• Adenomatoid odontogenic tumor (AOT), generally considered to be an uncommon tumor
• Occurs mostly in association with an unerupted maxillary cuspid.
• Some investigators consider it as a benign neoplasm, while others have categorized it as a hamartomatous malformation due to the limited size and to the lack of recurrence of most cases (attributed perhaps to its minimal growth potential).
• The AOT represents 3% to 7% of all odontogenic tumors.
• Although this lesion was formerly considered to be a variant of the ameloblastoma and was designated as “adenoma glioblastoma,” its clinical features and biologic behavior indicate that it is a separate entity.
PATHOPHYSIOLOGY:
• There is evidence that the tumor cells are derived from enamel organ epithelium.
• Investigators have also suggested that the lesion arises from remnants of dental lamina.
• The specific stimulus that triggers proliferation of the progenitor cells of AOT is unknown.
• Various hypotheses for the pathogenesis of AOT have been proposed. It could theoretically arise from the:
- Enamel organ
- The Epithelial lining of dentigerous cyst.
- Epithelial rests of Malassez of the deciduous or permanent tooth
- Remnants of the dental lamina.
CLINICAL FEATURES:
• The mean age of these patients was approximately 18 years, with a range of 5-53 years.
• However, 73% of the patient were under 20 years of age.
• Marked predilection: in females 64%: males 36%.
• Occurrence: greater in the maxilla (65%) than in the mandible (35%).
• In contrast to the ameloblastoma, this tumor occurs more frequently in the anterior part of the jaws with 76% developing anterior to the cuspid in the maxilla and mandible.
• Only very rarely does the lesion occur distal to the premolar area.
• It is of some interest that in at least 74% of the cases, the tumors were associated with an unerupted tooth, and in over two-thirds of the cases, this tooth was the maxillary or mandibular cuspid.
• Most tumors are relatively small, seldom exceed 3 cm in greatest diameter.
• Although a few large lesions have been reported.
• Peripheral (extraosseous) forms of the tumor are also encountered but are rare.
• These usually appear as small, sessile masses on the facial gingiva of the maxilla.
• Clinically, these lesions cannot be differentiated from the common gingival fibrous lesions.

***It is known as two-third tumour:
As it is seen :
• 2/3rd in females.
• 2/3rd in Anterior teeth region.
• 2/3rd in impacted tooth region.
• 2/3rd in cuspid region.
RADIOGRAPHIC FEATURES:
• They are frequently asymptomatic , are discovered during the course of a routine radiographic examination or when films are made to determine why a tooth has not erupted.
• Larger lesions cause a painless expansion of the bones.
• In about 75% of cases, the tumor appears as a circumscribed, unilocular radiolucency that involves the crown of an unerupted tooth, most often a canine.
• Follicular type of AOT may be impossible to differentiate radiographically from the dentigerous cyst.
• Radiolucency associated with the follicular type of AOT sometimes extends apically along the root past the cementoenamel junction.
• This feature may help to distinguish an AOT from a dentigerous cyst.
• Less often the AOT is a well-delineated unilocular radiolucency that is not related to an unerupted tooth, but rather is located between the roots of erupted teeth (extrafollicular type)
• The lesion may appear completely radiolucent: often, however, it contains fine (snowflake) calcifications.
• Rare, multilocular cases have been reported and a scalloped border is observed occasionally.
• Most cases are between 1 and 3 cm in greatest diameter. About 65% of reported cases also demonstrate faintly detectable radiopaque foci within the radiolucent lesion.
• Occasionally, a more obvious intralesional radiopacity may be identified, usually eccentrically positioned within the lesion.
• Divergence of roots and displacement of teeth occurs more frequently than root resorption.
• Orbital and maxillary sinus encroachment have been reported.
• Gingival lesions may cause slight erosion of the underlying alveolar bone cortex.


HISTOLOGICAL FEATURES:
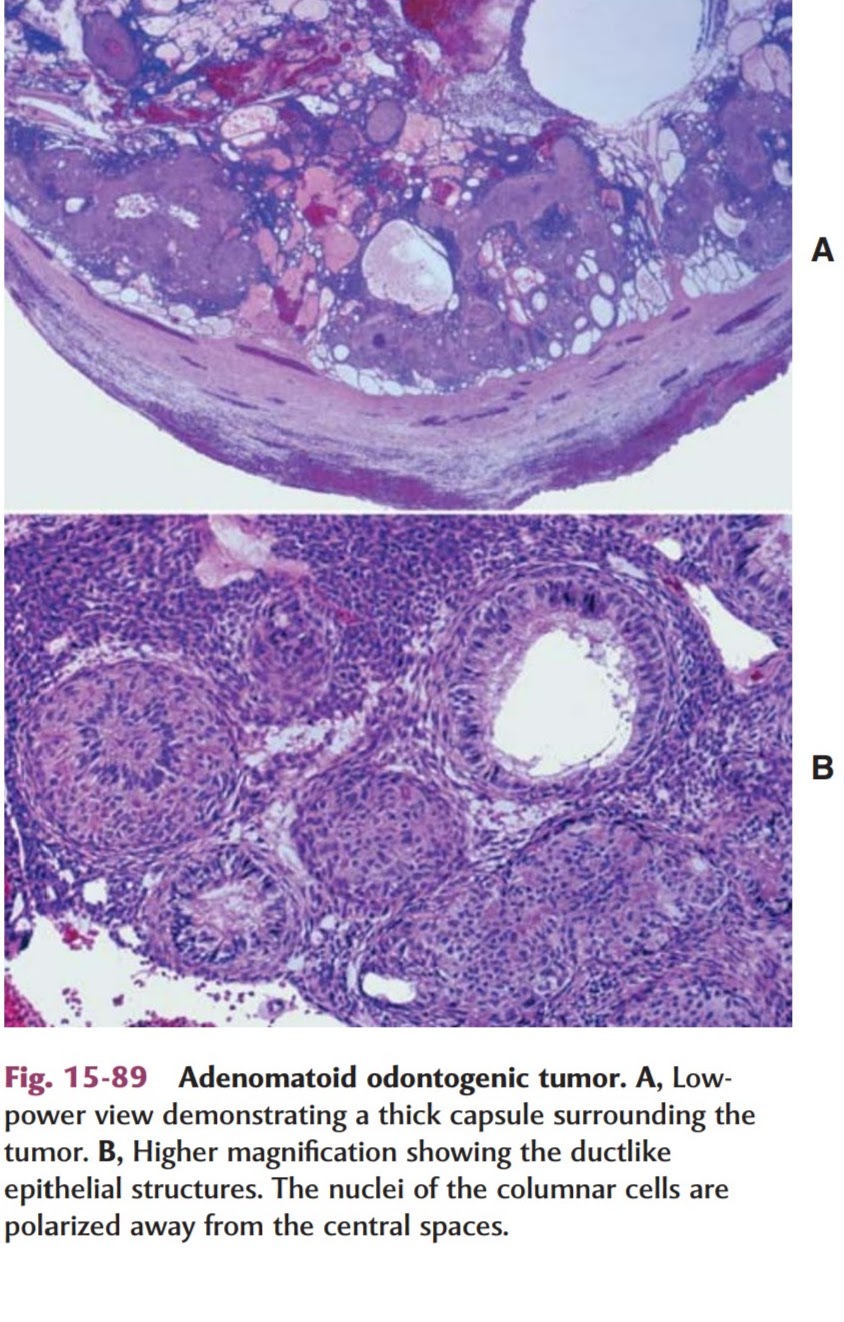
• AOT is a well-defined lesion that is usually surrounded by thick capsule.
• When the lesion is bisected the central portion of the tumor may be essentially solid or may show varying degrees of cystic change.
• Microscopically , the tumour composes of spindle shaped epithelial cells that form sheets, strand, or whorled masses of cells in a scant fibrous stroma
• The epithelial cells may form rosette like structures about a central space, which may be empty or contain small amounts of eosinophilic material.
• This material may stain for amyloid.
• The tubular or duct like structures, which are the characteristic feature of the AOT, may be prominent, scanty, or even absent in a given lesion.
• Lesion may consist of a central space surrounded by a layer of columnar or cuboidal epithelial cells.
• The nuclei of these cells tend to be polarized away from the central space.
• Small foci of calcification may also be scattered throughout the tumor.
• These have been interpreted as abortive enamel formation.
• Some tumours may contain larger areas of matrix material or calcification.
• This material has been interpreted as dentinoid or cementum.
• Some lesions also have another pattern, particularly at the periphery of the tumor adjacent to the capsule.
• This consists of narrow, often anastomosing cords of epithelium in an eosinophilic, loosely arranged matrix.

TREATMENT & PROGNOSIS:
• AOT is completely benign: because of its capsule, it enucleated easily from the bonc
• Aggressive behavior has not been documented.
• Recurrence after enucleation seldom, if ever, occurs.
REFERENCES:
• Shafer’s Textbook of Oral Pathology (6th Edition).
• Textbook of Oral Pathology, Neville (3rd Edition).
• Manual of Oral Histology & Oral Pathology, Maji Jose.
- Hackdentistry/youtube.com