INTERESTING FACTS ON ORAL CAVITY!

Cigarettes contain nicotine and by smoking regularly and for long hours, your body becomes dependent on it. Giving up smoking can cause nicotine withdrawal symptoms which are :
Stop smoking medicines along with nicotine replacement therapy are effective aid to tobacco cessation & can help control these symptoms.
What are these?
3 types –

How does it work?
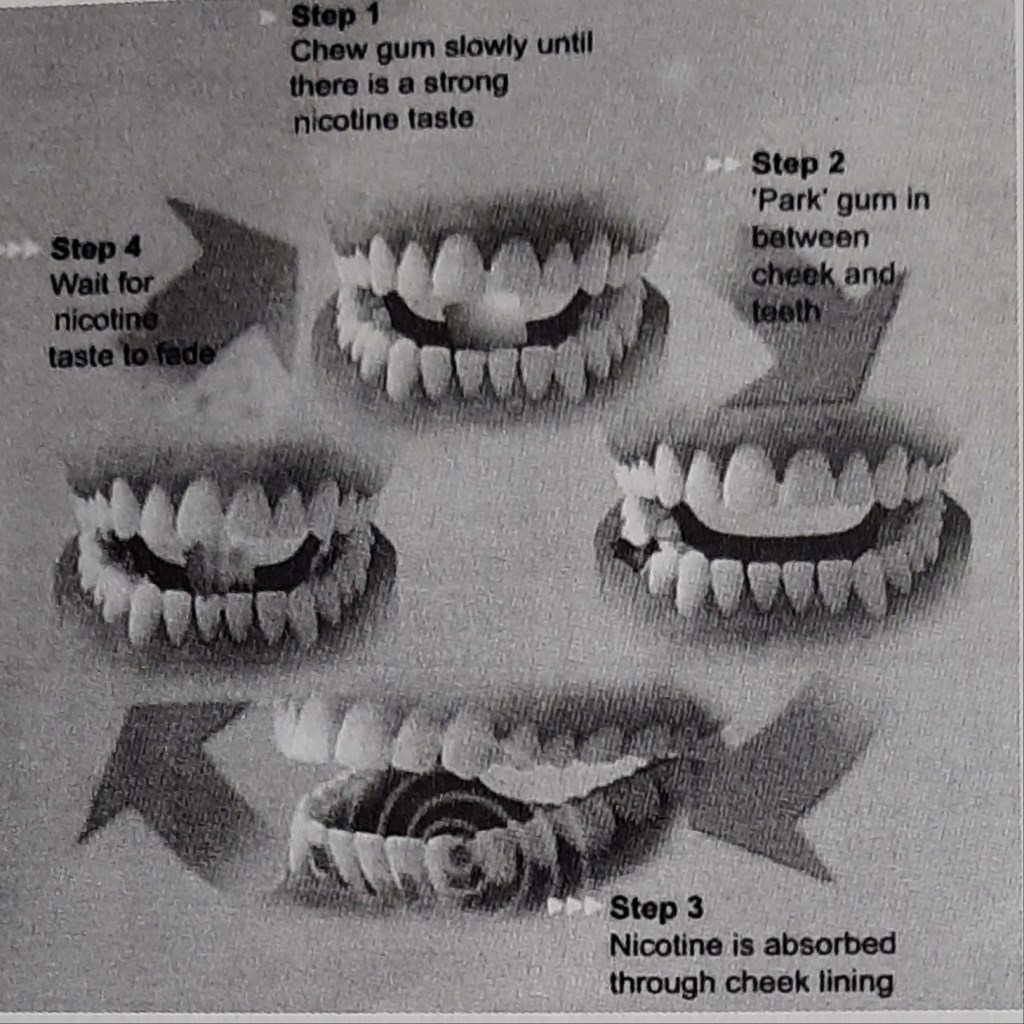
Tobacco intakers who are motivated to quit the habit & are dependent on nicotine should be offered NRT.

Is it safe?
NRT is safe because of the facts that the nicotine levels are low and it’s less addictive delivery mechanism (unlike smoking tobacco where the nicotine reaches the brain quickly) and also because most of the harmful problems are caused by the other components of tobacco smoke ,not by the nicotine.
NRT is safe for most adults and in people with stable cardiac diseases, but caution needed in unstable,acute cardiovascular disease,pregnancy,or breastfeeding or in those aged under 18 years.
Brownie points-reduces the constant urge to munch on food,thus reducing weight gain.😊
When should one stop using NRT?
Most courses of NRT recommend use for about 12 weeks.This is because it takes this much time for the brain to adjust to working without the high doses of nicotine that the cigarettes supply.However there is no hard and fast rule.After starting the therapy,most people mistake the lack of discomfort for the belief that the addiction is over,leading to stop using the product too soon. This can result only in reappearing of the symptoms.
The best method is to take the help of the health professional when you start the therapy and keep them updated about the progress.
Lastly ,we all are not the same….each tobacco smoker’s tendency & pattern to quit may vary & it depends on different factors like age,gender,environment, general physical and mental health.
Sources:S.S Hiremath textbook of preventive and community dentistry, http://www.healthunlocked.com(Quit Support)

Tobacco is the leading preventable cause of death in the world and is the only consumer product that kills when used as intended by its manufacturers ;which may become deadly for non-smokers also.
FACTS & FIGURES:
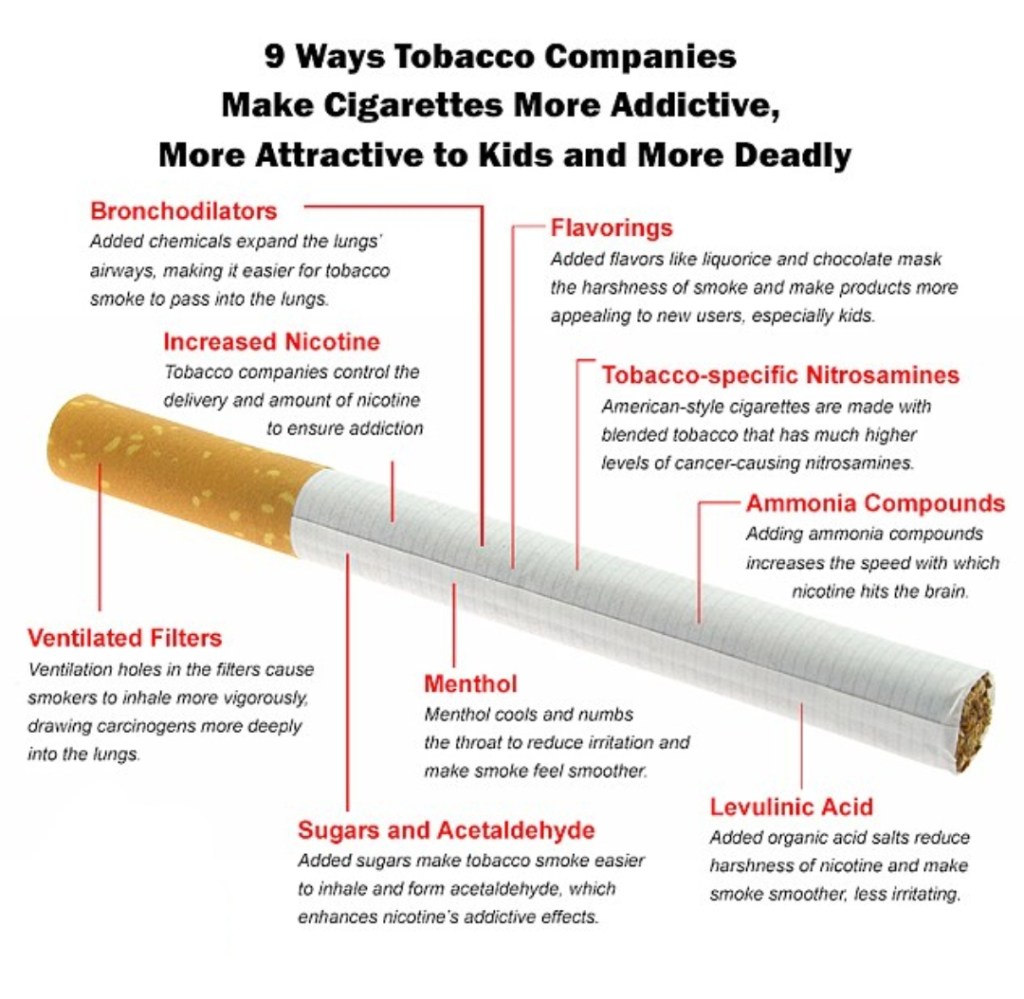
EFFECTS OF NICOTINE :
‘Nicotine itself is not carcinogenic unless it undergoes nitrosation to form nitrosamines(during tobacco curing & combustion).’

HOW TO ASSESS TOBACCO DEPENDENCE?
A question-answer session with the individual would be very helpful ….

THE 5 A’S :

Lastly ,dentists play a major role in helping a patient quit smoking because we might be the first to detect an abnormality( be it a small stain or an abnormal mass ) in the oral cavity during routine examination. Do your part ,every small step counts……
Sources- S.S Hiremath textbook of preventive and community dentistry ,www.alhambraesd.org ,www.tobaccofreekids.org


Here’s a list of the few laboratory tests and investigations which are helpful & specific for diagnosis of certain diseases and conditions.


Sources : Burkets oral medicine 11th edition,Shafer’s textbook of oral pathology 7th edition,www.glasbergen.com
Rubber dam was introduced byBarnum, a New York dentist in 1863
Advantages of using a rubber dam
• It is raincoat for the teeth
• It helps in improving accessibility and visibility of the working area
• It gives a clean and dry aseptic field while working
• It protects the lips, cheeks and tongue by keeping them out of the way
• It helps to avoid unnecessary contamination through infection control
• It protects the patient from inhalation or ingestion of instruments and medicaments
• It helps in keeping teeth saliva free while performing a root canal so that tooth does not get decontaminated by bacteria present in saliva
• It improves the efficiency of the treatment
• It limits bacterial laden splash and splatter of saliva and blood
• It potentially improves the properties of dental material.
• It provides protection of patient and dentist.
Disadvantages of using a rubber dam
• Takes time to apply
• Communication with patient can be difficult
• Incorrect use may damage porcelain crowns/crown margins/ traumatize gingival tissues
• Insecure clamps can be swallowed or aspirated.Contraindications of use of rubber dam
• Asthmatic patients
• Allergy to latex
• Mouth breathers
• Extremely malpositioned tooth • Third molar (in some cases).
Rubber dam equipment
• Rubber dam sheet• Rubber dam clamp • Rubber dam forceps• Rubber dam frameRubber dam accessories•Lubricant/petroleum jelly• Dental floss• Rubber dam napkin.

Rubber Dam Sheet

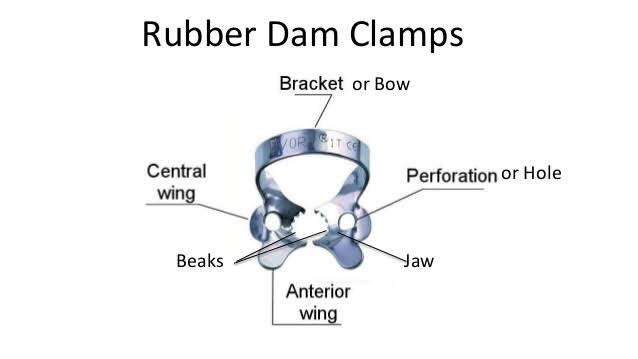
Rubber Dam Clamps
Rubber Dam Forceps

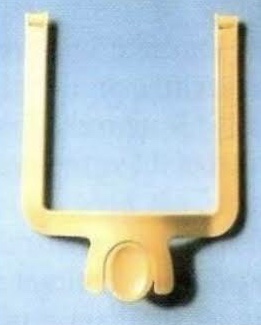
Rubber Dam Frame
Rubber dam frame supports the edges of rubber dam .Frames have been improved dramatically since their old style with the huge ‘butterflies’.Modern frames have sharp pins which easily grip the dam. These are mainly designed with the pins that slope backwards.
• Rubber dam frames are available in either metal or plastic.
• Plastic frames have advantage of being radiolucent.
• When taut, rubber dam sheet exerts too much pull on the rubber dam clamps, causing them to come loose,especially clamps attached to molars.
• To overcome this problem, a new easy-to-use rubber dam frame (Safe-T-Frame) has been developed that offers a secure fit without stretching the rubber dam sheet. Instead, its “snap-shut” design takes advantage of the clamping effect on the sheet, which is caused when its two mated frame members are firmly pressed together. In this way, the sheet is securely attached, but without being stretched. Held in this manner, the dam sheet is under less tension, and hence, exerts less tugging on clamps—especially on those attached to molars.

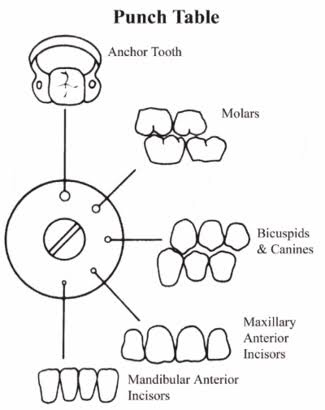
Rubber Dam Punch


Rubber Dam Napkin
• This is a sheet of absorbent materials usually placed between the rubber sheet and soft tissues.
• It is generally not recommended for isolation of single tooth.

REFERENCE – NISHA GARG TEXTBOOK OF ENDODONTICS AND GROSSMAN’S TEXTBOOK OF ENDODONTICS
A continuation of the previous post on syndromes and easy short forms to remember the key features. Hope you find it helpful. Sources: Shafers textbook of oral pathology,www.rxpg.com,instagram–@_dentistars_,@dental_exams,www.medinaz.com

Method II: Placement of rubber dam and clamp together

Split dam technique is indicated:
• To isolate anterior teeth
• When there is insufficient crown structure
• When isolation of teeth with porcelain crown is required. In such cases placement of rubber dam clamp over the crown margins can damage the cervical porcelain.
• Dam is placed without using clamp.
• Here two overlapping holes are punched and dam is stretched over the tooth to be treated and adjacent tooth on each side.
REFERENCE- NISHA GARG TEXTBOOK OF ENDODONTICS
