Def:- Fibrous dysplasia is an uncommon nonhereditary, developmental anomaly of the bone due to a defect in osteoblastic differentiation and maturation.
HISTOPATHOLOGY:
Microscopic finding of fibrous dysplasia show irregularly shaped trabeculae of immature (woven) bone in a cellular, loosely arranged fibrous stroma.
The bone trabeculae are not connected to each other . They often assume curvilinear shapes.
which have been likened to CHINESE script writing.
The bone trabeculae are considered to arise by metaplasia and are not surrounded by plum appositional osteoblasta.
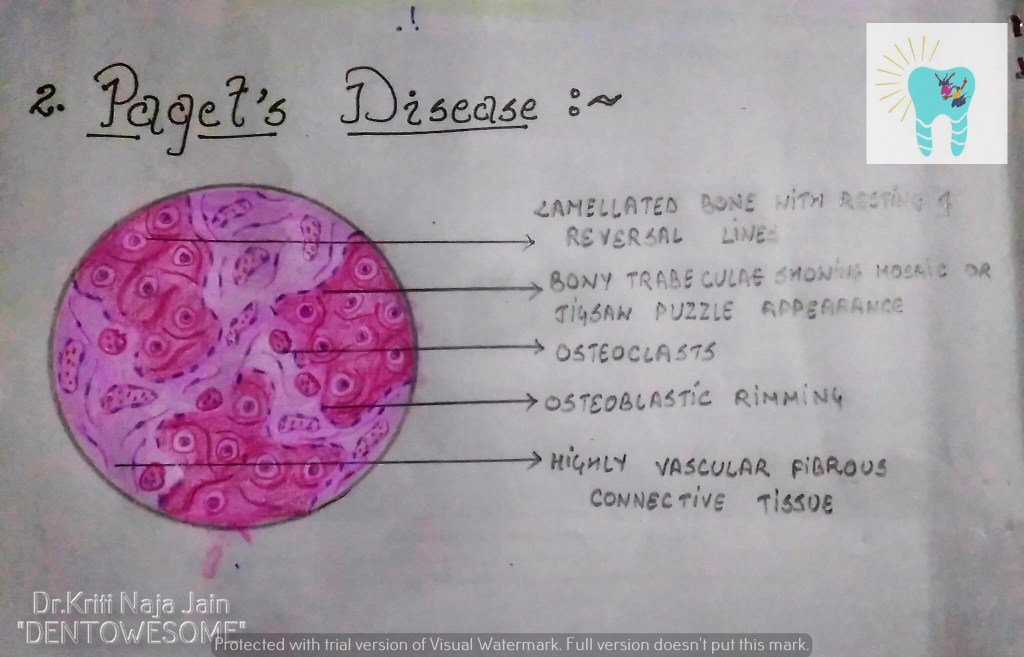
2. PAGET’S DISEASE (OSTEITIS DEFORMANS):-
Def:- Paget’s disease of bone is a condition characterized by abnormal and anarchic resorption and deposition of bone, resulting in distortion and weakening of the affected bones.
HISTOPATHOLOGY:-
Microscopic examination shows an apparent uncontrolled alternating resorption and formation of bone.
in the active resorption stages, numerous osteoclasts surround bone trabeculae and show evidence of resorption activity.
Simultaneously ,osteoclastic activity is seen with formation of osteoid rims around bone trabeculae .
A highly vascular fibrous C.T. replaces the marrow .
A characteristic microscopic feature is the presence of basophilic reversal lines in the bone.
These lines indicate the junction between alternating resorptive and formative phase of the bone and result in a ” JIGSAW PUZZLE” or “MOSAIC” appearance of the bone.
In the less active phases ,large masses of dense bone showing prominent reversal lines are present.
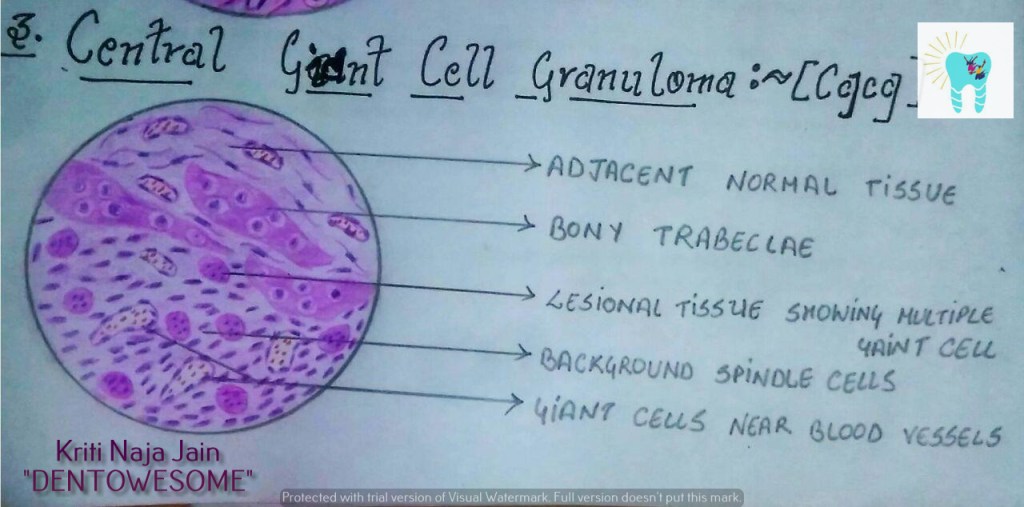
3. CENTRAL GAINT CELL GRANULOMA(GIANT CELL LESION; GIANT CELL TUMOR):-
Def :- Central giant cell granuloma (CGCG) is an uncommon, benign and proliferative lesion whose aetiology is not defined. Central giant cell granuloma is a relatively common benign intraosseous destructive giant cell lesion, which often affects the anterior part of the jawbone. By seeing clinical and radiographically , CGCG is divided into two types:-
1. Nonaggressive lesions make up most cases, exhibit few or no symptoms, demonstrate slow growth, and do not show cortical perforation or root resorption of teeth involved in the lesion. 2. Aggressive lesions are characterized by pain, rapid growth, cortical perforation, and root resorption. They show a marked tendency to recur after treatment, compared with the nonaggressive types.
HISTOPATHOLOGY:-
Lesional tissue is composed of highly cellular connective tissue stroma with numerous spindle shaped cells.
Multinucleated giant cells are distributed in this C.T.
Mesenchymal cells
Gaint cells are large with many nuclei upto 20 or more.
Gaint cells are usually aggregated close to the blood vessels.
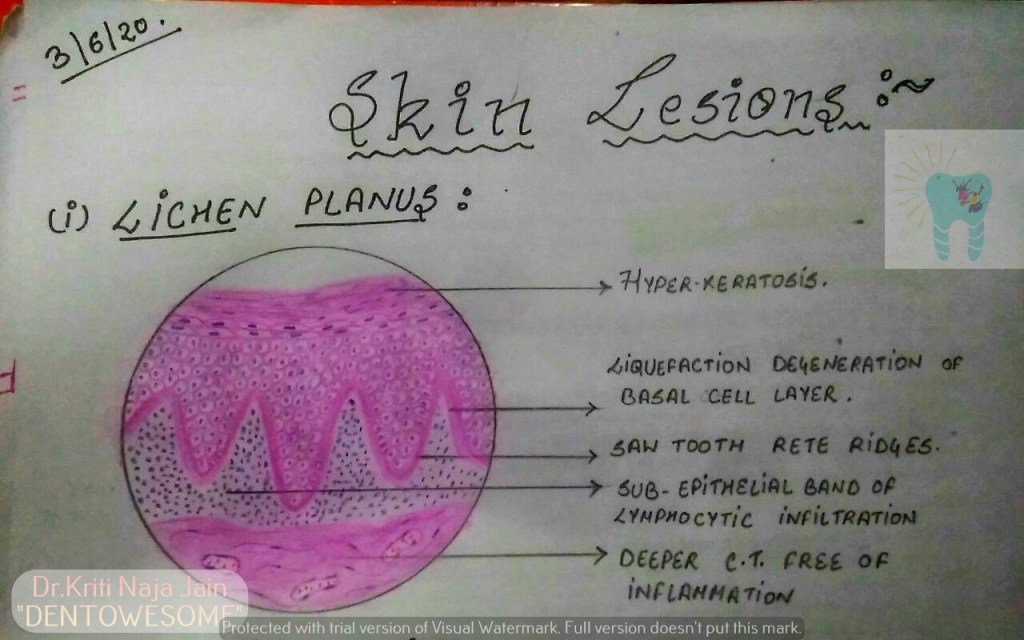
*Lichen planus is a chronic mucocutaneous disorder manifested in a various forms in the oral cavity.
*The most characteristic pattern is” RETICULAR TYPE” with the interlacing white stripe called “WICKHAM’S STRIAE”.
*HISTOPATHOLOGY:-
Histopathology FIRST DESCRIBED BY DUBRENILL 1906
later revised by Shklar in 1972
Hyper orthokeratinisation or hyper parakeratinisation
◦Thickening of granular layer
◦Acanthosis of spinous layer
◦Intercellular oedema in spinous layer
◦“ Saw-tooth” rete pegs
◦Liquefaction necrosis of basal layer- Max Joseph spaces
◦Civatte ( hyaline or cytoid) bodies
◦Juxta epithelial band of inflammatory cells
◦An eosinophilic band may be seen just beneath the basement membrane and represent fibrin covering lamina propria.
2.PEMPHIGUS :-
Pmphigus is a tissue specific autoimmune disease affecting the skin and mucosa. Clinical manifestations is in the from of “vesiculobullous lesions” that rupture to form ulcer and erosions .
*Vesiculobullous lesions develop due to immune mediated acantholysis causing intraepithelial vesicle formation.
*HISTOPATHOLOGY :-
Formation of the vesicle or bullae within the epithelium that often results in a supra-basilar spilt or separation. • Following this suprabasilar spilt in the epithelium, the basal cell layer remains attached to the lamina propria, and it often appears as a row-of-tomb stones. • Loss of intercellular bridges and collection of edema fluid result in acantolysis within the spinus cell layer, which causes disruption of the prickle cells. • As a result of acantholysis, clumps of large hyperchromatic epithelial cells desquamate that are often seen lying free within the vesicular fluid, these desquamated cells are often rounded and smooth in appearance and are known as “Tzanck cells”.
Small number of polymorphonuclear neutrophil (PMN) and lymphocytes may be found within the vesicular fluid, but there is minimum inflammatory cell infiltration in the underlying connective tissue (unlike any other vesiculobullous lesion).
3.PEMPHIGOID :-
Pemphigoid is a vesiculobullous lesions that develop due to an autoimmune reaction directed against some components of basement membrane.
*This results in seperation of epithelium from the connective tissue with sub epithelial vesicles formation .
*Bullous pemphigoid and cicatricial pemphigoid are two different types of pemphigoid lesions.
*HISTOPATHOLOGY:-
The inflammatory infiltrate is typically polymorphous, with an eosinophilic predominance.
Mast cells and basophils may be prominent early in the disease course.
Electron microscope shows basement membrane attached to the connective tissue rather than overlying separated epithelium.
Bence Jones protein in urine – Also seen in leukemia, polycythemia
⬆️ ESR
⬆️ Alkaline phosphatase
Hyperuricemia
🔹Histological Features:
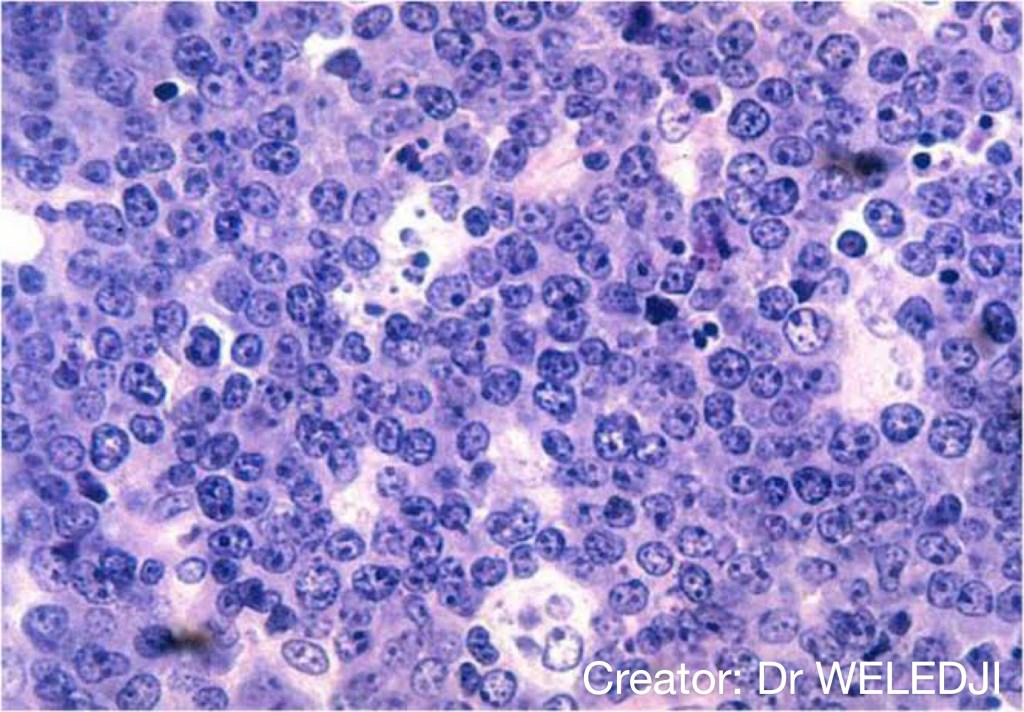
1. Cells are closely packed in large sheets..👇🏻
Round/Ovoid
Nuclei – eccentric placed
Chromatin clumping in a cart wheel/checkerboard pattern
Perinuclear halo (Golgi complexes)
2. Russell bodies: Russell bodies are multiple round cytoplasmic hyaline inclusions that are frequently seen in bone marrow aspirates in myeloma. They are composed of immunoglobulin molecules within vesicular structures derived from rough endoplasmic reticulum. Plasma cells containing them are sometimes referred to as Mott cells.
Many are dematiaceous, aka, pigmented fungi. – It is thought that the melanin in their cells contributes to virulence.
Many are dimorphic, which means they exist in both hyphal and yeast forms.
Reside in soil, on plants, and decaying vegetation.
Trauma to the skin introduces pathogenic fungi to the underlying tissues. – Thus, infections tend to occur on the extremities, especially the feet and hands, which are likely to be inoculated during gardening or field work.
Chronic, granulomatous lesions in the skin and deeper tissue. – Often, histopathologic samples will show Splendore-Heoppliphenomenon, aka, asteroid bodies, which are characterized by eosinophilic materials radiating from the microorganisms.
Initial lesion occurs at the site of inoculation, for example, in the skin of the feet – Then spreads to deeper tissues, which can include the lymphatics, muscles, and connective tissues.
Rarely disseminate to other organs.
Long-term antifungals can be used to treat some subcutaneous mycoses.
Lymphocutaneous sporotrichosis “Rose Gardener’s Disease” – Many individuals are inoculated via rose thorns.
The fungi most often responsible are members of the Sporothrix schenckii complex.
Mycosis manifests as linear cutaneous nodules and ulcers that begin at the site of inoculation and travel along the path of the draining lymphatics. – In some patients, the lesions will become suppurative; the discharged pus contains fungi that is useful for diagnostic purposes.
Chromoblastomycosis Chromomycosis
Caused by a variety of fungi – Fonsecae, Cladosporium, Phialophora, etc.
Histopathologic samples show characteristic Medlar bodies (aka, sclerotic bodies or muriform cells). – Medlar bodies are cells with transverse septa and thick, pigmented cell walls; some liken them to copper pennies. In the sample, we can see some Medlar bodies within a giant cell.
Chromoblastomycosis produces slowly developing, chronic lesions that can cause progressive tissue fibrosis. – Lesion morphology varies; for example, some patients have warty or “cauliflower-like” nodules, while others develop plaques with central scarring.
Mild cases where warty nodules are involved may be cured by excision.
However, excision is not practical in patients with extensive lesions, as we see in the example of plaques; thus, long-term antifungals are the preferred treatment in such cases.
Eumycotic Mycetoma Madura foot or Maduramycosis
Caused by Madurella mycetomatis and other fungi.
Because mycetoma is also caused by bacteria, it’s important to culture samples from the patient to rule out actinomycetemycetoma, which requires a different intervention.
Eumycotic mycetoma is characterized by painless nodules that progress to ulcers; the ulcers discharge fluid and granules. – Granules comprise the fungal hyphae – The color of the granule is indicative of the microorganism type M. mycetomatis granules are dark brownish-black.
Eumycotic mycetoma is a chronic and progressive condition,and new sinuses form as older sinuses heal.
The draining sinuses produce swelling and tissue deformity;infection can ultimately invade and destroy deeper tissues.
Unfortunately, eumycotic mycetoma often responds poorly to antifungal treatments, so amputation is often necessary to prevent further destruction.
Subcutaneous Entomophthoromycosis
Conidiobolus coronatus
Conidiobolomycosis most commonly affects adults.
Inhalation produces infection in the nasal and paranasal sinuses.
Swelling and deformity of the nose and upper lip can be quite dramatic, though relatively painless.
Basidiobolus ranarum
Basidiobolomycosis more commonly affects male children.
Produces “rubbery” dark lesions on the buttocks, thighs, and shoulders. – Gastrointestinal involvement is possible, though rare.
Subcutaneous Phaeohyphomycosis
Various species – Exophiala, Bipolaris, Curvalaria, etc.
Histopathologic samples are characterized by irregular hyphae.
Basidiomycota – Specifically, species of Malassezia, which are yeast that colonize the superficial layers of the skin and hair.
Because they do not invade or destroy living tissues, they generally do not trigger an immune response.
Infections common in warm, moist environments.
Ascomycota Dermatophytes are fungal pathogens that can invade the skin and cause dermatophytoses, such as ringworm. – Dermatophytic species come from three genera: Trichophyton, Epidermophyton, and Microsporum. – These molds infect keratin of the skin, hair, and nails; because they cause damage to the tissues, they trigger an immune response. – These fungi cause mycoses called tineas, aka, ringworm Are acquired from contact with infected soil, animals, or other humans.
Laboratory diagnosis
KOH (potassium hydroxide) testing, in which skin scrapings and KOH are viewed under microscope.
Calcofluor white stain is also used to detect fungi in samples. – Fluorescent stain with affinity for the chitin in fungal cell walls.
Treatments
When necessary, treatments for superficial and cutaneous mycoses involves topical and/oral antifungals, in addition to good hygiene.
Mycoses
Pityriasis versicolor Sometimes called tinea versicolor
Caused by species of the Malassezia genus. – In the microscopic image we can see Malassezia cells and some short hyphae; some authors describe their appearance as looking like “spaghetti and meatballs.”
Young adults in warm, moist environments are most likely to develop pityriasis versicolor.
Fungi are spread via human to human contact.
Lesions appear as either hypo- or hyper-pigmented, and typically appear on the upper body, face, and neck.
Tinea nigra is caused by the fungus Hortaea werneckii
In the microscopic image, we can see septate hyphae and budding cells.
Tinea nigra is most common in children and young adults in tropical and subtropical climates.
Manifests as patches of small dark dots, typically on the palms of the hands and soles of the feet.
White piedra (piedra means “stone”) is caused by species of Trichosporon, which are yeasts that colonize the hair shaft.
Individuals in tropical and subtropical areas are most likely to have white piedra.
Manifests as soft white or cream-colored nodules on the hair shafts.
Black piedra is caused by the yeast Piedra hortae, which colonizes the hair and scalp of individuals in tropical areas.
It produces firm dark nodules in the hair.
Tineas Commonly referred to as Ringworm.
Caused by dermatophytic fungi.
The tineas are named for their location on the body, as follows: – Tinea capitis develops on the scalp, especially of children, and is associated with alopecia, scaling, and cervical and suboccipital lymphadenopathy. – Tinea barbae is ringworm that occurs in areas of facial hair. – Tinea corporis is ringworm that appears on the trunk or extremities; it produces red rings with scaly skin and is pruritic (itchy). – Tinea cruris, aka, jock itch, is most common in adolescent and young males; it produces a rash on the upper thighs, but typically does not involve the scrotum. – Tinea pedis, aka, athlete’s foot, can involve all aspects of the feet: Interdigital is the most common, and involves the skin between the toes Moccasin tinea pedis is chronic and involves the sides and soles of the feet Vesicular tinea pedis is characterized by inflammation with vesicles and lesions – Tinea unguium is a fungal infection of the nails (thus, it is a type of onychomycosis).
Rickettsia prowazekii and Rickettsia typhi cause different forms of typhus
Orientia tsutsugamushi causes scrub typhus. to damage to the endothelial cells of blood vessels.
Anaplasmataceae
Ehrlichia chaffeensis causes human monocytic ehrlichiosis
Ehrlichia ewingii causes human ewingii ehrlichiosis
Anaplasma phagocytophilum causes human granulocytic anaplasmosis.
Coxiellaceae
Coxiella burnetti causes Q fever.
INFECTIONS, RESERVOIRS, AND VECTORS
Rickettsia rickettsii
Rocky Mountain Spotted Fever — Fever, headache, myalgias, and, sometimes, confusion (as a result of CNS involvement). — Patients commonly develop a macular rash that can progress to petechiae; the rash characteristically begins on the wrists and ankles, then spreads to the palms, soles, and trunk. This pattern of spread is a helpful distinguisher. — Gastrointestinal involvement is possible, and can cause abdominal pain, nausea, vomiting, and/or diarrhea. — Left untreated, disseminated vasculitis can lead to multi-organ failure.
Ticks and rodents are key reservoirs; hard ticks are vectors.
Rickettsia akari
Rickettsialpox — Typically less severe than Rocky Mountain Spotted Fever. — Patients experience fever and papulovesicular rash with eschars. Headaches and myalgia are possible. — Rodents are the reservoirs; mites are the vectors.
Rickettsia prowazekii
Epidemic typhus — Brill-Zinsser disease is the result of latent infection that manifests years, even decades, later. — Patients experience fever, headache, chills, myalgia, and a macular rash that spreads from the trunk to the extremities. — CNS involvement is possible, and can present as confusion. — If left untreated, vasculitis can lead to multi-organ failure. — Humans are the main reservoir, and the human body louse is the vector; be aware that flying squirrels and their fleas have also been described as reservoirs and vectors.
Rickettsii typhi
Endemic typhus (aka, murine, typhus) — Patients experience fever, headache, myalgia, and a maculopapular rash that spreads from the trunk to the extremities. — Gastrointestinal involvement is possible, and more common in children. — Cases are typically mild, but severe cases can lead to renal dysfunction or respiratory impairment (experienced as cough, dyspnea). — Small mammals, particularly cats and rodents, are key reservoirs; their fleas are the vectors.
Orientia tsutsugamushi
Scrub fever — Fever, intense headahces, mylagias, and a maculopapular rash that starts on the trunk; in some cases, eschars will form, especially at the site of inoculation. — Lymphadenopathy and pulmonary and neurologic involvement are common; gastrointestinal involvement may also occur. — Reservoirs include mites (chiggers) and rodents; mites are the vector.
Ehrlichia chaffeensis
Human monocytic ehrlichiosis — Fever, headache, and myalgia; Coughing is common in adults. — The rash associated with this infection varies, and is more common in children. — Central nervous system involvement is possible. — Leukopenia, thrombocytopenia, and elevated transanimases. — Deer, dogs, and other mammals are common reservoirs; soft ticks are the vector.
Anaplasma phagocytophilum
Granulocytic anaplasmosis — Similar symptoms and signs to human monocytic ehrlichiosis — Rash is rare. — Small mammals are the reservoirs; soft ticks are the vector.
Coxiella burnettii
Q fever — Fever, headache, and myalgia, but no rash. — Chronic Q fever can lead to serious complications, including hepatitis, pneumonia, and subacute endocarditis. — Reservoirs include mammals, ticks, and birds; though ticks are a potential vector, most cases of Q fever are the result of the aerosol inhalation or consumption of the bacteria in contaminated milk.
A heterogenous group of disorders that include disorders of Bone Growth (eg, achondroplasia).
Limb Malformations
Of the digit (suffix: -dactly)
Of the limbs (suffix: -melia)
BONE GROWTH: REVIEW
Typical long bone in a mature stage of endochondral ossification
We see the hyaline cartilaginous model (its template) and periosteal bone collar. -In the center, we draw the medullary cavity, which forms as the primary ossification center degenerates and remodels. It’s filled with hematopoetic marrow (which comprises red and white blood cell precursors) from vasculature that invades the cavity. -Secondary ossification centers lie in the epiphyses. -We include the epiphyseal growth plates and specify the direction of growth.
Epiphyseal growth plate zones
The reserve zone is filled with fetal hyaline cartilaginous cells.
The proliferative zone is filled with chrondrocytes that proliferate but do NOT hypertrophy.
The hypertrophic zone is filled with hypertrophic chondrocytes.
We show the zone of vascular invasion.
BONE REMODELING: REVIEW
Osteoprogenitor cells and Osteoblasts
We see an osteoprogenitor cell and an osteoblast on a slab of bone matrix (the inorganic component is hydroxyapatite and the organic component is osteoid).
Members of the (bone morphogenetic protein) BMP family and Transforming growth factor stimulate these cells to become osteoblasts.
Within a lacuna, lies an osteocyte.
Vitamin D and Parathyroid hormone (PTH) stimulate osteoblasts to secrete factors that promote osteoclastogenesis – the formation of osteoclasts.
Osteoblasts produce M-CSF (macrophage colony stimulating factor), which stimulates proliferation of monocytes, which later fuse into multinucleated PREosteoclasts (we’ll see that these nuclei can be as robust as 30 nuclei in a single osteoclast).
RANKL (an osteoprotegerin ligand) binds to the RANK receptor on the multinucleated osteoclast to stimulate differentiation from pre-osteoclast to osteoclast.
To regulate osteoclast differentiation, osteoblasts release osteoprotegerin, which binds RANKL and inhibits its binding to the RANK receptor.
Osteoclasts
Osteoclasts resorb bone.
They are dome-shaped with a ruffled border, and have a site of active bone resorption, the subosteoclast/Howship lacuna.
Actin fibers attach the edge of the cell to the bony surface, which forms the sealing (aka clear) zone of the osteoclast.
Cytoplasm contains: -Numerous nuclei. -Acidophilic vesicles, which are key to the osteoclasts ability to degrade bone – these vesicles release hydrogen ions into the subosteoclastic zone that can reduce the pH to as low as ~4.5 to solubilize mineralized bone.
The cytoplasm is also rich in mitochondria.
THE SKELETAL DYSPLASIAS
ACHONDROPLASIA
This is an ossification anomaly that manifests with short limbs.
Patients have short stature, pronounced lordosis, and bowed legs.
This is a more severe form of hypochondroplasia.
Systemic complications
Obstructive sleep apnea (OSA)
Recurrent otitis media
Neurologic manifestations
Macrocephaly
Spinal stenosis
Hydrocephalus
Genetics
Autosomal Dominant (80%) of patients have denovo mutations
FGRFR3 gene Mutation
Achondrogenesis
Think Achondroplasia but as a Lethal Skeletal Dysplasia — prenatally morbid or stillbirth.
MARFAN SYNDROME
Patients have abnormally long bones.
Systemic complications
Dislocated lens (ectopia lentis)
Aortic aneurysm and dissection
Mitral valve prolapse
Long, narrow face, with crowded teeth
Scoliosis or kyphosis
Neurologic manifestations
Dural ectasia
Spinal stenosis
Hydrocephalus
Genetics
Autosomal Dominant
FBN1 gene
Fibrillin-1 protein with mycrofibril abnormalities with decreased elasticity
Bone tumors (osteochondromas) form at the end of long bones and cause shortening of growth.
Systemic complications
Transformation from benign tumor to malignancy (sarcoma)
Neurologic manifestations
Direct nerve pressure
Genetics
EXT1 and EXT2 gene
Heparan sulfate is nonfunctional
Autosomal Dominant
ENCHONDROMATOSIS (AKA OLLIER’S SYNDROME)
Bone tumors form at the ends of long bones, near the growth plates, thus these patients generally have short stature.
Systemic complications
Transformation from benign tumor to malignancy (chondrosarcoma)
Genetics
Somatic (non-heritable)
IDH1 & IDH2 genes for isocitrate dehydrogenase 1 and isocitrate dehydrogenase 2
POLYOSTOTIC FIBROUS DYSPLASIA
Fibrous scar tissue develops in bones.
Mccune-Albright Syndrome
A genetic disorder that occurs in females, involves of polyostotic fibrous dysplasia and also multiple endocrinopathies that notably manifest with precocious puberty and café-au-lait spots.
Endocrinopathies in Mccune-Albright Syndrome
Precocious Puberty
Hyperthyroidism
Goiter
Acromegaly
Cushing’s syndrome (rare)
Dermatologic Manifestations
Café-au-lait spots
Genetics
GNAS gene for guanine nucleotide-binding protein (G-protein)
Musculoskeletal structures (muscles, tendons, ligaments) are replaced with bone (ossified). * This extra-skeletal ossification causes immobility, manifesting with difficulty even opening one’s mouth to eat or ability to breath.
Genetics
AVCR1 gene for BMP type 1 receptor
Autosomal Dominant
HEREDITARY HYPOPHOSPHATEMIC RICKETS
Patients suffer from a bowing of bones due to chronic hypophosphatemia (in adults, this causes osteomalacia – bone softening).
Pathophysiology
Hypophosphatemia
Genetics
PHEX gene
Most common: X-linked dominant
OSTEOPETROSIS
Bones are abnormally dense (thick).
Systemic complications
Anemia
Hepatosplenomegaly
Immunodeficiency
Neurologic manifestations
Cranial neuropathies
OSTEOPOIKILOSIS
Bones are spotted with round areas of increased bone density.
OSTEOGENESIS IMPERFECTA
Bones are abnormally fragile: fractures occur commonly.
Mild forms of the disease are associated with blue-appearing sclera.
Severe forms are lethal just after birth due to inability to adequately breathe.
Genetics
COL1A1 and COL1A2 genes (mostly)
Autosomal Dominant (mostly)
EHLERS-DANLOS
Causes hypermobile joints.
Systemic complications
Hypermobile joints
Elastic skin
Kyphoscoliosis
Respiratory changes from severe scoliotic abnormalities
Genetics
Autosomal recessive
CLEIDOCRANIAL DYSPLASIA
Manifests with abnormalities in the clavicles and skull [delayed closure of the fontanelles], most notably (hence its name).
These bones develop from intramembranous ossification, thus we can remember the disorder as one of pathologic intramembranous ossification.
Bony abnormalities
Clavicles
Skull
Teeth
Genetics
RUNX2 gene
Autosomal Dominant
Additional notable causes of skeletal dysplasia include:
Neurofibromatosis
Storage Disorders: Gaucher Disease and the Mucopolysaccharidoses.
LIMB AND DIGIT DEVELOPMENT
The upper limb bud forms at ~ day 24, followed shortly thereafter by the lower limb bud (at ~ day 28).
The limb bud comprises a core of mesenchyme, surrounded by ectoderm.
The AER (apical ectodermal ridge) forms a thickening at the distal end of the limb bud.
The distal upper limb bud forms a digital plate, distally (for the fingers) and a carpal plate (for the hand). Then, via programmed cell death, digital rays form.
COMMON LIMB DISORDERS: TERMINOLOGY
Amelia is absence of a limb.
Meromelia is absence of a part of a limb.
DIGIT DISORDERS
Syndactyly is webbing (fusion) of digits.
Polydactyly is presence of extra digits.
Brachydactyly is shortening of digits.
Known Teratogens that cause limb and digit malformations, include