Written by : Dr.Urusa I Inamdar
The importance is to determine deviation of jaw from the midline during the opening and closing of the jaws.
Causes of jaw deviation:
- Traumatic injuries of the joint
- Infection of the jaw
- Fractures of the jaw
- Muscular hypertrophy and hypotrophy
The lateral mandibular range of motion or movement is assessed ” Normal 8 to 10 mm ” by having the patient to occlude the teeth and then slide the jaw in both directions. The range of movement from midline and any pain, location and severity is recorded.
Maximum interincisal opening: As a general guide, mobility is considered to be reduced if the subject is unable to open his or her jaw to the width of two fingers ( <30 mm ).
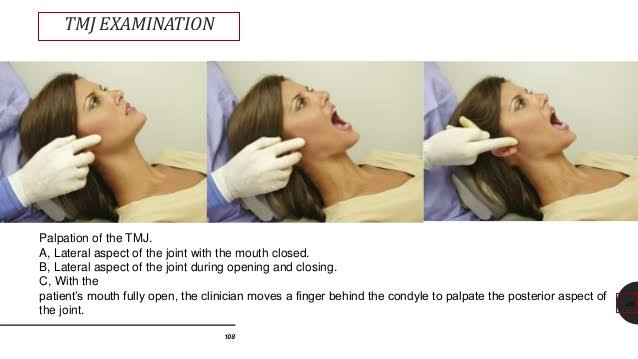
Palpation
- Bimanual and bidigital Palpation or extra-auricular or intra-auricular.
- Palpation may reveal pain and irregularities during condylar movement , described as clicking or crepitus. Clicking reveals the internal derangement of TMJ.
- The lateral pole of condyle is most accessible for palpation during mandibular movements.
- Palpation just anterior and posterior to the lateral pole detects pain associated with TMJ capsular ligament.
- The comparison between both condyles must be assessed by palpation.
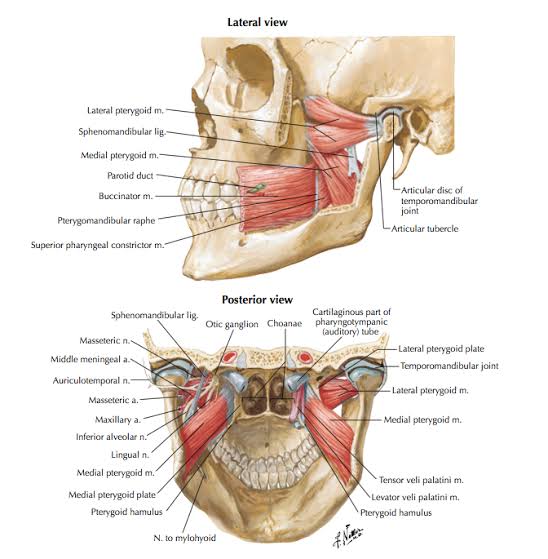
TMJ muscles :
Gravity muscles ( Depression of mandible )
- Geniohyoid
- Digastric
- Mylohyoid
Anti-gravity muscles ( Elevation of mandible )
- Medial , oblique , anterior , vertical of temporalis.
- Medial Pterygoid , masseter .
Protrusion of mandible
- Medial pterygoid.
- Lateral pterygoid.
TMJ disorders :
Developmental
- Hypoplasia/aplasia of condyle
- Hyperplasia of condyle
- Bifid condyle
Traumatic
- Dislocation of condyle
- Fracture of condyle
- Injury to articular disc
Inflammatory
- Osteoarthritis
- Rheumatoid arthritis
- Septic arthritis
Neoplastic
References:
- A practical manual of Public Health Dentistry – C M Marya
- Slide share – Diagnosis of Temporomandibular disorder- Kelly
- TMJ Anatomy – Geeky medics