Muhad Noorman P, Final year Student – Team Dentowesome
Scoring good and better marks are always priority of any student irrespective of their level and class . Hard work and smart work helps to score good marks.
Some tips to study smart and score more marks
1) Always organise yourself, Neverprocrastinate. Don’t think about wasted days ,look forward days ahead and make efficient planning.
2) Give importance to every subject equally, start with easy and end in hard nuts.
3) Identify your best time, and place to study. Ignore and never seek how you’re peer group works. Always your peer lies about studies, focus on yourself 🙂
4) Cut your social distraction, even though it sounds like a rocket science, regular practice helps to cut your Distraction. Utilise focus mode in android phones, Install Forest app. It Helps to prioritise your study hours.
5) Teach yourself as if you’re a teacher, trust me you’ll crack a million topics.
6) Teach you’re peer group , it’ll help to recollect and brush up your brain.
7) Regularly shift your studyplace , between a period of 1 hour or 2 hour later, brain and mind always rejects learning from a same environment.
8) Get familiarise with the exam layout, use previous year question, understand nature of questions , prepare accordingly.
9) Always finish with previous questions first and if time allows study other topic left, mentioned in University syllabus.
10) Reading a book not studying : Revise topic after 1 or 2 hour, Prepare notes, put away books . Attempt topic as an exam question. Self realization is best methodology to improve yourself.
11) Never cut too many corners: Often we get devastated listening rumors , predictable questions . And the truth is anything can come.
12) Practice mock exams during free times. Practice always make a man perfect.
13) Organize your answer while writing in exam papers. Never forget, Presentation matters. Include as much as figures, flowcharts, pie diagrams..etc.. Proove examiner you have an edge over topics. Underline important points with seperate ink.
14) Last but not least get an adequatesleep.(Ideally 6 to 7 hours) Give some time for your brain and hippocampus to process your memory.
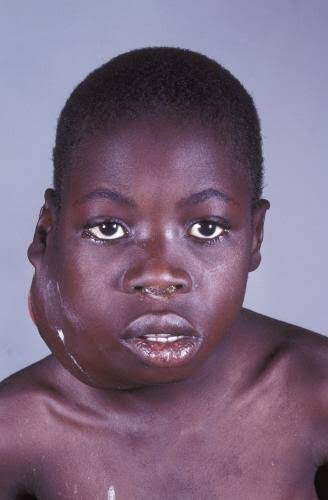
It is also called as ‘African jaw lymphoma’. It is a lymphoreticular cell malignancy. In the African form jaw involvement is 75% and in cases of the American form, abdomen involvement is more common. It is a B-cell neoplasm.
Etiology
• Epstein-Barrvirus(EBV)which also causes nasopharyn- geal carcinoma and infectious mononucleosis is considered to be the etiological factor. There are higher EBV antibody levels in patients of Burkitt’s lymphoma.
Clinical Features
Age and sex—peak incidence is in children between 6to 9 years. Males are affected more commonly than the females, with a ratio of 2:1.
Site distribution—more are found in maxilla than in mandible, where it may spread rapidly to the floor of the orbit. Almost always occurs in molar area. In the African form, more than one quadrant is involved while in the American form, only one quadrant is involved.
Onsetandprogress—the most important hall mark of this tumor is the fast growth with a tumor doubling time of less than 24 hours.
Symptoms—the most common presenting features are swelling of the jaws, abdomen and paraplegia. It is painless.
Sign—peripheral lymphadenopathy is common.
Prognosis—it is rapidly fatal in the absence of treatment,with death occurring within 6 months.
Oral Manifestations
• Onset and extent—it begins generally as a rapidly growing tumor mass of the jaws, destroying the bone with extension to involve maxillary, ethmoid and sphenoid sinus as well as orbit.
Symptoms—loosening or mobility of permanent teeth.There is gross distortion of the face due to swelling. Paresthesia and anesthesia of inferior alveolar canal or other sensory facial nerves are common.
Signs—gingiva and mucosa adjacent to the affected teeth become swollen, ulcerated and necrotic. As the tumor mass increases, the teeth are pushed out of their sockets. Swelling of the jaw occurs and it may cause facial asymmetry. They are capable of blocking nasal passages, displacing orbital contents and eroding through skin. There is derangement of arch and occlusion. There may be large quantity of mass protruding into the mouth, on the surface of which may be seen rootless, developing permanent teeth.
Spread—once the tumor perforate the bone, it is initially confined by the periosteum, but subsequently it spreads to the soft tissues of the oral cavity and face where rapid tumor growth soon obliterates the entire face and skin becomes tense and shiny.
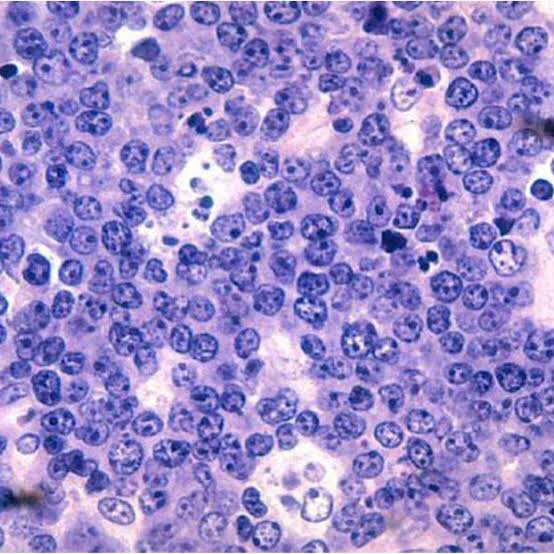
Histology
Shows characteristic starry sky appearance.
Radiographic Features
Motheatenappearance—small radiolucent foci scattered throughout the affected area. These small foci coalesce and form a multilocular moth eaten appearance.
Sunray appearance—if periosteum is elevated, it will produce sunray appearance.
Margins—margins are ill defined and non-corticated.
Shape—they expand rapidly and are ballooned shaped.
Teeth—Lesions are osteolytic with loss of lamina dura about the erupted teeth and crypts of developing teeth are enlarged.
Effect ons urrounding structures—they expand very rapidly and breach its outer cortical limits.
Diagnosis
• Clinical diagnosis—swelling of the jaw and abdomen with peripheral lymphadenopathy can give clue to the diagnosis.
• Radiological diagnosis—moth eaten appearance is seen with loss of lamina dura around the teeth.
• Laboratorydiagnosis—monotonous sea of un differentiated monomorphic lymphoreticular cells, usually showing abundant mitotic activity. There is also hyperchro- matosis and loss of cohesiveness. Characteristic ‘starry sky’ appearance is seen.
Management
• Cytotoxicdrugs—cytotoxicdrugs like cyclophosphamide 40 mg/kg in single IV administration and repeated about 2 weeks later. Vincristine and methotrexate have been successful in some cases.
• Multiagent chemotherapy—combination of drugs such as cyclophosphamide, vincristine and methotrexate give better results than any single drug. Majority of patients show dramatic response to the therapy. The swelling regresses and the displaced teeth return to their normal position within 1 to 2 weeks.
REFERENCE- SHAFER’S TEXTBOOK OF ORAL PATHOLOGY AND ANIL GHOM TEXTBOOK OF ORAL MEDICINE
These are incorporated into the deeper layers of enamel and dentin during odontogenesis and alter the development and appearance of the enamel and dentin
.Alkaptonuria: Dark brown pigmentation of primary teeth is commonly seen in alkaptonuria. It is an autosomal recessive disorder resulting into complete oxidation of tyrosine and phenylalanine causing increased level of homogentisic acid.
Hematological disorders
• Erythroblastosis fetalis: It is a blood disorder of neonates due to Rh incompatibility. In this, stain does not involve teeth or portions of teeth developing after cessation of hemolysis shortly after birth. Stain is usually green, brown or bluish in color.
• Congenital porphyria: It is an inborn error of por- phyrin metabolism, characterized by overproduction of uroporphyrin. Deciduous and permanent teeth may show a red or brownish discoloration. Under ultraviolet light, teeth show red fluorescence.
• Sickle cell anemia: It is inherited blood dyscrasia characterized by increased hemolysis of red blood cells. In sickle cell anemia infrequently the stains of the teeth are similar to those of erythroblastosis fetalis, but discoloration is more severe, involves both dentitions and does not resolve with time.
Amelogenesis imperfecta: It comprises of a group of conditions, that demonstrate developmental alteration in the structure of the enamel in the absence of a systemic disorders. Amelogenesis imperfecta (AI) has been classified mainly into hypoplastic, hypocalcified and hypomaturation type.
Fluorosis: In fluorosis, staining is due to excessive fluoride uptake during development of enamel. Excess fluoride induces a metabolic change in ameloblast and the resultant enamel has a defective matrix and an irregular, hypomineralized structure
Vitamin D deficiency results in characteristic white patch hypoplasia in teeth.
Vitamin C deficiency together with vitamin A deficiency during formative periods of dentition resulting in pitting type appearance of teeth.
Childhood illnesses during odontogenesis, such as exanthematous fevers, malnutrition, metabolic disorder, etc. also affect teeth.
Dentinogenesis imperfecta : It is an autosomal dominant development disturbance of the dentin which occurs along or in conjunction with amelogenesis imperfecta. Color of teeth in dentinogenesis imperfecta (DI) varies from gray to brownish violet to yellowish brown with a characteristic usual translucent or opalescent hue.
Tetracycline and minocycline: Unsightly dis- coloration of both dentitions results from excessive intake of tetracycline and minocycline during the development of teeth. Chelation of tetracycline molecule with calcium in hydroxyapatite crystals forms tetracycline orthophosphate which is responsible for discolored teeth.
Posteruptive Causes
Pulpal changes: Pulp necrosis usually results from bacterial, mechanical or chemical irritation to pulp. In this disintegration products enter dentinal tubules and cause discoloration.
Trauma: Accidental injury to tooth can cause pulpal and enamel degenerative changes that may alter color of teeth.Pulpal hemorrhage leads to grayish discoloration and nonvital appearance. Injury causes hemorrhage which results in lysis of RBCs and liberation of iron sulfide which enter dentinal tubules and discolor surrounding tooth.
Dentin hypercalcification: Dentin hypercalcification results when there are excessive irregular elements in the pulp chamber and canal walls. It causes decrease in translucency and yellowish or yellow brown discoloration of the teeth.
Dental caries: In general, teeth present a discolored appearance around areas of bacterial stagnation and leaking restorations.
Restorative materials and dental procedures: Discoloration can also result from the use of endodontic sealers and restorative materials.
Aging: Color changes in teeth with age result from surface and subsurface changes. Age related discoloration are because of:– Enamel changes: Both thinning and texture changes occur in enamel.
– Dentin deposition: Secondary and tertiary dentin deposits, pulp stones cause changes in the color of teeth.
• Functional and parafunctional changes: Tooth wear may give a darker appearance to the teeth because of loss of tooth surface and exposure of dentin which is yellower and is susceptible to color changes by absorption of oral fluids and deposition of reparative dentin.
Extrinsic Stains
Daily Acquired Stains
Plaque: Pellicle and plaque on tooth surface gives rise to yellowish appearance of teeth.
Food and beverages: Tea, coffee, red wine, curry and colas if taken in excess cause discoloration.
Tobacco use results in brown to black appearance of teeth.
Poor oral hygiene manifests as:
– Green stain
– Brown stain
– Orange stain.
Swimmer’s calculus: – It is yellow to dark brown stain present on facial andlingual surfaces of anterior teeth. It occurs due toprolonged exposure to pool water.
Gingival hemorrhage.
Chemicals
• Chlorhexidine stain: The stains produced by use of chlorhexidine are yellowish brown to brownish in nature.
Metallic stains: These are caused by metals and metallic salts introduced into oral cavity in metal containing dust inhaled by industry workers or through orally administered drugs.
Stains caused by different metals
• Copper dust—green stain • Iron dust—brown stain • Mercury—greenish black stain • Nickel—green stain • Silver—black stain.
Reference- Nisha garg textbook of endosontics and Anil Ghom textbook of oral medicine
Contrast resolution is the ability to distinguish different densities in the radiographic image.
Current digital detectors capture data at 8-, 10-, 12-, or 16-bit depths.
The bit depth is a power of 2.
Spatial Resolution
Spatial resolution is the capacity for distinguishing fine detail.
The theoretical limit of resolution is a function of picture element (pixel) size for digital imaging systems.
Film based IOPA – 20 lp / mm.
Digital receptors 7 lp / mm.
Film > CCD > PSP
Detector Latitude
It is the ability of the image receptor to capture a range of x-ray exposures as different densities.
The latitude ofCCD and CMOS detectors is similar to film
Photostimulable phosphor receptors have larger latitudes and have a linear response to five orders of magnitude of x-ray exposure.
Detector Sensitivity
Sensitivity of a detector is its ability to respond to small amounts of radiation. Intraoral film sensitivity is classified according to speed.
High resolution CCD and CMOS systems achieve less dose reduction than lower resolution PSP systems. CCD and PSP systems or extraoral imaging require exposures similar to those needed for 200-speed screen-film systems.
SLE is a multisystem autoimmune inflammatory disorder of unknown etiology.
Main feature is the formation of antibodies to DNA, which may initiate immune complex reactions, in particular a vasculitis.
Female to male ratio of 9:1
More common in persons of non-European descent.
Etiology
Geneticpredisposition—relativeofpatientshavehigher incidences of auto-antibodies, immune deficiency and connective tissue disease. This tendency is greatest among identical twins.
Immunological abnormality possibly mediated by viral infection—immune complex consisting chiefly of nucleic acid and antibody account for majority of the tissue changes.
Autoimmune disease—as these patients develop antibodies to many of their own cells.
Endocrine—thereishighincidenceinfemalesinpreg- nancy. This finding suggestive of increased estrogen level.
Biochemicalincreaseinexcretionofmetabolicproducts, particularly tyrosine and phenylalanine, in certain SLEpatient.
CLINICAL MANIFESTATIONS
Lupus is known as “the great mimic.”
Skin lesions of lupus can be classified
lupus-specific (having diagnostic clinical or histopathologic features)
nonspecific lesions.
Three subtypes of lupus-specific
Acute
subacute
chronic.
Acute cutaneous lupus occurs in 30 to 50% of patients and is classically represented by the butterfly rash-mask-shaped erythematous eruption involving the malar areas and bridge of the nose
Chronic cutaneous lupus occurs in 15 to 20% of cases and affects the skin of the face or scalp in about 80% of cases.
The least common subtype, subacute cutaneous lupus, occurs in 10 to 15% of patients and includes papulosquamous (psoriasiform) and annular-polycystic eruptions, usually on the trunk and arms.
Nonspecific but suggestive skin manifestations of lupus are common and include
alopecia (both scarring following discoid lesions and non-scarring)
Photosensitivity
Raynaud’s phenomenon
Urticaria
Erythema
Telangiectases
cutaneous vasculitis.
ORAL MANIFESTATIONS
Two predominant types of oral lesions are
discoid lesions
ulcerations.
Oral ulcerations associated with SLE they occur with increased frequency on the palate and in the oropharynx and are characteristically painless.
Histologically, they are characterized by lymphocytic infiltrate at the base of the ulcer and in the perivascular distribution, which is similar to that observed in discoid lesions.
Discoid oral lesions, appear as whitish striae frequently radiating from the central erythematous area, giving a so-called “brush border.”
Buccal mucosa, gingiva, and labial mucosa are the most commonly affected intraoral sites.
Direct immunofluorescent staining for immunoglobulins and complement C3 factor is a useful aid to diagnosis. Granular deposition of IgM, IgG, and C3 along the basement membrane is characteristic
Diagnosis
• Clinical diagnosis—skin lesion with lesion present on oral mucosa which is atrophic and erythematous will suspect lupus erythematous. Oral and nasopharyngeal ulceration is major diagnostic criteria for SLE.
Laboratory diagnosis—L.E. cell inclusion phenomenon with surrounding pale nuclear mass apparently devoid of lymphocytes. Anemia, leukopenia and thrombocyto- penia, with sedimentation rate increased. Serum gamma globulin increased and Coomb’s test is positive.
Positive lupus band test—it shows deposition of IgG,IgM or complement component in skin.
Differential Diagnosis
Lichenplanus—homogenouspicture,nodarkerythema and no telangiectasia. Mucosal changes are usually extensive and symmetrical.
Lichenoidreaction—historyofdrugisalwaysthere.
Ectopic geographic tongue—systemic manifestation present is lupus erythematous, which is absent in ectopicgeographic tongue.
Psoriasis—Auspitz’s’signispositive.
Electrogalvanic lesion—dissimilar restorations are seenin oral cavity.
Leukoplakiaanderythroplakia—lesionstendtomaintainsame appearance and there are no skin changes.
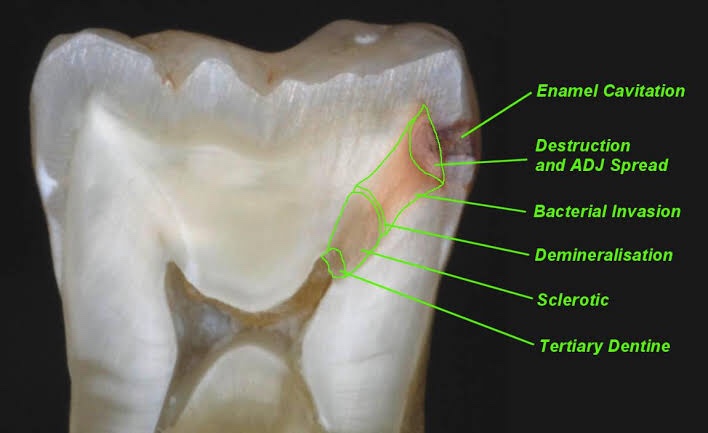
Zone I: Zone of fatty degeneration of odontoblast process Zone 2: Zone of dentinal sclerosis characterized by deposition of cal- cium salts in dentinal tubules Zone 3: Zone of decalcification of dentin, a narrow zone, preceding bacterial invasion Zone 4: Zone of bacterial invasion of decalcified but intact dentin Zone 5: Zone of decomposed dentin
Early dentinal caries
Fatty degeneration of odontob/ast process
>Disposition of fat globules – precedes early sclerotic changes >Special stains – Sudan red >Significance- 1.Fat contributes to impermeability
2.Predisposing factor for dental sclerosis
Sclerotic dentin
>Reaction of vital pulp – calcification of dentinal tubules (DT)
>Seals off DT from further penetration of microorganisms
>Minimal in rapidly advancing caries
>Prominent in slow caries
>Sclerotic dentin – appear white in transmitted light
Decalcification of dentinal tubules
>Above dentinal sclerosis – zone of decalcification
>Occurs in advance of bacterial invasion of DT
>Pioneer bacteria >The initial decalcification – only the walls of DT
>Study of tubules- pure form of microorganisms
Zone of microbial invasion
>Proteolytic organisms – predominantly in deeper layers Acidogenic microorganisms – more in early caries >Supporting the hypothesis that initiation and progression are two distinct processes and must be differentiated
Advanced dentinal caries
>Decalcification of the walls of DT – confluence
>Thickening of sheath of Neumann – along its course • Increase in the diameter of DT – microorganisms
>Focal coalescence of adjacent tubules and ovoid area of destruction- liquefaction foci >Acidogenic organisms – initial decalcification
>Proteolytic organisms – matrix destruction
>Multiple areas of destruction>Necrotic mass of dentin (leathery consistency)
>Formation of transverse cleftsExtend at right angles to DT and parallel contour line
>Peeling away of carious dentin
REFERENCE- Shafers textbook of oral pathology 8th edition
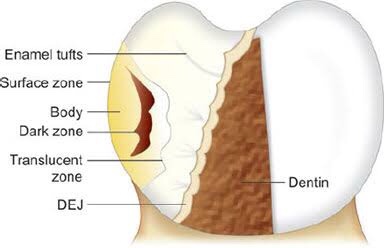
Four zones are clearly distinguishable, starting from the inner advancing front of the lesion. These are the (1) translucent zone, (2) dark zone, (3) body of the lesion and (4) surface layer.
Zones of enamel caries Translucent zone {TZ)
First recognizable zone of alteration
Advancing front of the lesion
Half the lesions demonstrate TZ, not always present
Seen in longitudinal ground sections in clearing (quinoline – RI – 1.62)
TZ appears structureless
Pore volume – I% (compared to 0.1 % of sound enamel)
Dark zone
Lies adjacent and superficial to the translucent zone Positive zone
Shows positive birefringence (in contrast to sound enamel.
Pore volume of 2-4% (polarized light) Presence of small pores; large molecules of quinoline are unable to penetrate Micropore system – gets filled with air and becomes dark Medium like water may penetrate
Body of the lesion
Between unaffected, surface and dark zone Area of greatest demineralization Pore volume – 5% in periphery and 25% in centre Quinoline imbibition – body appears transparent Water imbibition – positive birefringence compared to sound enamel Striae of Retzius – prominent
Surface zone
Quantitative studies – partial demineralization of 1-10% • Pore volume – less than 5% of the spaces
Negative birefringence – water imbibition
Positive birefringence – porous subsurface All the four zones of enamel caries cannot be seen with same immersion medium.
REFERENCE – Shafers textbook of oral pathology 8th edition
The term “juvenile periodontitis” was introduced by Chaput and colleagues in 1967 and by Butler in 1969. In 1971, Baer definedit as “a disease of the periodontium occurring in an otherwise healthy adolescent which is characterized by a rapid loss of alveolar bone about more than one tooth of the permanent dentition.
• Usually affecting persons under 30 years of age (however, may be older).
• Generalized proximal attachment loss affecting at least three teeth other than first molars and incisors.
• Pronounced episodic nature of periodontal destruction. • Poor serum antibody response to infecting agents.
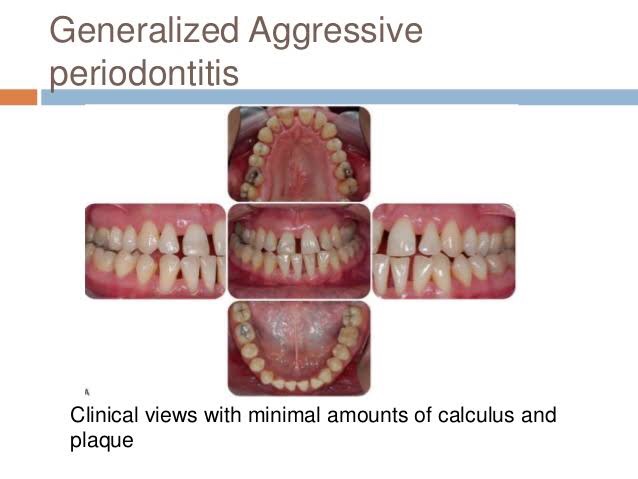
Clinical Characteristics
GAP usually affects individuals under age 30, but older patients also may be affected. In contrast to LAP, evidence suggests that individuals affected with GAP produce a poor antibody response to the pathogens present.
Clinically, GAP is characterized by “gen- eralized interproximal attachment loss affecting at least three per- manent teeth other than first molars and incisors.”The destruction appears to occur episodically, with periods of advanced destruction followed by stages of quiescence of variable length (weeks to months or years).
P. gingivalis, A. actinomycetemcomitans, and Tannerella forsythia (formerly Bacteroides forsythus) frequently are detected in the plaque that is present.
Two gingival tissue responses can be found in cases of GAP. One is a severe, acutely inflamed tissue, often proliferating, ulcerated, and fiery red. One is a severe, acutely inflamed tissue, often proliferating, ulcerated, and fiery red.
Bleeding may occur spontaneously or with slight stimulation. Suppuration may be an important feature. This tissue response is believed to occur in the destructive stage, in which attachment and bone are actively lost.
Some patients with GAP may have systemic manifestations, such as weight loss, mental depression, and general malaise.
Radiographic Findings
No definite pattern of distribution occurs, The radiographic picture in GAP can range from severe bone loss associated with the minimal number of teeth to advanced bone loss affecting the majority of teeth in the dentition.
Prevalence and Distribution by Age and Gender
A US national survey of adolescents ages 14 to 17 reported that 0.13% had GAP. In addition, blacks were at much higher risk than whites for all forms of aggressive periodontitis, and male teenagers were more likely to have GAP than female adolescents.
Treatment of aggressive periodontitis
• Successful treatment of EOP depends on early diagnosis use of antibiotics against the infecting micro organisms and provision of an infection free environment for healing
• EOP both localized and generalized types includes surgery and use of tetracyclines (Lindhe 1982, Christersson and Zambon 1993)
• T/T of GAP – often less predictable – alternative antibiotics directed to specific pathogenic flora require
– Multidisplinary approach combines clinical labroartory evaluation with conventional periodontal therapeutic methods for diagnosis and t/t of GAP
The term “juvenile periodontitis” was introduced by Chaput and colleagues in 1967 and by Butler in 1969. In 1971, Baer defined it as “a disease of the periodontium occurring in an otherwise healthy adolescent which is characterized by a rapid loss of alveolar bone about more than one tooth of the permanent dentition.
According to Hart et al. diagnosis of localized early-onset periodontitis is based on
• attachment loss of > or equal 4 mm on at least two permanent first molars
and incisors (one of which must be a first permanent molar)
Not more than two other permanent teeth, which are not first permanent molars or incisors, should be affected
• Bone loss around primary teeth can be early finding in LAP
Clinical Characteristics
The lack of clinical inflammation despite the presence of deep periodontal pockets and advanced bone loss .
The amount of plaque on the affected teeth is minimal, which seems inconsistent with the amount of periodontal destruction present.The plaque that is present forms a thin biofilm on the teeth and rarely mineralizes to form calculus.
The rate of bone loss is about three to four times faster than in chronic periodontitis.
Other clinical features of LAP may include (1) distolabial migration of the maxillary incisors with concomitant diastema formation, (2) increasing mobility of the maxillary and mandibular incisors and first molars, (3) sensitivity of denuded root surfaces to thermal and tactile stimuli, and (4) deep, dull, radiating pain during mastication, probably caused by irritation of the supporting structures by mobile teeth and impacted food.
Radiographic Findings
Vertical loss of alveolar bone around the first molars and incisors, beginning around puberty in otherwise healthy teenagers, is a classic diagnostic sign of LAP. Radiographic findings may include an “arcshaped loss of alveolar bone extending from the distal surface of the second premolar to the mesial surface of the second molar”
Prevalence and Distribution by Age and Gender
LAP affects both males and females and is seen most frequently in the period between puberty and 20 years of age.
RISK FACTORS FOR AGGRESSIVE PERIODONTITIS
Microbiologic Factors
A. actinomycetemcomitans, Capnocytophagaspp., Eikenella corrodens, Prevotella intermedia, and Campylobacter rectus), A. actinomycetemcomitans has been implicated as the primary pathogen associated with LAP.
Immunologic Factors
Some immune defects have been implicated in the pathogenesis of aggressive periodontitis. The human leukocyte antigens (HLAs), which regulate immune responses, have been evaluated as candidate markers for aggressive periodontitis.
Genetic Factors
Familial pattern of alveolar bone loss and have implicated genetic factors in aggressive periodontitis.
Environmental Factors
The amount and duration of smoking are important variables that can influence the extent of destruction seen in young adults.46 Patients with GAP who smoke have more affected teeth and more loss of clinical attachment than nonsmoking patients with GAP.16 However, smoking may not have the same impact on attachment levels in younger patients with LAP.
Treatment
In ps with LAP,
Aa organisms penetrate into crevicular epithelium T/T with antibiotic alone such as 2 week course of doxycycline reduce Aa organisms
Surgical removal of infected crevicular epithelium and debridement of root surface during surgery while the patient is on a 14 day course of doxycycline hyclate (1gm per day) (Mandell and Sockaransky 1988, Saxen et al 1990).
Microdentex manufacturers the DMDx(Microdentex, FORT MYERS, Florida) test, a DNA test kit for establisting the risk of aggressive periodontits and confirms whether the child has responded favorably to the use of antimicrobial therapy Retesting after 4-6 weeks after the completion of antibiotic therapy determines the pts response to t/t
• Rams and collagues described keyes technique for treating LAP Scaling and root planning of all teeth , with irrigation to probing depth of saturated inorganic salt solutions and 1% chloramine T.((sodium para-toluene sulfonchloramide) In addition recommended administration of systemic tetracycline (18 per day) for 14 days This dose appropriate for pts 12 yrs of age and older
Home T/T Daily application of paste of sodium bicarbonate and 3% hydrogen peroxide and inorganic salt irrigation.










 Spatial Resolution
Spatial Resolution