Cigarettes contain nicotine and by smoking regularly and for long hours, your body becomes dependent on it. Giving up smoking can cause nicotine withdrawal symptoms which are :
- Restlessness ,impatience
- Eating more than usual
- Anxiety / tension
- Headaches,irritability / anger
- Difficulty in concentration + Depression
- Loss of energy,dizziness
- Sweating
- Insomnia
- Stomach or bowel problems
- Heart palpitations
- Tremors
- Craving for tobacco
Stop smoking medicines along with nicotine replacement therapy are effective aid to tobacco cessation & can help control these symptoms.
What are these?
3 types –
- Champix tablets (varenicline)
- Zyban tablets (bupropion)
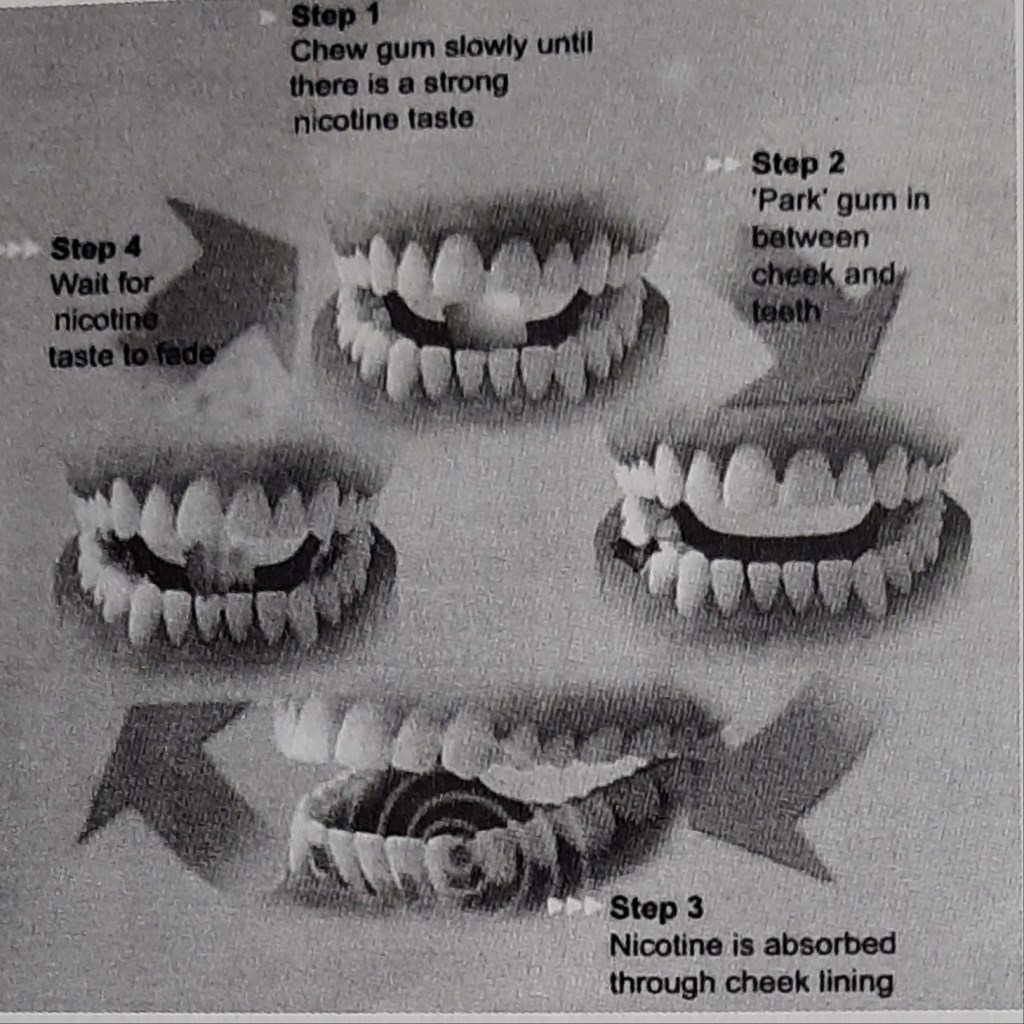
- Nicotine replacement therapies (gums,patches,lozenges,microtabs,sublingual tablets,insulators,cigs,nasal sprays)

How does it work?
Tobacco intakers who are motivated to quit the habit & are dependent on nicotine should be offered NRT.
- Prescribed for 6 to 8 weeks,in blocks of up to 2 weeks,contingent on continued abstinence.
- If one type of NRT is not working for the patient ,the health professional is advised to prescribe a suitable type informing about the dosage & maximum amount to take a day.

Is it safe?
NRT is safe because of the facts that the nicotine levels are low and it’s less addictive delivery mechanism (unlike smoking tobacco where the nicotine reaches the brain quickly) and also because most of the harmful problems are caused by the other components of tobacco smoke ,not by the nicotine.
NRT is safe for most adults and in people with stable cardiac diseases, but caution needed in unstable,acute cardiovascular disease,pregnancy,or breastfeeding or in those aged under 18 years.
Brownie points-reduces the constant urge to munch on food,thus reducing weight gain.😊
When should one stop using NRT?
Most courses of NRT recommend use for about 12 weeks.This is because it takes this much time for the brain to adjust to working without the high doses of nicotine that the cigarettes supply.However there is no hard and fast rule.After starting the therapy,most people mistake the lack of discomfort for the belief that the addiction is over,leading to stop using the product too soon. This can result only in reappearing of the symptoms.
The best method is to take the help of the health professional when you start the therapy and keep them updated about the progress.
Lastly ,we all are not the same….each tobacco smoker’s tendency & pattern to quit may vary & it depends on different factors like age,gender,environment, general physical and mental health.
Sources:S.S Hiremath textbook of preventive and community dentistry, http://www.healthunlocked.com(Quit Support)