Deep bite has traditionally been explained using the interincisal angle—but is that really the most reliable predictor? Houston’s 1989 study in the European Journal of Orthodontics challenges this long-held belief and introduces a more clinically meaningful parameter: the edge–centroid relationship.
The Traditional View
For decades, orthodontists have associated increased overbite with a larger interincisal angle, especially in Class II Division 2 malocclusions. The logic is straightforward: retroclined incisors create a steep incisal guidance, promoting deeper vertical overlap.
Several studies supported this:
- Popovich (1955): r=0.73
- Ludwig (1967): r=0.52
- Backlund (1960): r≈0.57
However, Houston highlights an important limitation: even in the best-case scenario, the interincisal angle explains less than one-third of the variation in overbite.
The New Perspective: Edge–Centroid Relationship
Houston proposes a more comprehensive variable:
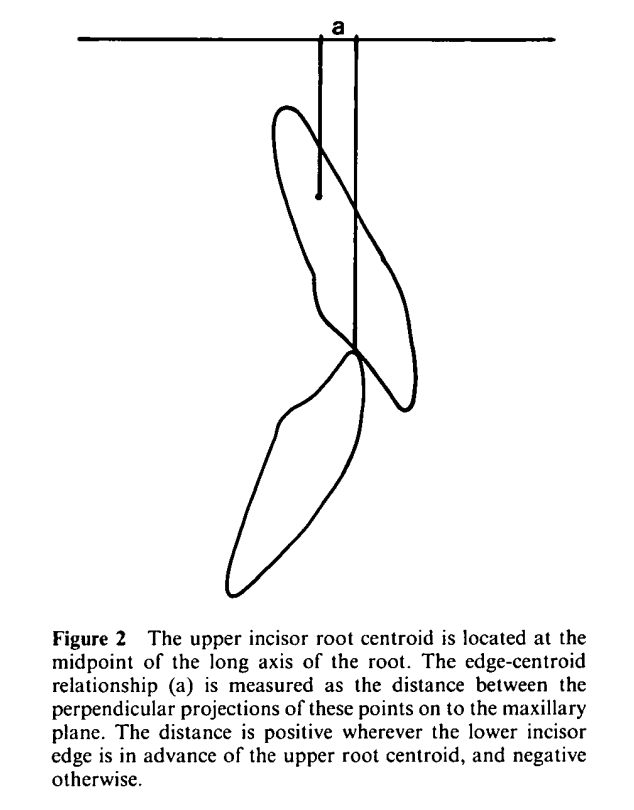
- The horizontal distance between:
- Lower incisor edge
- Upper incisor root centroid (midpoint of root axis)
Measured along the maxillary plane:
- Positive: Lower incisor edge is ahead of centroid
- Negative: Lower incisor edge is behind centroid
Key Findings
- Strongest correlation with overbite was found in Class II Division 2 cases:
- Interincisal angle: r=0.53, r2=0.28
- Edge–centroid relationship: r=−0.78, r2=0.61
- Once edge–centroid was accounted for:
- Interincisal angle had no independent effect (partial r=−0.01)
Why This Matters Clinically
The edge–centroid relationship integrates:
- Apical base relationship (skeletal pattern)
- Lower incisor inclination
- Functional occlusal positioning
This makes it far more relevant for:
- Diagnosis
- Treatment planning
- Stability prediction
Clinical Application
1. Class II Division 1 Cases
- If lower incisor edge is already 1–3 mm ahead of centroid:
- Simple upper incisor retraction may be sufficient
- Good stability expected
2. Class II Division 2 Cases
- Lower incisor edge typically lies posterior to centroid
- Requires correction for stable deep bite reduction
Options:
- Lower incisor proclination (limited stability unless growth-supported)
- Upper incisor palatal root torque (technically demanding)
- Combination approach (most realistic)
3. Stability Considerations
- For extrusion-based bite opening:
- Aim for centroid at least 2 mm behind lower incisor edge
- Prevents relapse via incisal “slippage”
- For intrusion-based correction:
- Less stringent requirement, as eruption forces are better controlled
A Simple Clinical Insight
Think of it this way:
Two patients may have identical interincisal angles—but very different overbites.
Why?
Because what truly determines vertical overlap is not just how teeth are inclined, but where they are positioned relative to each other in space.
Final Takeaway
Houston’s work shifts the focus from angular measurements to spatial relationships. The edge–centroid relationship is a more powerful and clinically actionable predictor of overbite depth and its stability—especially in Class II cases.
For exam answers, remember this line:
- Interincisal angle is a contributing factor, but edge–centroid relationship is the dominant determinant of overbite depth.

