A neoplasm of epidermal melanocytes and third most common cancer of skin.
▪️Arises in preexisting mole. Appearance – Large, flat, spreading lesion; deeply pigmented Nodule
🔹Precursor Lesions:
(i) Congenital Nevi
https://dentowesome.wordpress.com/2020/05/18/oral-nevi/
(ii) Dysplastic Nevi (Atypical Mole)
(iii) Lentigo Maligna: Also called as Hutchinson’s freckle, is a tan or black on the skin that looks like a freckle.
- Grows slowly
- Dark, thick, nodular, mottled
- Seen on one side of the face of an older adult who had a large amount of sun exposure.
🔹Etiology:
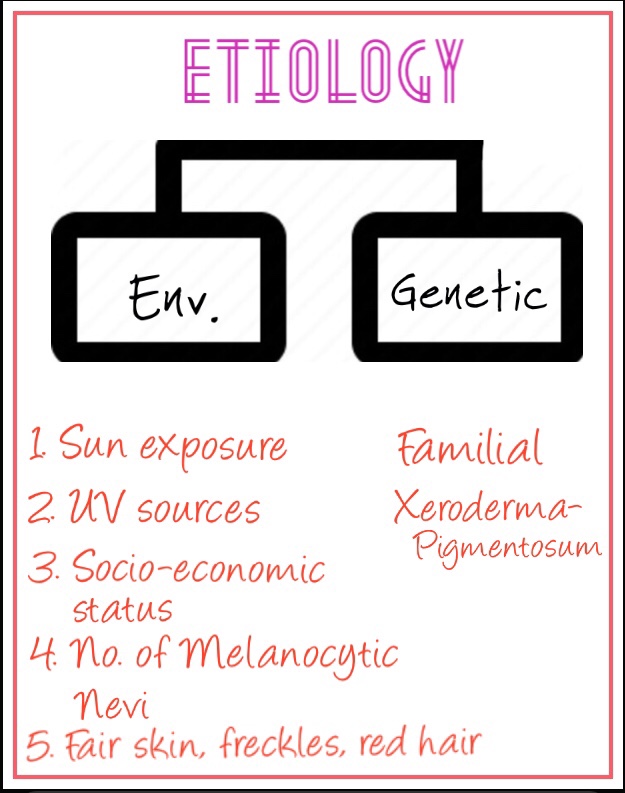
• Genes in the development of Melanoma:
• Phases in the growth of Melanoma:
- Radial
- Vertical
🔹Classification:
1. Superficial spreading Melanoma:
- most common type (65%)
- Radial growth phase – premalignant melanosis/pagetoid melanoma in situ
- Vertical growth phase – Increase in size, color, nodularity/ulceration
- Lesions are usually flat, scaly or crusty & 2 cm in diameter
- Found in trunk & back of Men; Legs of women
- Median age of occurrence – 50’s
2. Lentigo Maligna Melanoma:
- Least serious form
- More in women
- Macular lesion on malar skin of middle-aged and elderly
3. Nodular Melanoma:
- Exhibits only vertical growth phase
- Sharply delineated nodule, may be pink/black
- Occur in men on skin of head, neck & trunk
- Looks like blood blister
4. Acral Lentiginous:
- Also called muco-cutaneous Melanoma
- Less common with fair skin
- Palms of hands, soles of feet, mucous membrane, nail beds
- Median age of occurrence – in 50’s & 60’s
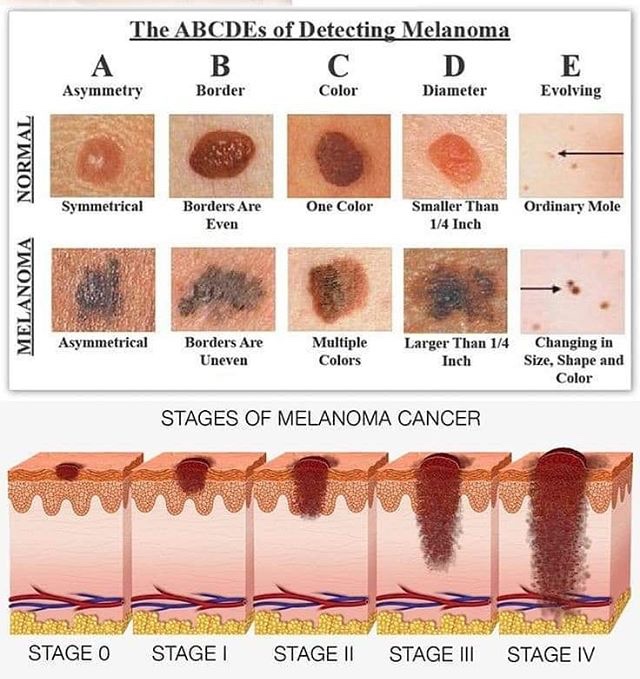
Assessing the ABCDE’s of Moles
🔹Oral Manifestations:

- Age: 55 yrs
- Sex: M>F
- Site: Palate/Gingiva
- Appearance: Deeply pigmented area; ulcerated/haemorrhagic; ⬆️ size
- Amelanotic melanomas: 5-35% of oral cases
Melanoma stages 5 years survival rates:
- Stage 0: Melanoma in situ ( Clark level I), 99.9% survival
- Stage I/II: Invasive melanoma, 85-99% survival
- Stage II: High risk Melanoma, 40-85% survival
- Stage III: Regional Metastasis, 25-60% survival
- Stage IV: Distant Metastasis, 9-15% survival
🔹Treatment depends on stage:
➡️ Metastases that cause symptoms but cannot be removed may be treated with radiation, immunotherapy, targeted therapy, or chemotherapy.
Dr. Mehnaz Memon🖊
References: Shafer’sTextbook Of Oral Pathology; Textbook Of Surgery by S.Das