Written by: Ashtinder kaur


References: Textbook of pedodontics shobha tandon 2nd edition
Written by: Ashtinder kaur
References: Textbook of pedodontics shobha tandon 2nd edition
Written by : Ashtinder kaur



References: Textbook of pedodontics shobha tandon 2nd edition
Written by : Ashtinder kaur


References: Textbook of pedodontics shobha tandon 2nd edition
Volume of air inspired during quiet breathing → 0.5 liters
Forced inhalation → 3.0 liters
= 6.0 liters lung volume
The volume of forceful exhalation → 1.0 liter
= 1.5 liters lung volume
The volume of air still in the lungs after maximal expiration
VC = TV + IRV + ERV
TLC = VC + RV
IC = IRV +TV
FRC = ERV + RV
Trachea → left, right bronchi → terminal bronchioles
Physiologic dead space = anatomic dead space.
Physiological dead space > anatomic dead space.
The conducting portion
Pharynx
Larynx
Lungs
Asthmatic airway:
By now you may already know that the kidneys filter your blood. Microscopically speaking, it is structures known as the glomeruli (singular ‘glomerulus’) inside of the kidney that perform the actual filtration. If they, like the car and fridge filter, are damaged, then they will leak stuff into your urine that normally shouldn’t be there.
A glomerular disorder that causes hypoalbuminemia, proteinuria, and edema is known as nephrotic syndrome. All sorts of glomerulopathies (diseases of the glomerulus) can result in nephrotic syndrome, including:
CAUSES OF NS
Minimal change disease:
Membranous nephropathy
Focal segmental glomerulosclerosis
I don’t want you to really get bogged down in remembering the causes of nephrotic syndrome so much as understanding what actually happens. Any of those diseases damage the glomerulus. The glomerulus is the filter that is supposed to keep large things, such as proteins, inside of the blood while filtering out smaller toxins that get excreted in the urine. If the pores of the glomerulus, the little holes that allow for things to pass through the glomerulus and into the urine, are damaged, they get bigger. Bigger pores in any filter means that things that should’ve been kept out are now leaking into the urine and out of the blood.
You can reproduce this point at home. Take out some dirty old rag you no longer need. If you look really closely, you will see that there are small holes in the rag. They’re truly tiny. This rag will represent our glomerulus, the filter. Turn on the faucet in a sink and place a couple of golf balls or something similar into the rag. Now place all of this under the running faucet. You’ll note that the golf balls aren’t filtered through, but the water and all the microscopic parts of it easily pass through to the other side.
Now go ahead and cut some big holes into the rag, mimicking the damage glomerulopathies cause. Repeat what you did before. This time around, not only will the water leak through but the golf balls will pass through as well.
In the case of nephrotic syndrome, a protein called albumin is like a golf ball that leaks out of the blood and into urine when it normally shouldn’t. This leakage results in decreased levels of albumin in the blood, termed hypoalbuminemia and increased levels of protein in the urine, known as proteinuria.
SERUM ALBUMIN= Normal Value is 3.5-5.5 but in NS the value decreases to 2.5 g/dl
PROTENURIA
Old= more than 3.5 g/dl
Children= More than 2g/dl
Adult= More than 3g/dl
Proteinuria during nephrotic syndrome is in the range of three grams per day or more. This is in contrast to other causes of proteinuria, such as a kidney infection, which results in less than that (up to two grams per day, normally).
You should note that the protein albumin, now leaking out of blood and into the urine, is important in keeping fluid within the blood vessels and out of the body tissues. Albumin is like a sponge that sucks up water into the vasculature. Since there’s less albumin in the blood during nephrotic syndrome, there are fewer sponges in the blood vessels. This means water leaks out of the blood vessels and into the tissues. This is what is known as edema. Edema causes a person to literally swell up with fluid. Keeping this in mind, lets understand:
Initiating Mechanism of Edema:
Decrease in oncotic pressure due to albumin loss —> Fluid shift from intravascular to extravascular—> causing effective decrease in intravascular volume.
Hence, increase in renin and aldosterone leading to increase in water and sodium retention.

References: Textbook of pedodontics shobha tandon 2nd edition
HOW TO ENJOY THE PREPARATION
Graves’ disease is the most common cause of hyperthyroidism, or overactive thyroid. In Graves’, the body’s hyperactive immune system produces an antibody that attaches to the TSH receptors on the thyroid gland. Because TSH isn’t actually triggering the release of T3 and T4, the negative feedback system the body has in place doesn’t work and the thyroid continually makes and releases thyroid hormones. Since the antibodies consistently trigger the thyroid cells to produce more T3 and T4, the body responds by increasing the thyroid’s size, causing a classic thyroid symptom called goiter.
The other primary external symptom of Graves’ is called exophthalmos, or protrusion of the eyes. Exophthalmos has two causes. The first is due to a prolonged ‘fight or flight’ response – the widening of the eyes by a retraction of the upper lids. The second is due to that overactive immune system: the fat and muscles around the eyes become swollen due to an increase in the number of lymphocytes present and other symptoms of inflammation, pushing the eyes forward.
Internally, excess thyroid hormones are also stressing the sympathetic nervous system, constantly preparing us for a threat that’s not really there. Resting metabolic rate increases, causing weight loss. Resting heart rate jumps irregularly (arrhythmia) or increases to over 100 beats per minute (tachycardia). Heat intolerance and heavy perspiration are also symptoms.
Diagnosis of Graves’ through blood tests relies largely on high-circulating levels of T3 and T4 and low TSH levels, as well as antibodies for TSH receptors. Occasionally, an iodine uptake test is used for confirmation. In this test, the patient consumes a low dose of radioactive iodine. Since thyroid cells actively take up iodine, the degree and location of overactive cells present in radiography as darkened areas of the thyroid.
Pharmaceutical treatment for Graves’ consists of symptom relief through beta blockers, which dull sympathetic nervous system activity, and antithyroid medications that prevent the thyroid from making hormones, such as methimazole. In more severe cases, surgical removal of or destruction of the hyperactive cells through radioactive iodine is a treatment option.
– current approach in dentistry in Covid state Amidst the pandemic state with the high transmissibility of the disease through air & droplets and considering that routine dental procedures usually generate aerosols; alterations to dental treatment is of prime concern to maintain a healthy environment for patient & dental team.Here is where the approach of […]
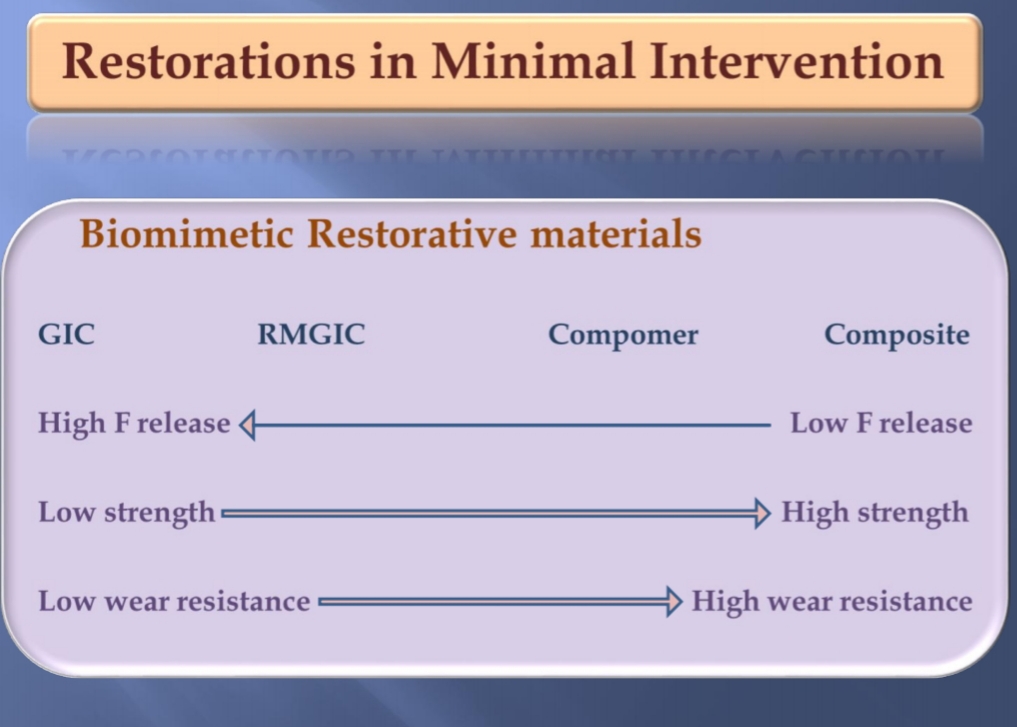
Minimal Invasive Dentistry
Sources: Slideshare-Minimal invasive dentistry by Nabeela Basha , Minimal intervention dentistry by Dr.Nagamaheswari, Sturdvent’s South Asian edition,Clinical operative dentistry principles & practice by Ramya Raghu,textbook of preventive and community dentistry by SS Hiremath
Sources:
