media and diarrhea, for
causing 12% of the deaths in children under four years.
Complete opposite views are also available. It is seen
that these local and systemic factors are associated with
the disease somewhere else also and just as a coinci-
dence appear with teething.
Eruption of primary dentition usually begins in the 4-6th month of a child’s life. The appearance of normal teeth is eagerly awaited by the parents since it represents an important early milestone in development. In most cases eruption of teeth causes no distress to the child or parents, but sometimes the process causes local
irritation, which is usually minor but which may be severe enough to interfere with the child’s sleep.
CLINICAL FEATURES OF TEETHING
LOCAL SIGNS
1. Hyperemia or swelling of the mucosa overlying theerupting teeth.
2. Patches of erythema on the cheeks.
3. Flushing may also occur in the skin of the adjacen cheek.
SYSTEMIC SIGNS
1.General irritability and crying
2.Loss of appetit.
3.Sleeplessness
4.Increased salivation and drooling
5.Insanity
6.Meningitis
7.Increased thirst
8.Circumoral rash
9.Cough
Associated Problems
Systemic
Fever,convsions, diarrhea,vomiting, bronchitis, cholera, tetanus
Local
Eruption hematoma, eruption sequestrum, ectopic eruption, transmigration , transposition
MANAGEMENT
PREVENTIVE MEASURES
1. Maintain child’s oral and general body health.
2.Gums should be wiped after each meal with cotton soaked in a weak antiseptic.
3. Adequate quantities of vitamins, minerals , proteins, are given to the child for increasing body’s resistance .
GENERAL MANAGEMENT
1. Hard , non sweetened rusks
2. Use of toasted bread helps in providing gingival stimulation.
3. Use of hard fruits such as appleor guava .
MEDICAL MANAGEMENT
demulcent and mild antiseptic.
1. Topical application of glycerin: It acts as a protective demulcent and mild antiseptic.
2. Topical application of lignocaine hydrochloride which provide relief in the interval before the analgesic is effective .
3. Topical application of benzyl alcohol can also be effective.
SURGICAL MANAGEMENT
Surgical treatment is sometimes recommended for the relief of pain from an eruption cyst or a hematoma. The technique advocates is to make 2 semilinar incisions over the crowns of the tooth , which meet at their extremities. The intervening portion of the tissue , which lies over the occlusal surface of unerupted tooth is then removed with a pair of tissue foreceps.
REFERENCES:TEXTBOOK OF PEDODONTICS SHOBHA TANDON 2ND EDITION



References – Shafer’s oral pathology , SN Chugh – Textbook of clinical medicine for dental students , osmosis.org


source – Nancy 13th edition

source – Nancy 13th edition
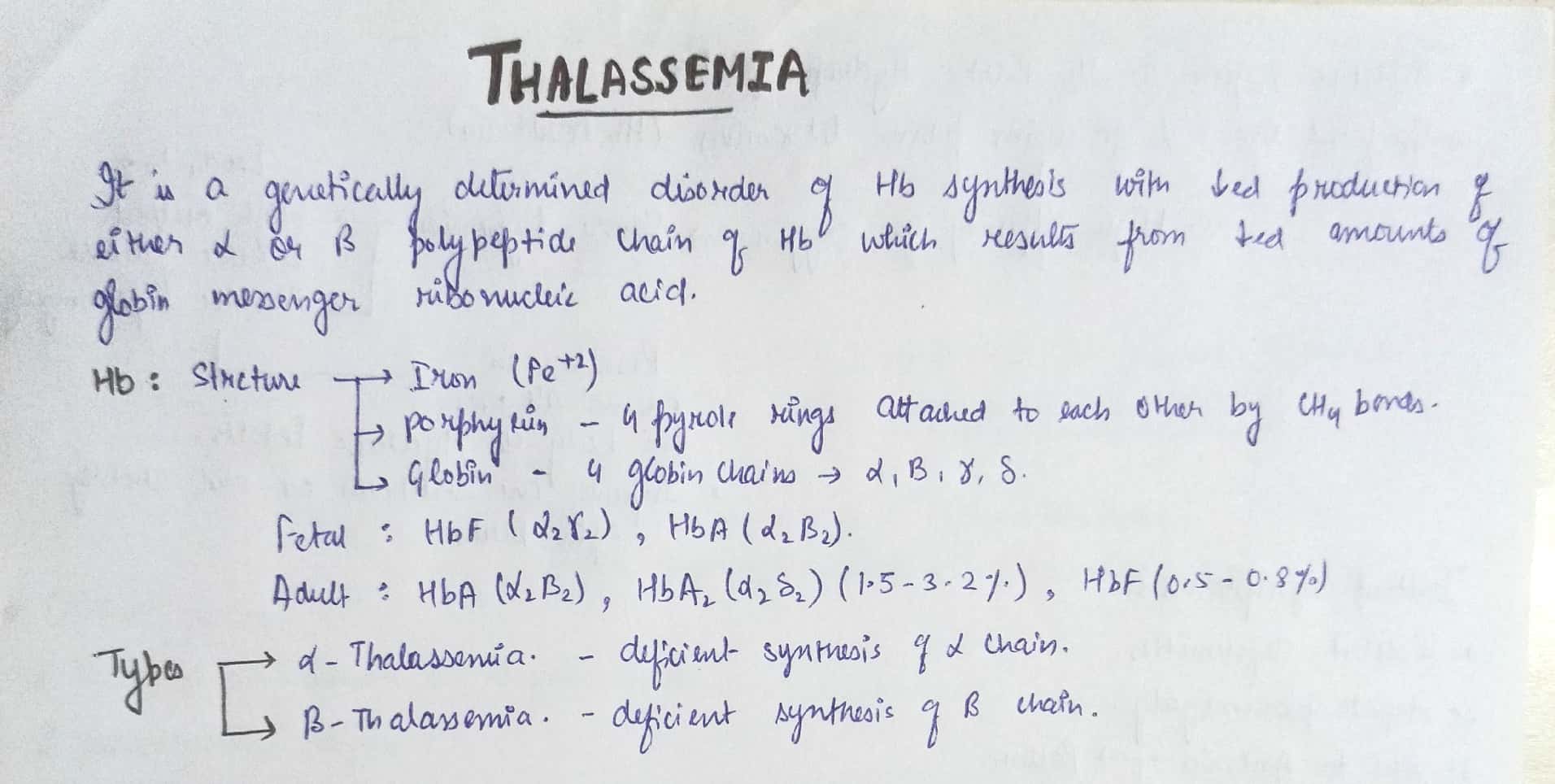
• Decrease Thyroid hormones
Classification
• primary hypothyroidism – due to cause within the thyroid gland itself.
• secondary hypothyroidism – due to failure of TSH production following pituitary or hypothalamic disease.
Causes
• spontaneous atropic thyroidism
• iodine deficiency
• iodine therapy
• thyroidectomy
• hashimoto’s thyroiditis
• dyshormonogenesis
• drug-induced ( lithium , amiodrone etc)
• radiation therapy
clinical features
A. Thyroid gland enlargement
B. Gastrointestinal
• weight gain
• decrease in appetite
• constipation
• acsite
C. Cardiorespiratory
• angina
• bradycardia
• hypertension
• pericardial effusion
• Pleural effusion
• cardiac failure
D. Neuromuscular
•ache and pain
•muscle stiffness
•carpal tunnel syndrome
•delayed relaxation of tendon reflex • •depression
•psychosis
•cerebral ataxia
•myotonia
•deafness
E. Dermatological
• mycoderma(non- pitting edema of skin of hands , feet and eyelid)
• dry flaky skin and hair
• Alopecia
• purplish lips
• malar flush
• xanthelasma
• carotenaemia
F. Reproduction
• menorrhagia
• infertility
• galacoma
• impotence
G. Haemtological & miscellaneous
• macrocytosis
• anaemia
• cold intolerance
• tiredness
• harseness of voice
• low pitched sound
Slurred speech
Investigation
• serum T4 decrease; TSH increase ( > 20mU/l)
• serum cholesterol & triglycerides increase
• serum LDH, Ck increase
• serum Na+ decrease
• ECG – sinus bradycardia, low voltage QRS complex, ST – T wave abnormalities
• chest radiograph – Enlargement of cardiac shadow
Treatment
D.o.c – Thyroxine – 50 microgram/day for 3 weeks
then
100microgram/day for 3weeks
then
150microgram/day for maintenance dose
• pt with heart disease angina may worsen with thyroxine therapy -treated with beta block and vasodilators or CABG
It’s hard to believe that a sheet of rubber can make you feel more comfortable during a dental treatment and allow dentists to do better, but a “RUBBER DAM” can . S.C. BARNUM
It is a direct method of isolation. It is a safeguard against the bacterial contamination from saliva and accidental swallowing of instruments.
HISTORY :
ADVANTAGES:
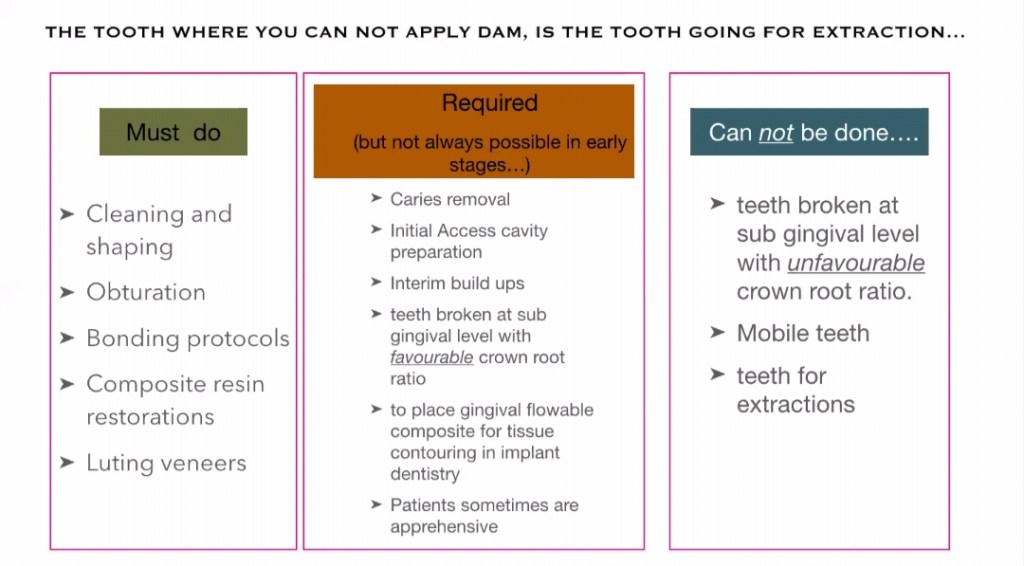
INDICATIONS:
ARMAMENTARIUM:
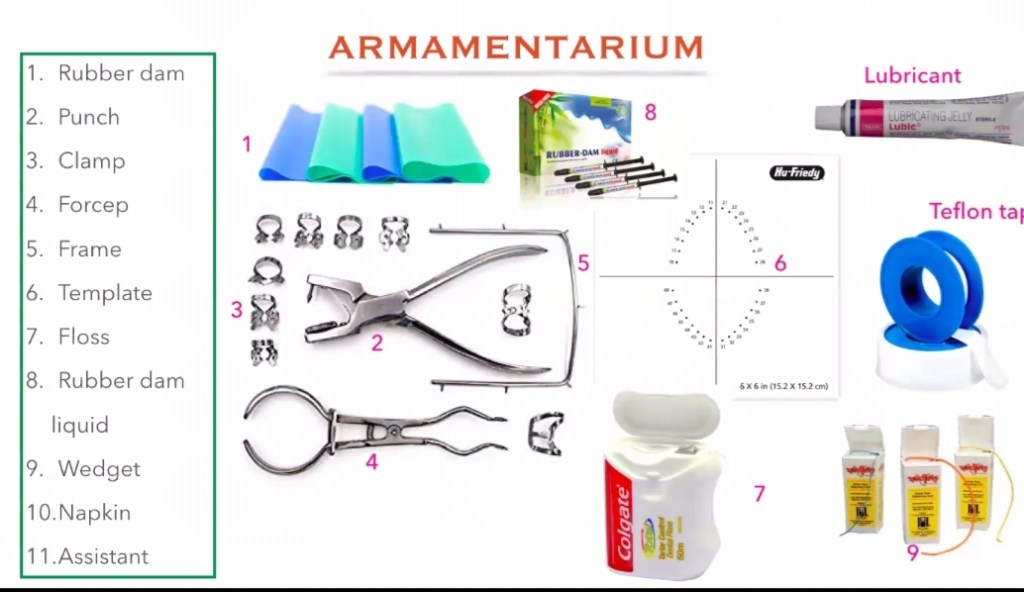
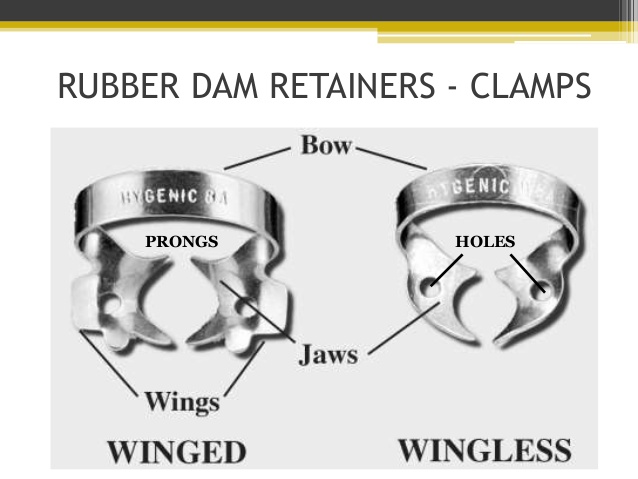
2, RUBBER DAM CLAMPS:
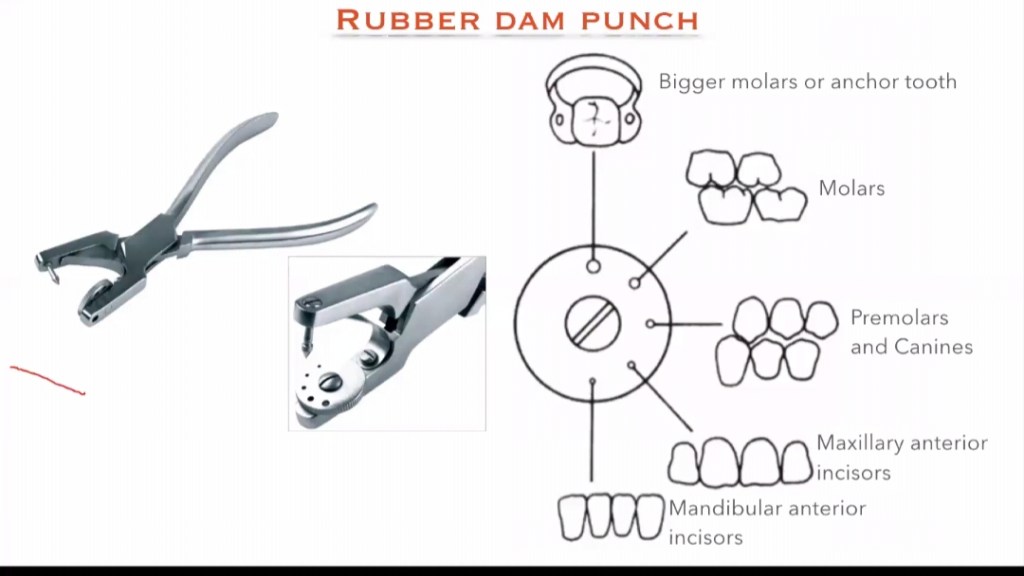
3. RUBBER DAM PUNCH :
It is an instrument which have a metal table and a tapered , sharp, pointed plunger to produce clear cuts holes on the rubber dam sheet so that the teeth can be isolated. It is of 2 types: Single hole punch and multi hole punch.
4. RUBBER DAM FRAME:
5. RUBBER DAM FORCEPS:
6. RUBBER DAM TEMPLATE:
7. RUBBER DAM NAPKIN :
8. WEDGET CORDS:
9. FLOSS:
REFERENCE: GROSS-MAN’S ENDODONTIC PRACTICE 13TH EDITION .
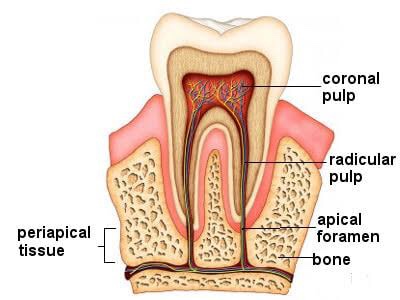
➡️ For all operative procedures, the shape of pulp chamber & its extensions into the cusps, pulpal horns is important.
➡️ In some developmental disturbances the pulpal horn projects high into the cusps & exposure of pulp can occur when it is least anticipated.
➡️ Pulpitis is the response of the traumatized pulp with trauma being the result of a bacterial infection as in dental caries or physical trauma to tooth structure.
➡️ Pulpitis in milder form could result in focal reversible pulpitis & may progress if left unchecked to acute & chronic forms of pulpitis.
➡️ Well vascularized pulpal tissue may at times in carious molar teeth of young adults & children with open apex exhibit a form of hyperplasia seen clinically in exposed pulp chamber as a protruding red mass of granulation tissue called pulp polyp or chronic hyperplastic pulpitis.
➡️ Inflammation within pulp may also sometimes result in a condition called pulp polyp, internal resorption or pink tooth.
➡️ Pulp infection can spread apically into PDL causing granuloma, abscess, cysts.
➡️ Pulp stones lying at the opening of the root canal may cause difficulty to locate the root canals.
➡️ A necrotic pulp can cause spread of disease to periodontium through an accessory canal.
➡️ Pulp capping is successful in non-infected or minimally infected accidentally exposed pulp in individuals of any age.
Source: Internet, Grossman’s Textbook of Endodontics
Dentowesome 2020 @ dr.mehnaz
BY Dr. KRITI NAJA JAIN :-
1. FIBROUS DYSPLASIA :-
Def:- Fibrous dysplasia is an uncommon nonhereditary, developmental anomaly of the bone due to a defect in osteoblastic differentiation and maturation.
HISTOPATHOLOGY:


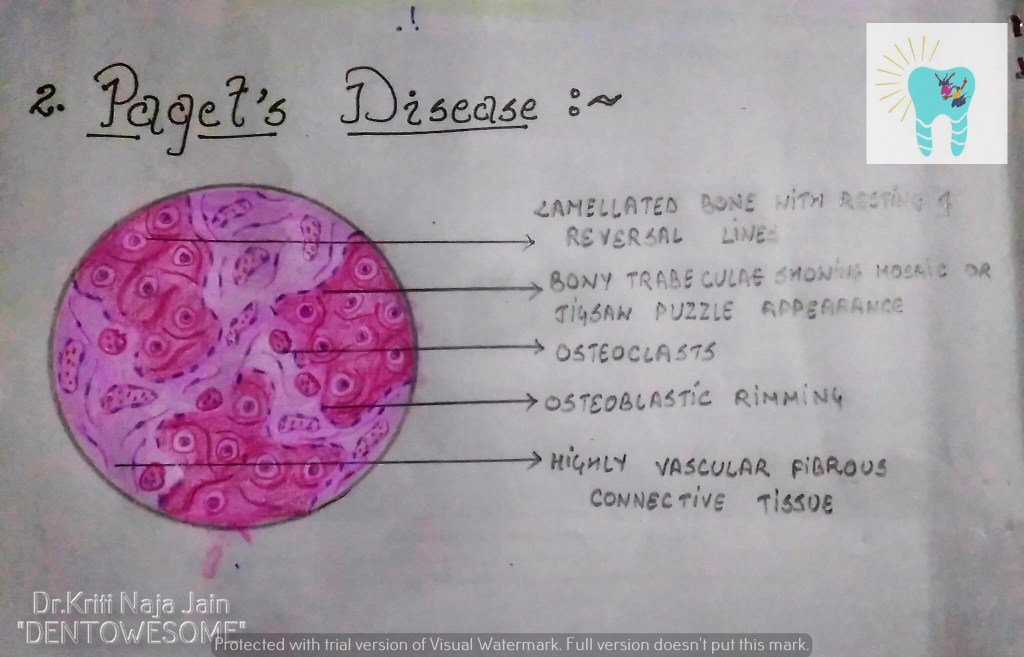
2. PAGET’S DISEASE (OSTEITIS DEFORMANS):-
Def:- Paget’s disease of bone is a condition characterized by abnormal and anarchic resorption and deposition of bone, resulting in distortion and weakening of the
affected bones.
HISTOPATHOLOGY:-

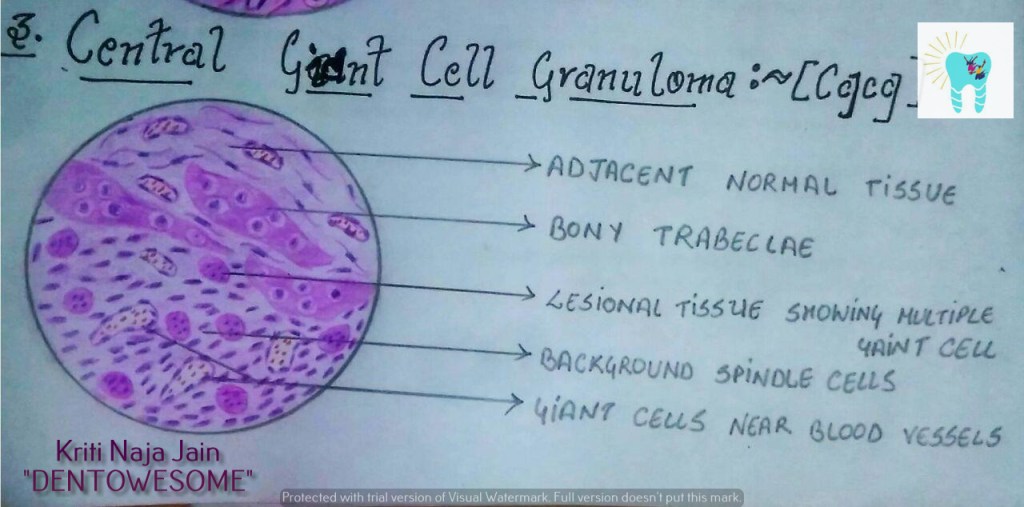
3. CENTRAL GAINT CELL GRANULOMA(GIANT CELL LESION; GIANT CELL TUMOR):-
Def :- Central giant cell granuloma (CGCG) is an uncommon, benign and proliferative lesion whose aetiology is not defined. Central giant cell granuloma is a relatively common benign intraosseous destructive giant cell lesion, which often affects the anterior part of the jawbone. By seeing clinical and radiographically , CGCG is divided into two types:-
1. Nonaggressive lesions make up most cases, exhibit few or no symptoms, demonstrate slow growth, and do not show cortical perforation or root resorption of teeth involved in the lesion.
2. Aggressive lesions are characterized by pain, rapid growth, cortical perforation, and root resorption. They show a marked tendency to recur after treatment, compared with the nonaggressive types.
HISTOPATHOLOGY:-

REFERENCE:-
1.Maji Jose 2nd edition
In NEET MDS Preparation process, your Oral pathology knowledge needs to be sound. Without knowledge in oral pathology, a lot of your final year may not make sense. A lot of overlaps exist between oral pathology, oral medicine, periodontics, and endodontics. In this article, we bring you the standard books to refer & most important topics which cater under the topic Oral Pathology & Medicine along with few preparation tips.
Given below are the list of Questions MERITERS experts will answer that are essential for an effective and efficient preparation:
20-22/240 Questions (9%)

Author : B Sivapathasundharam
INR 1,750 Buy on Amazon
Author : Brad W. Neville DDS, Douglas D. Damm DDS, Carl M. Allen DDS MSD, Jerry Bouquot DDS MSD
INR 1,995 Buy on Amazon
Author : Michael Glick
INR 1,753 Buy on Amazon
| UNIT | MOST IMPORTANT TOPICS |
|---|---|
| Developmental Disturbances | Developmental disturbances of TeethDevelopmental disturbances sizeShape Developmental disturbances of FaceDevelopmental disturbances of TongueTongueDevelopmental disturbances of FaceDevelopmmental disturbances of Jaw |
| Benign And Malignant Tumours Of Oral Cavity | General considerationPrecancerous lesions and conditions Basal cell carcinoma Squamous cell carcinoma TNM staging Treatment modalities Verrucous carcinoma Hemangioma KAPOSI ‘s sarcoma Nevi Melanoma Neoplasm of Muscles, Nerve tissue Multiple myeloma Connective tissue tuomours of Jaw Burkitt’s lymphoma |
| Diseases Of Salivary Glands | Mucocele and Ranula Mickulz’s disease and Sjogren syndrome Pleomorphic adenoma Warthin’s tumor Cylindroma Oncocytic adenoma |
| Dental Caries | Theories of dental caries Etiologies of dental caries Stephan’s curve Classification of dental caries Histopathological zones of Dentine Histopathology od dental caries (Enamel caries) |
| Pulp And Periapical Infections | Classification of periapical infection Cellulitis Ludwig’s angina Osteomyelitis |
| Physical And Chemical Injuries | Physical And Chemical InjuriesPigmentationsRegressive alterations of teethMucocele Other physical and Chemical Injuries. |
| Diseases Of Bones & joints | Osteogenesis imperfectaOsteopetrosis Achondroplasia Osteoporosis CherubismFibrous dysplasia Paget’s disease Cleidocranial dysplasia CGCGSyndromes associated with bone Osteosarcoma |
| Diseases Of Nerves & Muscles | Trigeminal Neuralgia Glossopharyngela neuralgia Bells palsy Syndromes associated with nerve pathology Disease of Muscular or connective tissue origin |
| Skin And Vesiculobullous Lesions | Skin lesions Ectodermal dysplasia Lichen planus Erythema multiforme Classification of vesiculobullous lesions 5Psoriasis Miscellaneous |
| Bacterial Infections | Sinus Botryomycosis Sarcoidosis Syphilis Actinomycosis Leprosy |
| Viral Infections | Herpes Simplex Virus Herpes Zoster Cox sackie virus Paramyxovirus Apthous ulcers |
| Mycotic Infections | Candidiasis Histoplasmosis Mucormycosis Phycomycosis |
| Oral Aspects Of Metabolic Diseases | Vitamin D deficiency HyperparathyroidismHyperpituitarism Hand Schullar christian disease Hypophosphatasia Amyloidoisosi and other disease |
| Tongue Disorders | Tongue Disorders |
| Pigmentation | Pigmentation |
| Diseases Of Blood | Hemophilia Von Willebrand’s diseaseTypes of anaemia Aplastic anaemia Thrombocytopenic purpura Leukemia Miscellaneous |
| Miscellaneous | Miscellaneous |
1. Single best answer
2. Image based questions
3. True or false type questions
Please watch the above featured video for more detailed explanation about this article.
We hope this blog will assist you in preparing this subject meticulously for MDS entrance exams.
Prepare judiciously..
SOURCE: MERITERS!!
