- direct structural and functional connection between the implants and the bone.
- [ hemidesmosomes like structures, no CT insertion, no Sharpey’s fibers ] – the first cell to contact the implant is osteoblast
- It’s normal to have up to 2 mm of bone resorption around the neck of the implant in the first year.
- Implants only have a periosteal blood supply
- No innervation & no proprioception
- Since implants do not have CT [ no shock absorption ] – if there is any traumatic occlusion or excessive force it will lead to bone resorption [ cervically] or the implant might mechanically fail.
garden gatekeeper
I have a little garden of affection, where I feel affection for anyone who steps into that garden. I will be loyal to them, help them if they need it, devote time and attention to them. This garden is (mostly) unconditional; it does not decide who within it gets its fruits, or if they’re worthy enough to eat; the only requirement is to be in the garden.
But my garden has the gatekeeper, who decides who to let into the garden. I might see someone who doesn’t have their shit together, who needs a lot of emotional labor, who might cause me a lot of pain, who I will struggle to understand, and know that I could love and care for them.
The question is not if I have a garden that would accept them, but rather if I want to let them into my garden. My gatekeeper is cold and brutal. It checks how many resources my garden has, how many people are in there already, how sustainable it is. It evaluates potential entries on concrete facts – how emotionally mature are they, how intelligent? How much power do they have? Are they socially strategic to be associated with? Will they increase your garden capacity to hold others in the future?
And so, right now my choices around who new to allow into my garden is associated mainly with an unflattering calculating strategy. My life is a chess game, and these players are the potential pieces.
This is particularly true with my life right now; I’m looking at potential mates as strategic moves. Really I suspect this is what I was doing all along, and likely what many other people are doing, it was just much more subconscious before.
But the gatekeeper itself is not allowed in the garden; once in the garden, the newcomers are free from evaluation. If they drop in power, if they stop helping me, if they start absorbing way more emotional energy, then in my garden they remain; doused in affection and unconditionally accepted.
My garden carries many powerless people from earlier places in my life, or from high-proximity adventures, or people who came in attached to someone else who my gatekeeper wanted more. I am not evaluating them, my love for them is not dependent on what they can offer me; they simply reside in my heart. I have no regrets about this and it’s not an issue for me that my gatekeeper might continue to reject people similar to them.
(also to be clear, the garden analogy isn’t perfect and I’m oversimplifying; people don’t always stay in my garden forever, it’s not exactly binary if you’re in/out of the garden, there are different garden levels, and I don’t think literally everybody would be automatically and unconditionally drowned in affection once they got past the gatekeeper)
Histopathology of Dentinal caries
- As the carious lesion invades dentin, dentinal tubules become involved.
- As dentin is part of the dentin pulp complex, it leads to reparative dentine formation.
FIVE PATHOLOGICAL ZONES
- Zone 1: Zone of fatty degeneration of Tomes fibers.
- Starts at pulp
- No fat degeneration (misnomer name)
- Alteration by dentin by fat deposition leads to impermeability of tubules which leads to sclerosis
- Sclerosis is reaction between vital pulp and vital dentin
- It is the calcification of tubules against further penetration of microorganisms.
- Zone 2: Zone of dentinal sclerosis characterized by deposition of calcium salts in dentinal tubules.
- Sclerotic zone is minimum in rapidly advancing caries and prominent in slow/chronic caries.
- This is a translucent zone due to the vital reaction of odontoblasts
- High mineral content
- Reflected Light: Appears Dark
- Transparent Light: Appears White
- Zone 3: Zone of Decalcification of dentin
- Tubules are made of pure microorganisms such as pioneer bacteria (Cocci and Bacilli etc)
- Intertubular matrix is mainly affected by waves of acid produced by bacteria in the zone of bacterial invasion
- Initial decalcification occurs in the wall of tubules.
- Softened infected dentin cannot be differentiated with sterile soft dentine, clinically.
- Appears yellow-brown
- Zone 4: Zone of bacterial invasion of decalcified but intact dentin.
- Bacteria multiply within dentinal tubules.
- Acidogenic microorganisms: Seen in early caries
- Proteolytic organisms—predominate in deeper layers
- It supports the hypothesis that initiation and progression are two distinct processes and must be differentiated
- Zone 5: Zone of decomposed dentin.
- Bacteria invade both peritubular and intertubular dentin. Hence, Little architecture of dentin remains
- Liquefaction foci of miller enlarge and increase in number.
- Transverse Clefts: Perpendicular to tubules
- Acute Caries: necrotic dentin is very soft and yellowish-white
- Chronic Cases: Dentin is leathery and brownish-black
SUGAR SUBSTITUTES
- Xylitol
- its 5 carbon sugar
- comes from birch trees.
- preferential binding to Mutans strep but it cant ferment xylitol to acid
- Hence, no decrease in pH
- Sorbitol = caloric sweetness
- Aspartans = non caloric sweetener = 4Kcal/g = 200 times sweeter than sugar
Caries activity tests
- Lactobacillus Count Test
- It was introduced by Hadley in 1933.
- It estimates the number of bacteria in the patient’s saliva by counting the number of colonies appearing on tomato Peptone Agar at ph 5
- Interpretation of caries activity
- Immune: less than 1000
- Slight: 1000 – 5000
- Medium: I5000 – 10,000
- High: more than 10000.
- Snyder Test 2m
- The rapidity of acid formation by cariogenic bacteria
- Stimulated saliva + Glucose in Agar Medium containing bacto peptone, sodium chloride, and bromocresol green
- Dye changes from blue-green to yellow
- Interpretation of color change with caries activity
- High—24 hours
- Medium— 48 hours
- Slight—72 hours
- Immune—no color change
- Streptococcus mutans Level in Saliva
- The number S.Mutans colonies per ml of saliva is indicative of caries activity.
- Saliva samples obtained by using tongue blades are incubated on MSB agar (Mitis Salivarius Bacitracin Agar).
- Buffer Capacity Test
- The test evaluated the quantity of acid required to lower the pH of saliva using an arbitrary pH interval
- Buffering Capacity is inversely proportional to the process of caries
- Swab Test
- Oral swab- the buccal surface of teeth and placing it in Snyder media.
- This is incubated for 48 hours and the pH changes are read and correlated with caries activity.
- Fosdick Calcium Dissolution Test
- Patient saliva is mixed with glucose and powdered enamel
- Measuring of powdered enamel dissolved in 4 hours by acid formed
- This is not a single test and requires trained personnel
- Reductase Test
- Measures the activity of salivary enzyme reductase.
- Stimulated Saliva + diazo resorcinol, which colors the saliva blue.
- The change in color from blue to red is measured after 30 seconds – 15 minutes and this is taken as a measure of caries activity.
- Interpretation
- Non-Conducive: Remains blue after 15 minutes
- Slightly conducive: Orchid after 15 minutes
- Moderately conducive: Red after 15 minutes
- Highly conducive: immediately to red
- Extremely conducive: Changes to pink or white
EARLY CHILDHOOD CARIES
DEFINITION = American Academy of Paediatric Dentistry (AAPD) defines early childhood caries as ‘the presence of one or more decayed (non-cavitated or cavitated lesions), missing (due to caries) or filled tooth surfaces in any primary tooth in a child 71 months of age or younger.
A window of infectivity 2M**:
- Caufield (1996) stated that there is a window of infectivity between 19 and 33 months during which teeth get infected with S. mutans
- The most beneficial time for vaccination against dental caries would be in infancy before the eruption of teeth.
- This would promote the induction of adherence inhibiting salivary IgA thus delaying colonization of S. mutans.
- With the establishment of early colonizers, there would be a synergistic effect of suppressing the colonization of S.mutans during the period of the window of infectivity.
- A booster dose of vaccination may be required at the time of eruption of first permanent molars
ETIOLOGY AND PATHOGENESIS 3M
- Early colonization of MS is the most imp risk factor for developing ECC – MS transmission can be through the mother or from peers [ other kids]
- MS Colonization of pre dentate children is mostly associated with maternal factors [ high level of MS in the mother, poor OH, and active caries ]
- How is nocturnal bottle feeding/breastfeeding related to ECC?
- When a child is laid to rest, the bottle or breast nipple rests against the palate and the tongue covers the lower incisors [ that’s why they are not affected] –
- As the child becomes sleepy, saliva flow and swallow reflex are reduced
- Sugar remains stagnant around the neck of the teeth
- what practices increase the chance of developing ECC?
- Prolonged nighttime bottle feeding
- On-demand breastfeeding after the age of 1
- Frequent snacking with sugary foods
- Frequent sipping of sugary drinks throughout the day
CLINICAL FEATURES 2M
- ECC = also known as nursing bottle caries, baby bottle tooth decay
- Seen in infants and preschool children [ below the age of 6
- Demineralization at the necks of the upper incisors – mandibular incisors are not affected
- Decay pattern:
- Maxilla: incisors, canines, first molars
- Mandible: canines, first molars
- Lesion progresses to the necks of the teeth and in advanced cases, only a root stump is left
- Why does ECC follow this specific pattern?
- Chronology of primary tooth eruption
- Duration of the deleterious habit [ bottle feeding]
- A muscular pattern of infant sucking
- STAGES
- Very mild: slight demineralization usually at the gingival crest and no cavitation.
- Mild: demineralization in a gingival third of tooth and moderate cavitation.
- Moderate: frank cavitation on multiple tooth surfaces.
- Severe: Widespread destruction of tooth and loss of the clinical crown
MANAGEMENT 6M
- Identify the cause and stop the habit
- Give parental instruction on proper oral hygiene measures + diet counseling
- Decide if the case can be managed in the clinic [ with regular LA or nitrous sedation ] or the child needs GA
- If the case is treated in the clinic: full assessment of all affected teeth to know
- which teeth can be restored
- which need pulp therapy
- which need extractions
| First visit | Second visit | Third visit |
| Immediate excavation of caries followed by temporization Dietary chart Caries activity doneTopical fluoride application doneParent counselling | Examine diet chart Caries activity done again Replace any temporary restoration with permanent restoration | Pulpul procedures Extractions Space maintersRecall the pt every 3 months |
What instructions would you give the parents to a child with ECC?
- STOP NIGHT TIME BOTTLE FEEDING / stop breastfeeding at will after the first tooth erupts
- Feed the child while being held + burp the infant after feeding
- Clean the teeth after each feeding [ wipe the teeth with a wet gauze]
- regularly lift the upper lip to check for signs of demineralization of the upper Interiors
- OH should start with the eruption of the first tooth – wipe the teeth with gauze and for ages 2- 6 brush with low fluoride tooth past [ 400-500 ppm] – parental supervision until the child can properly spit
- Children are encouraged to drink from a cup as they become 1 year old
- Avoid frequent snacking and have regular meals instead
- First dental visit should be combined with immunization dates [ at or before 6 months]
Prevention of ECC ideally begins prenatally:
- give the mother information about diet and OH
- treat the mother’s own oral diseases and lower MS count by mouth rinses and restorative care
- educate the mother on modes of transmission of MS [ don’t lick spoons or pacifiers etc..]
DENTAL HYGIENE & NCDs
Stainless Steel Crowns #pedodontics

Classification of Dental Caries
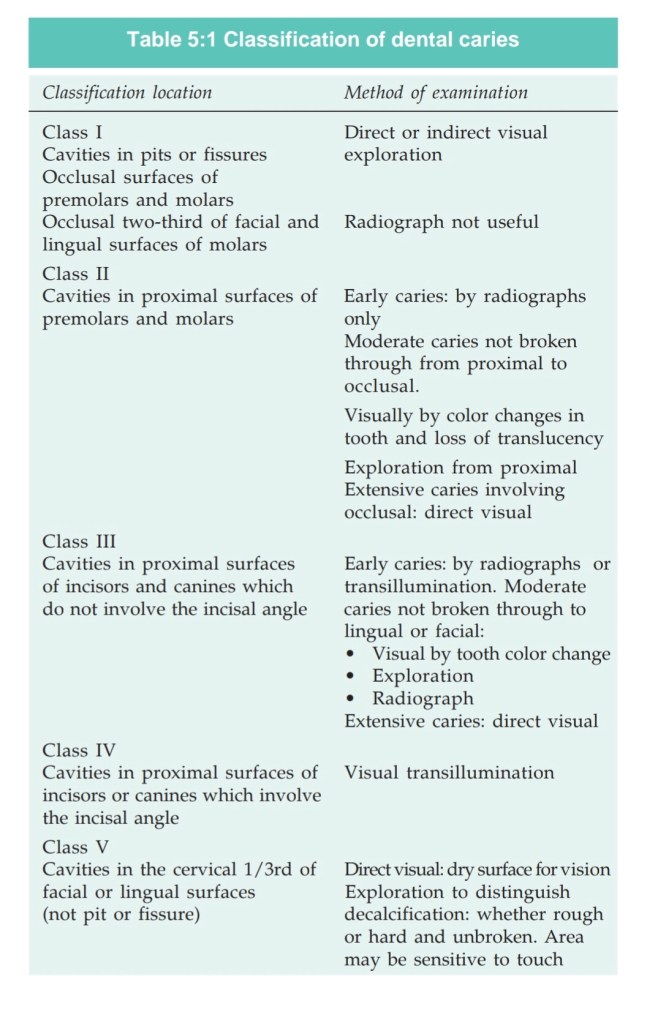
© 2008, Jaypee Brothers Medical Publishers
WHITE SPONGE NEVUS
References-Ghoms Textbook of oral medicine 2nd edition
