- Seen in Microdontia
- Seen in Congenital syphilis = also called hutchinson incisors

ELEPHANTIASIS GINGIVA
- Seen in Hereditary fibromatosis gingivae
- Pseduoedentiliusm is present = overgrown gingiva covers the crowns of tooth making it look like edentulism

COBBLESTONE APPEARANCE
- Heck’s disease/focal epithelial hyperplasia
- Multiple squamous papillomas, papules, nodules
- HPV – type 13 and 32
- Pysotomatitis Vegetans
- Inflammatory stomatitis associated with inflammatory bowel disease
- Crohn’s disease
- Ulcerative Colitis
- Cereberiform tongue
- This is also seen MC in pemphigus Vegetans and less likely in Scrotal tongue
- Fissured Tongue
- Seen in scrotal tongue
- Also called plicated tongue
- Etiology = suffering from stress/ hereditary
- Associated with Merkelsson Rosenthal syndrome = Triad of
- Facial paralysis
- Cheilitis Granulomatosa
- Fissured tongue
- Darrier’s disease





GHOST TEETH
- Large sized pulp chambers
- Thin enamel and dentin
- Also called, Regional Odontodysplasia
- Also called odontogenesis imperfecta
- Also called odontogenic dysplasia
- H/P
- UNMINERALIZED DENTIN quantity is more
- Wide predentin zone
- Large areas of interglobular dentin
- Presence of enameloid conglomerates
- Calcification seen in REE of unerupted teeth
- UNMINERALIZED DENTIN quantity is more


DENTIN DYSPLASIA TYPE 2
- Coronal type
- Abnormally large sized pulp chambers = THISTLE TUBE APPEARANCE of pulp chambers



DENTIN DYSPLASIA TYPE 1
- Extremely short roots
- Obliteration of Pulp chambers with osteodentin
- Osteodentin – histologically looks like
- Cascades of dentin = one layer of dentin forms, it stops and then new layer of dentin forms on top of it
- Lava flowing around boulders
- Cascades of dentin = one layer of dentin forms, it stops and then new layer of dentin forms on top of it
- Few pulpal remnants are left behind – crescent shaped pulpal remnants



DENTINOGENESIS IMPERFECTA
- Not associated with osteogenesis imperfecta
- Mutation in gene – DSPP – dentin sialo phospho protein
- DSPP located on chromosome number 4
- Revised shield classification
- Common traits seen in both types
- Flat DEJ line
- Gene = DSSP
- Common traits seen in both types
| Type 1 Opalescent dentin type | Type 2 Brandy white type |
 Bulbous crowns are seen With cervical constriction Giving tulip shaped crownsWHY? Because of atypical dentin formation = obliteration of pulp chambers |  Large sized pulp chambers Very thin dentin – hence, radiographically SHELL TEETH |
Radiographic Interpretation of Ameloblastoma 4m*** 2m**
-
- Slow growing = identified late
- Initially, pt has asymptomatic symptoms
- Later develops swelling due to buccolingual expansion and come to dentist
- Unilateral
- Mandible = posterior = Ramus/body = mc
- If it occurs in anterior region = desmoplastic type = aggressive and resembles fibro osseous lesion
- 20% of cases seen in maxilla = can involve sinus
- Epicenter = odontogenic in origin = above IAC
- Size = large, diffuse
- Borders = well defined
- Internal structure =
- Multilocular
- septa are small and round = honeycomb appearance
- Septa are large and round = soap bubble appearance
- Septa are curved and round
- Displace IAC inferiorly
- Root resorption = Knife edge resorption
- Lower border of mandible = thin egg shell appearance due to aggressive expansion
RADIOLUCENT LESIONS OF JAWS #9M #NTRUHS
- Acute periapical abscess
- Swelling
- Vertical pain = tenderness on percussion
- Vestibular tenderness and obliteration = pathognomonic sign
- Widening of PDL = Only feature. It takes time for r/g features to develop, by that time acute has been converted into chronic
- Chronic Periapical abscess
- Carious tooth
- Sinus tract = pus will come out
- Hence, there will be a breach in the continuity of lamina dura
- Diffuse, ill-defined radiolucency surrounding root apex
- Periapical Granuloma
- Granuloma is made up of granulation tissue. It is formed due to new vascularizations.
- May or maynot be corticated
- Size is less than 1.5 cm in diameter
- Well defined
- Periapical cyst
- Well defined
- Surrounding corticated or sclerotic border
- Size is more than 1.5 cm
- Infected Cyst
- Partially well defined
- Corticated border = evident only in few areas
- PERIAPICAL CEMENTAL DYSPLASIA 2M*
- Site = mandibular anteriors
- Teeth = vital
- Multifocal
- Appearing as periapical radiolucency
- RL = initial stage
- Mixed = intermediate stage
- RO = mature stage
- Phoenix abscess
- Acute exacerbated phases of chronic periapical abscess
- Pt complains that Every 6 months, swelling and pain
- Pulp is non vital
- Lateral periodontal Cyst






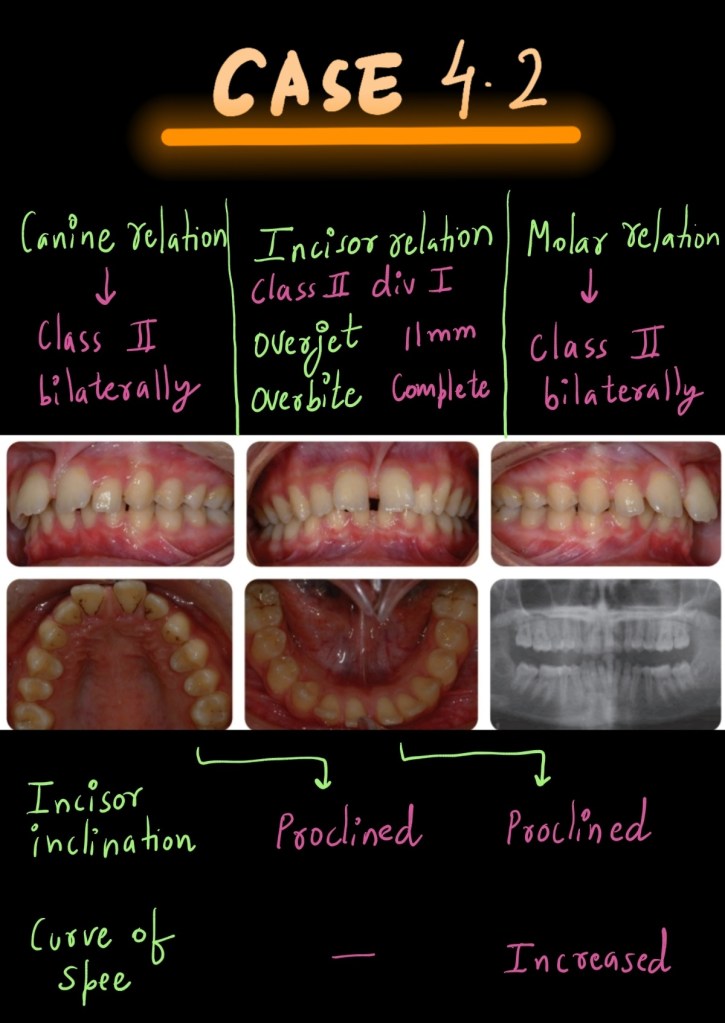
Ortho Case 4.2
An 11-year-old female presented with a class II division 1 malocclusion on a moderate skeletal class II pattern with reduced vertical dimensions complicated by an increased overjet (11mm), increased overbite, generalized spacing and bi-maxillary proclination.
The aetiology of this malocclusion is multi-factorial.
The moderate skeletal class II discrepancy resulted in an increased overjet and class II molar relationship. The overjet was exacerbated by the presence of a lower lip trap. The generalized spacing was a result of an underlying dento-alveolar disproportion. This was compounded by bi-maxillary proclination, which arose due to resting soft tissue pressures and dento-alveolar compensation.
TREATMENT PLAN
• Integration of twin block functional and sectional lower fixed Herbst appliancee
• Continuation of functional appliance wear at night
only
• Use of headgear
• Inter-arch class II elastic traction following fixed
appliance placement
The prognosis for long-term stability of class II correction is good in this case, as the new maxillary incisor position will be controlled by the lower lip following the achievement of lip competence.
