Contd…Page 2👇🏻
Contd…Page 2👇🏻

Oral disease transmitted by droplet spread/contact with the lesion.
• Incidence – Children & young adults. <6 months of age: Rare (Due to presence of circulating Ab. in the infant derived from the mother)
• Clinical Manifestations:
➡️ Within a few days mouth becomes painful with gingiva being inflamed, edematous & erythmatous.
➡️ Involvement of lips, tongue, buccal mucosa, palate, pharynx & tonsils.
Yellowish fluid-filled vesicles develop
⬇️
Rupture
⬇️
Shallow, ragged, extremely painful ulcers (grey membrane, erythmatous halo)
➡️ Ulcers heal within 7-14 days with No scar formation
➡️ Isolation of HSV-1 from these lesions after onset: (2 – 6 days)
➡️ Trigeminal for HSV-1 (Virus remain latent until reactivated in the ganglia)
➡️ Viral DNA to Host DNA – lifelong infection
➡️ Incubation Period: 2-20 days
➡️ While most children will be asymptomatic, diagnosis of children with symptoms is made based on clinical presentation of erythematous gingiva, mucosal hemorrhages, and clusters of small erupted vesicles throughout the mouth.
➡️ The condition is highly contagious and complications range from indolent cold sores to dehydration and even life-threatening encephalitis.
➡️ Symptomatic relief primarily involves pain management and oral fluids to prevent dehydration until the viral infection subsides.
➡️ Acyclovir is a well established antiviral drug used effectively for the treatment of herpes simplex infections, chickenpox (shortened fever time), and shingles. It is also used frequently for children with immunodeficiency.
➡️ The current recommended dose of oral acyclovir is 40 to 80 mg/kg a day, divided in 3 or 4 doses, for 7 days. Caregivers should be aware of potential adverse effects of acyclovir such as headache, malaise, and vomiting.
Dr. Mehnaz Memon🖊
References: Shafers Textbook Of Oral Pathology 7Ed, Internet

1
2
3
References: Shafers Textbook Of Oral Pathology 7Ed
➡️ Reticular, erythematous, erosive lesions or ulcerations with whitish streak. Atypical location & absence of bilateral occurrence.
Dr. Mehnaz Memon🖊
References: Shafers Textbook Of Oral Pathology 7Ed
➡️ They are clearly visible & can be easily diagnosed as per the clinical features alone – high viral load. They are useful markers of disease progression & immuno-suppression.
➡️ The EC (1995) gave two diagnostic criterias:
🔸 Candidiasis – 4 clinical patterns observed
🔸 Hairy Leukoplakia – Associated with EBV
⬇️
Langerhan cells by HIV
⬇️
cause reactivation of EBV
⬇️
epithelial hyperplasia
🔸 Kaposis’s Sarcoma (HHV-8)
🔸 Non-hodgkin’s lymphoma
🔸 Periodontal Disease
🔸 Bacterial infection
🔸 HSV, Herpes Zoster
🔸 Melanotic hyperpigmentation (Brown-black intra-oral focal/diffuse Macules)
🔸 Necrotizing Ulcerative Stomatitis
Dr. Mehnaz Memon🖊
References: Ghom’s Oral medicine & Internet
References: Shafers Textbook Of Oral Pathology 7Ed


source – don’t remember, had written it long back. , textbook – Shafers

source – don’t remember, had written it long back. , textbook – Shafers

source – don’t remember, had written it long back. , textbook – Shafers

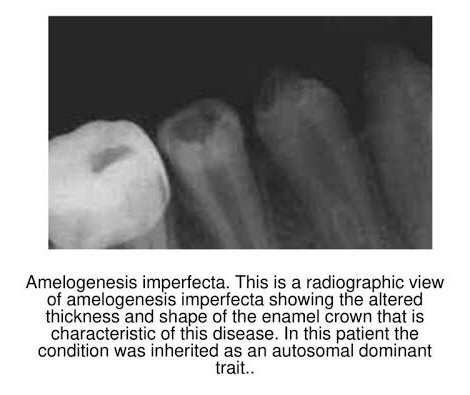
➡️ Represents a group of hereditary defects of enamel unassociated with any other generalized defects. It is entirely an ectodermal disturbance, since the mesodermal components of the teeth are basically normal.
➡️ Otherwise known as…


➡️ 3 stages:
Based on clinical, histological & genetic criteria:
🔹 TYPE I HYPOPLASTIC
🔹 TYPE II HYPOMATURATION
🔹 TYPE III HYPOCALCIFICATION
🔹 TYPE IV COMBINATION TYPE
1) Hypoplastic – Enamel not formed to full normal thickness.
2) Hypomaturation –
3) Hypocalcified –
References: Shafer’sTextbook Of Oral Pathology; Internet
