Types of Anchorage Based on Maximum Anchorage Demand
Anchorage is classified into three types based on the maximum anchorage required:
Type A: Maximum Anchorage
Definition: Anchorage demand is very high.
Space Utilization: Not more than 1/4th of the extraction space should be closed by forward movement of anchor teeth.
Mechanism: The extraction space is primarily closed by maximum incisor retraction.
Type B: Moderate Anchorage
Definition: Anchorage demand is moderate.
Space Utilization: Anchor teeth are allowed to move forward by up to half the extraction space.
Mechanism: The extraction space is closed by a combination of incisor retraction and posterior tooth protraction.
Type C: Minimum Anchorage
Definition: Anchorage demand is very low.
Space Utilization: More than half of the extraction space is closed by mesial movement of the anchor teeth.
Mechanism: The extraction space is primarily closed by protraction of posterior teeth with minimal incisor retraction.
Group B Anchorage: Biomechanics of Space Closure
Key Features
Archwire: A working archwire with a minimal curve of Spee (e.g., 0.019 × 0.025-inch SS wire) is engaged into the bracket slots and molar tubes.
Couples and Forces:
The wire generates a couple at the level of the bracket/molar tube at both ends, leading to the generation of a moment of couple (M_c).
Tiebacks create a force for space closure (F), generating a moment of force (M_F).
Force and Moment Interaction:
At either end of the system, the moments of couple and force are created in opposite directions, canceling each other.
This leaves only the translatory force (F) to exist, enabling space closure.
Translational Movement
When moments are balanced correctly:
No vertical component of force is produced.
No rotational tendency occurs in the system.
Occlusal plane and overbite remain unchanged.
Diagram: Depicts the working archwire (faded blue line) and the resulting forces and moments.
Outcome: Translation of anterior and posterior segments without altering the occlusal plane or overbite.
Planned Imbalance of Moments
In some scenarios, moments are deliberately imbalanced to achieve specific vertical movements:
Posterior Teeth: Extrusion (yellow arrows).
Anterior Teeth: Intrusion (yellow arrows).
Effect: Opens the deep overbite by modifying the vertical dimension.
Diagram: Illustrates the planned imbalance (thick red curved arrow) leading to controlled vertical movements.
Outcome: Deep overbite correction through extrusion of posterior teeth and intrusion of anterior teeth.
Summary
Group B anchorage allows for controlled space closure through balanced forces and moments. By adjusting the moments, orthodontists can achieve either translational movement or vertical adjustments, making it a versatile approach in clinical orthodontics.
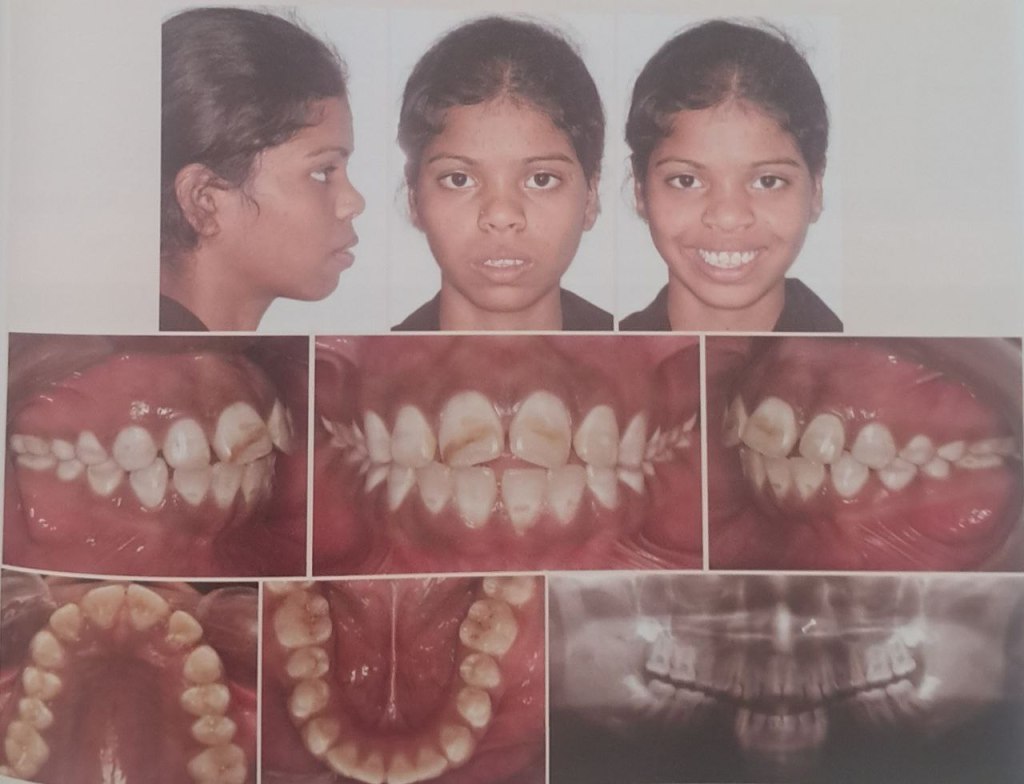
Bimaxillary protrusion is a condition characterized by protrusive and proclined upper and lower incisors with increased lip procumbency. It is commonly seen in African-American and Asian populations but can occur across all ethnic groups. Due to the negative perception of protrusive dentition and lips in many cultures, patients with bimaxillary protrusion often seek orthodontic treatment to improve their facial profiles. This guide summarizes key aspects of bimaxillary protrusion, including its etiology, pretreatment characteristics, treatment goals, and outcomes.
Etiology of Bimaxillary Protrusion
The etiology of bimaxillary protrusion is multifactorial, including:
Genetic Factors: Hereditary traits influencing facial and dental structures.
Environmental Factors:
Mouth breathing.
Tongue and lip habits.
Increased tongue volume.
Morphological Features
Keating’s study on Caucasian patients identified the following cephalometric traits:
Feature
Observation
Posterior cranial base
Shorter
Maxilla
Longer and more prognathic
Skeletal pattern
Mild Class II
Upper and posterior face height
Smaller
Facial planes
Divergent
Soft tissue profile
Procumbent with a low lip line
Pretreatment Characteristics
Cephalometric Traits
Patients with bimaxillary protrusion exhibit the following pretreatment characteristics:
Trait
Observation
Upper and lower incisor proclination
Increased (2-3 SD above mixed racial norms)
Vertical growth patterns
Increased lower anterior face height
Mandibular plane angle
Elevated
Alveolar heights
Increased
Soft Tissue Features
Lip Position:
Upper and lower lips are ahead of the E-plane.
Lower lip: 6.0 mm ahead (Keating’s Caucasian sample).
Upper lip: 1.0 mm ahead (less than Keating’s 3.4 mm).
Nasolabial Angle:
Found to be 94° (1 SD more acute than mixed racial norms).
Tan’s study on Chinese patients reported an even more acute angle (86.6°).
Lip Thickness:
Increased, likely due to a higher proportion of African-American patients in the study.
Alveolar Morphology
Alveolar Width: Reduced compared to Handelman’s norms.
Alveolar Height: Increased, consistent with vertical facial growth patterns.
Thin and elongated alveolus may limit retraction mechanics and necessitate surgical osteotomies in severe cases.
Orthodontic Treatment Goals
The primary objectives of treating bimaxillary protrusion include:
Dental Goals:
Retraction and retroclination of maxillary and mandibular incisors.
Reduction in incisor proclination and protrusion.
Soft Tissue Goals:
Decrease in lip procumbency and convexity.
Improvement in the nasolabial angle.
Mechanics Used:
Extraction of four first premolars.
Retraction using maximum anchorage mechanics.
Flowchart: Treatment Goals and Process
1. Initial Diagnosis → 2. Extraction of Four Premolars → 3. Retraction of Incisors → 4. Profile Improvement
Treatment Outcomes
Dental and Skeletal Changes
Parameter
Observation
Interincisal angle
Increased significantly
Incisor inclination
Decreased significantly
Anteroposterior incisor position
Reduced significantly (P < .001)
Soft Tissue Changes
Upper Lip Retraction:
Ratio of upper incisor retraction to upper lip retraction: 2.2:1 (similar to Chiasson and Hershey).
Lip response depends on factors like interlabial gap, lip redundancy, and musculature quality.
Vertical Dimension
No significant changes in lower anterior face height or mandibular plane angle, indicating that treatment mechanics do not affect the vertical dimension.
In the world of orthodontics, Class II intermaxillary elastics have stood the test of time as a cornerstone of clinical treatment. Since their introduction by Maynard in 1843 and subsequent refinement by Henry A. Baker in the late 19th century, these small but mighty elastics have been indispensable in managing malocclusions. For orthodontic students, understanding their effects, particularly on the functional occlusal plane (FOP), is essential for mastering treatment planning and clinical decision-making.
Why Does the Functional Occlusal Plane Matter?
The occlusal plane is more than a line connecting occlusal surfaces; it’s a fundamental aspect of facial esthetics, function, and skeletal harmony. Its orientation relative to cranial and mandibular planes influences:
Maxillary and mandibular skeletal relationships
Facial forms and esthetics
Occlusal function
Alterations in the occlusal plane, whether due to growth or treatment, can significantly affect treatment outcomes and post-treatment stability. As orthodontic practitioners, it’s crucial to strike a balance between functional correction and maintaining or improving esthetic harmony.
The Role of Class II Elastics
Class II elastics have long been used to address sagittal and vertical discrepancies, including the correction of Class II malocclusions and open bites. While effective, their reciprocal forces can induce both desirable and adverse effects. Reports have suggested that Class II elastics might steepen the occlusal plane, potentially leading to instability or relapse post-treatment. However, these findings were often based on small sample sizes or non-growing patients, leaving gaps in our understanding of their effects during growth phases.
To address these gaps, a recent study analyzed the effects of Class II elastics on FOP in growing patients aged 11 to 16 years. Here’s what the researchers aimed to find out:
Does the use of Class II elastics steepen the FOP?
Are these changes more pronounced in extraction cases or patients with high-angle skeletal patterns?
Do these changes persist or relapse after treatment?
Key Findings to Remember
1. Angular Changes in the FOP
FOP-SN and FOP-FH: Decreased significantly from pretreatment (T0) to post-treatment (T1) and continued to decrease 1 year post-treatment (T2).
FOP-MP: Increased from T0 to T1, likely as a reciprocal effect of FOP-SN/FH changes.
2. Influence of Skeletal Patterns
Hyperdivergent patients showed the largest FOP angles across all time points, while hypodivergent patients had the smallest.
Despite these differences, changes in FOP were consistent across skeletal types, indicating that Class II elastics affect all growth patterns similarly.
3. Treatment Modalities: Extraction vs. Non-Extraction
Patients undergoing extraction treatment exhibited steeper initial FOP-MP angles, reflecting a preference to extract in such cases.
No significant differences were observed in FOP changes between extraction and non-extraction groups during or after treatment.
Clinical Implications for Students
Normal Growth vs. Treatment Effects: The study suggests that changes in FOP may largely reflect normal growth patterns rather than direct effects of Class II elastics. This aligns with findings from Creekmore, Schudy, and Harris, emphasizing the importance of accounting for growth dynamics.
Individualized Treatment Planning: While Class II elastics are versatile, their effects on the FOP and associated structures vary based on skeletal patterns and growth trends. Orthodontic treatment must be tailored to each patient’s unique craniofacial morphology.
Extraction Considerations: Although extraction cases may present steeper occlusal planes initially, the use of Class II elastics does not appear to exacerbate this steepness.
Takeaways for Orthodontic Students
Class II elastics remain a reliable tool for addressing Class II malocclusions, but understanding their nuanced effects on the FOP is key to optimizing outcomes.
Growth patterns play a pivotal role in how the FOP evolves during treatment. Observing these changes in clinical practice can enhance your ability to predict and manage treatment outcomes.
Finally, always consider the interplay between function, esthetics, and stability when planning orthodontic interventions.
Class II elastics may be small, but their impact on treatment is anything but. With careful planning and an understanding of growth influences, you can wield this classic tool to achieve remarkable results in your future practice.
Bimaxillary protrusion is a common orthodontic condition marked by protrusive and proclined upper and lower incisors, coupled with increased lip prominence. While predominantly seen in African American and Asian populations, it is not limited to any single ethnic group. This condition often leads patients to seek orthodontic treatment due to the aesthetic concerns of protruding lips and dentition.
Soft Tissue and Hard Tissue Correlation
Orthodontic studies present two conflicting perspectives on the relationship between incisor retraction and lip position:
Strong Correlation: Some studies demonstrate a direct relationship between incisor and lip retraction.
Weak Correlation: Some studies suggest that soft tissue changes do not proportionally mirror dental movements due to variables like growth, lip tonicity, and anchorage.
Four retrospective studies on bimaxillary protrusion treatment provided valuable insights:
Study Findings
Upper Lip Retraction (mm)
Lower Lip Retraction (mm)
Nasolabial Angle Increase (°)
Caplan et al. (2009)
3.0
2.4
Not significant
Tan et al.
2.7
2.0
10.5
Lew
3.2
4.5
10.0
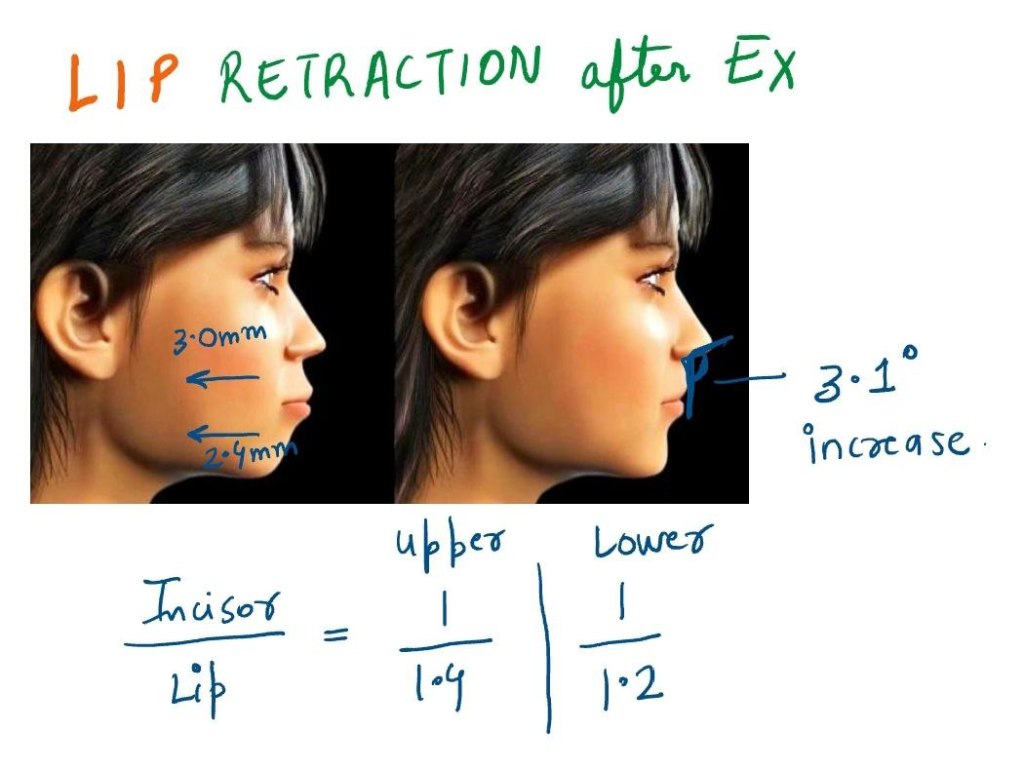
Bills et al.
3.0
2.4
3.1
Incisor Retraction and Lip Retraction Ratios
Study
Upper Lip to Incisor Retraction
Lower Lip to Incisor Retraction
Caplan et al.
1:1.4
1:1.2
Other Studies
1:2.2
1:1.75
Clinical Implications
Four-premolar extractions effectively reduce lip procumbency in bimaxillary protrusion.
Nasolabial angle tends to increase post-treatment.
Molar distalization is a crucial technique in orthodontics, particularly for patients with Class II malocclusion. Thanks to advancements in biomechanics, materials, and technology, orthodontists now have access to a variety of intramaxillary intraoral appliances that can apply light, continuous forces for effective molar distalization. These appliances have become a game-changer, providing us with more precise control and predictable results.
Types of Intramaxillary Appliances
The application of forces in molar distalization can come from two primary areas: the buccal or the palatal region. Depending on where the force is applied, appliances can be categorized into two broad groups:
Buccal Force Application: These appliances apply force from the outside of the dental arch.
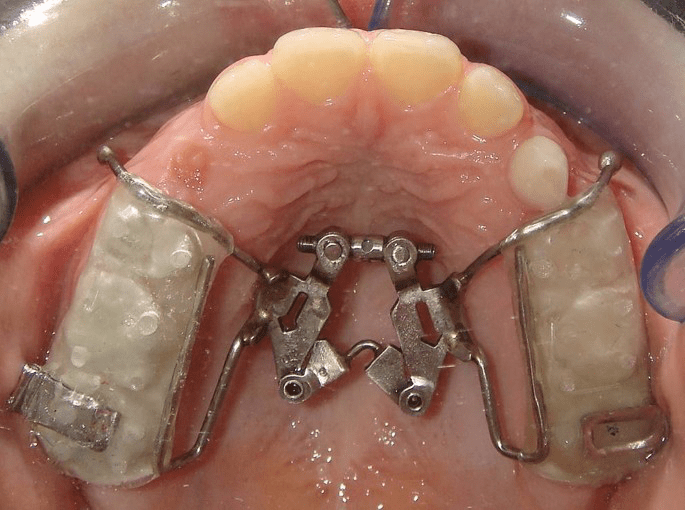
Palatal Force Application: These appliances exert force from the roof of the mouth.
Additionally, the force mechanisms can be divided into two categories:
Friction-Free Mechanism: This type involves appliances like the pendulum, which are designed to move the molars without causing significant friction.
Sliding Mechanism: Appliances like nickel-titanium (NiTi) coil springs use a sliding mechanism to apply force, creating a more dynamic force delivery system.
Each of these appliance types has its own set of advantages and drawbacks, and comparing their efficiency in achieving molar distalization is key to making evidence-based treatment decisions. However, due to the limited number of randomized clinical trials, a meta-analysis is often not possible. That said, a comprehensive analysis of existing studies can still offer valuable insights into how these appliances work.
Treatment Outcomes: Overall Effects
When all intramaxillary appliances were considered together, some general findings emerged:
First Molar Movement: On average, first molars moved 2.9 mm distally, but this came with a 5.4° of distal tipping.
Incisor Movement: The incisors shifted mesially by 1.8 mm with 3.6° of mesial tipping.
Premolar Movement: Premolars showed a mesial shift of 1.7 mm, though tipping was less pronounced.
Vertical movements were generally extrusive for incisors and premolars, with incisors showing an average extrusion of 0.4 mm and premolars 1.1 mm. Interestingly, molar vertical movements were not statistically significant, indicating that the main effect on molars was distal movement and tipping rather than vertical displacement.
Treatment Effects: Buccal vs. Palatal Appliances
Now, let’s delve into the specific effects of buccal and palatal appliances. These results highlight the different ways these appliances move teeth:
Buccal Appliances:
Molar Movement: Molar distal movement was 2.6 mm, with a more significant tipping of 8.3°.
Incisor Movement: Incisors moved mesially by 1.9 mm with 5.0° of mesial tipping.
Premolar Movement: Premolars demonstrated a 2.0 mm mesial shift, accompanied by 7.0° of mesial tipping.
Vertical Movement: Premolars showed a slight extrusion of 0.7 mm, while incisors had a more modest extrusion of 0.2 mm.
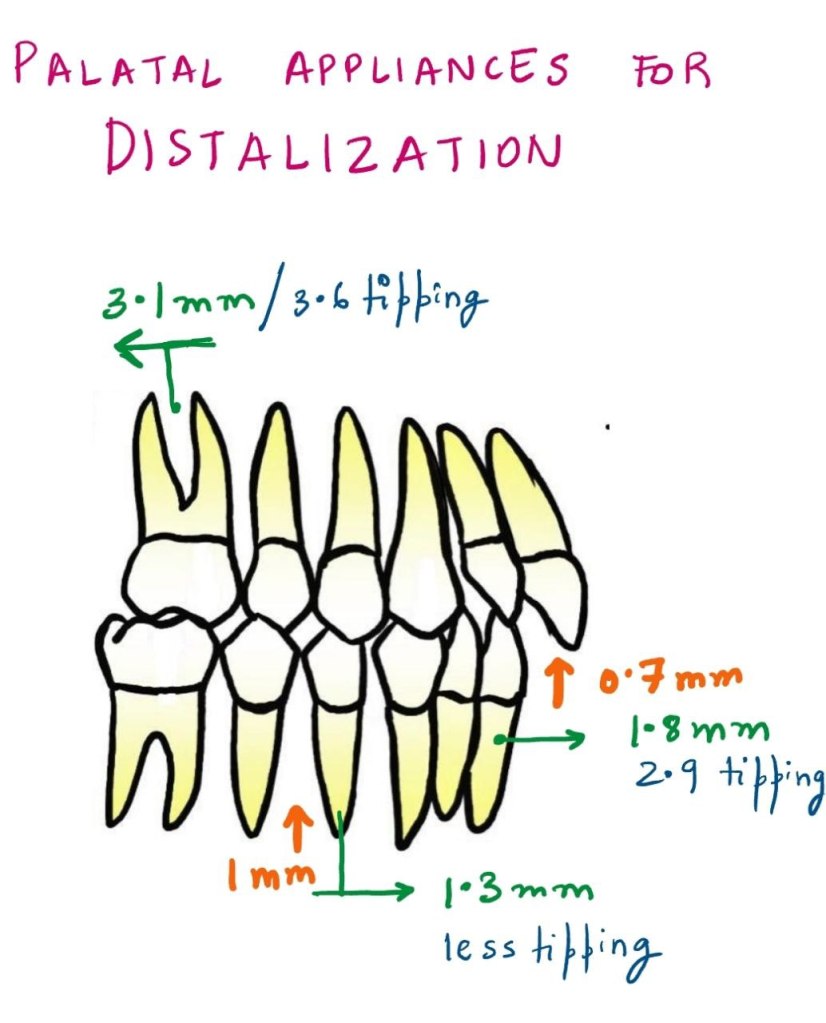
Palatal Appliances:
Molar Movement: Molar distalization was slightly more pronounced, with 3.1 mm of movement and 3.6° of tipping.
Incisor Movement: Incisors exhibited a mesial shift of 1.8 mm with 2.9° of mesial tipping.
Premolar Movement: Premolars moved mesially by 1.3 mm with less tipping than buccal appliances.
Vertical Movement: The extrusion for incisors was 0.7 mm, and premolars showed an extrusion of 1.0 mm.
Molar Distalization and Anchorage Loss
The primary effect of noncompliance intramaxillary appliances is molar distalization, which is typically achieved through a combination of crown distal movement and tipping. While distalization is the goal, a common side effect observed is loss of anchorage. This loss can be seen in the mesial movements and extrusions of incisors and premolars.
Key Findings:
Molars: Show a combination of distal crown movement and distal tipping.
Incisors: Exhibit mesial movement, tipping, and extrusion.
Premolars: Display mesial crown movement and extrusion.
As with any treatment modality, careful planning is required to manage these unintended side effects and achieve the best possible clinical outcomes.
Buccal vs. Palatal Appliances: Tipping and Force Mechanics
One interesting observation in the study was the difference in tipping effects between buccal and palatal acting appliances. Palatal appliances consistently resulted in less tipping of teeth compared to buccal appliances, as indicated by the non-overlapping confidence intervals.
Why the Difference?
The key reason for this difference lies in the moment arm of the force. In palatal appliances, the line of action of the force is closer to the center of resistance of the tooth, leading to less tipping and more controlled molar movement.
Table 1: Comparison of Tipping between Buccal and Palatal Appliances
Appliance Type
Molars Distal Movement (mm)
Molars Tipping (°)
Incisor Mesial Movement (mm)
Incisor Tipping (°)
Premolar Mesial Movement (mm)
Premolar Tipping (°)
Buccal Appliances
2.6
8.3
1.9
5.0
2.0
7.0
Palatal Appliances
3.1
3.6
1.8
2.9
1.3
3.0
This table highlights the greater tipping observed with buccal appliances compared to palatal appliances, as well as the differences in molar distalization and mesial movement of incisors and premolars.
The Nance Button: Anchorage Considerations
Another point of discussion is the use of the Nance button to reinforce anterior anchorage during molar distalization. While it can support anchorage to some extent, it does not provide absolute anchorage. This is because the Nance button, as part of the anchorage unit, cannot completely resist mesial forces during molar distalization. Clinically, this often results in an increased overjet and proclination of maxillary incisors.
Clinical Tip:
For patients already presenting with an increased overjet, orthodontists must proceed with caution when prescribing these appliances. These cases may require additional measures to control the overjet and manage incisor proclination.
The Pendulum Appliance: A Look at Tipping and Movement
The pendulum appliance, a popular friction-free appliance, was noted in the study to cause the greatest distal tipping of molars. However, this tipping was correlated with a larger amount of distal crown movement. Interestingly, this tipping can often be corrected with the use of molar uprighting bends.
Table 2: Molar Distalization and Tipping with the Pendulum Appliance
Movement Type
Molar Distal Movement (mm)
Molar Tipping (°)
Pendulum Appliance
3.4
9.0
This table shows that the pendulum appliance can achieve significant molar distalization but at the cost of increased tipping. These tipping movements can be addressed with molar uprighting bends, which can help reduce the tipping angle.
Factors Affecting Molar Distalization
Several factors can influence the effectiveness of molar distalization, including:
Teeth Used for Anchorage: Different anchorage setups can affect the extent of distal movement.
The Type of Appliance Used: Whether the appliance uses a sliding mechanism or a friction-free mechanism plays a role.
Patient Factors: Age, initial molar relationships, and the eruption of second and third molars all contribute to how effectively molars are distalized.
In studies that focus on growing patients, mean ages ranged from 11.2 to 14.9 years, which is crucial because the growth phase can significantly impact the effectiveness of treatment. For example, molar distalization is often more effective before the second molars have erupted. When second molars are erupted, more force may be required, and the treatment time may increase.
Table 3: Influence of Molar Eruption on Distalization Efficiency
Angle’s Class I malocclusion is one of the most common types of dental misalignment encountered in clinical practice. It refers to a situation where the upper and lower teeth are generally aligned, but various issues such as crowding, spacing, bidental protrusion, vertical problems (deep bite or open bite), and transverse issues (crossbite or scissor bite) can arise. The good news is that these issues are typically easier to treat compared to more complex malocclusions, giving patients a higher chance of successful outcomes.
The Role of Growth in Achieving Class I Malocclusion
It’s important to understand that many of us begin with a skeletal Class II pattern during early development. With favorable growth, the individual’s skeletal structure may gradually transition into a skeletal Class I relationship. For example, a patient presenting with a mild facial convexity in mixed dentition can often be expected to develop a straighter profile as they continue to grow. This process occurs as growth in all three spatial planes—vertical, transverse, and sagittal—happens synchronously, ultimately resulting in a Class I skeletal configuration.
As this growth progresses, the facial profile becomes less convex, giving the appearance of a more balanced, harmonious face. Therefore, many orthodontic cases that are deemed successful are a combination of favorable natural growth and orthodontic intervention.
Focus on Intraarch Alignment and Interarch Occlusion
In patients with Angle’s Class I malocclusion, the anteroposterior skeletal relationship is normal. The primary goal of orthodontic treatment in these cases is to focus on correcting intraarch alignment and interarch occlusal relations. Treatment options vary depending on the individual case and may include:
Extractions: Often used to create space when necessary.
Non-extraction approaches: These can include slenderization (reducing the size of teeth), expansion (widening the dental arch), distalization (moving the back teeth backwards), derotation (correcting the rotation of posterior teeth), and proclination (moving retroclined anterior teeth forward).
Managing Specific Class I Malocclusion Issues
Crowding and Spacing: Spacing issues in the dental arch can occur for various reasons, such as hypodontia (missing teeth) or microdontia (abnormally small teeth). Hypodontia often affects the maxillary lateral incisors and mandibular premolars. In these cases, the orthodontist must decide whether to open space for prosthetic replacements or to close the space orthodontically. On the other hand, microdontia can be managed through space redistribution and the aesthetic build-up of smaller teeth.
Bidental Protrusion: Bidental protrusion is another common concern seen in patients with a Class I skeletal base. This condition can often be efficiently managed with premolar extractions, which help reduce the protrusion and bring the teeth into better alignment.
Vertical and Transverse Problems: While Class I malocclusion is generally associated with a normal anteroposterior skeletal relationship, vertical (deep bite or open bite) and transverse issues (crossbite or scissor bite) may still be present. These concerns are often addressed in subsequent stages of orthodontic treatment.
Conclusion
Angle’s Class I malocclusion is a frequent and treatable condition seen in orthodontic practice. The successful outcomes often stem from a combination of natural growth and targeted orthodontic interventions. Whether addressing crowding, spacing, bidental protrusion, or vertical and transverse problems, orthodontists can employ various techniques such as extractions, slenderization, expansion, and more to achieve optimal results. Understanding the underlying growth patterns and employing the right treatment plan is key to ensuring that patients achieve a balanced, functional, and aesthetically pleasing smile.
Causes: Class III malocclusions can arise from mandibular protrusion, maxillary retrusion, or both.
Studies on Maxillary Retrusion: Various studies report the contribution of maxillary retrusion to Class III malocclusions in individuals with normal mandibles, with percentages ranging between 19.5% and 37%.
Treatment Focus: This recognition has led to introducing treatments like the orthopedic facemask for maxillary protraction.
Alternate Rapid Maxillary Expansion and Constriction (Alt-RAMEC)
Protocol: Expands and contracts the maxilla alternately (1 mm/day for a week each, repeated for 7–9 weeks) using a two-hinged rapid maxillary expander.
Rationale: Mimics the rocking mechanism in tooth extraction, disarticulating circum-maxillary sutures without over-expansion.
Alt-RAMEC Protocol Details
Activation Phase:
The expansion screw was turned twice daily at a rate of 0.20 mm per turn.
This phase lasted for 1 week, ensuring the maxilla was progressively expanded.
Deactivation Phase:
The screw was then turned twice daily in reverse at a rate of 0.20 mm per turn.
This phase also lasted for 1 week, gradually constricting the maxilla back.
Repetition:
The activation and deactivation sequence was repeated for a second cycle.
After each week-long activation or deactivation phase, the patients were examined to monitor proper opening or closing of the screw, ensuring precision in the procedure.
Post-Protocol Guidance:
Following the completion of the Alt-RAMEC cycles, patients were instructed to wear the Reverse Headgear (RH). This is a common adjunct in orthopedic facemask therapy designed to enhance maxillary protraction after the suture disarticulation achieved by Alt-RAMEC.
Results of Alt-RAMEC
Comparison with RPE:
Alt-RAMEC: Achieved an average anterior movement of point A by 5.8 mm in cleft patients over 9 weeks.
RPE: Achieved only 2.6 mm movement after 1 week.
Suture Opening: Experimental studies confirmed that Alt-RAMEC opens circum-maxillary sutures more extensively than 1 week of RPE.
Clinical Implications
Parameter
A/D-RPE Group
RPE Group
Comparison with Previous Studies
Maxillary Advancement (Point A)
4.13 mm (T3)
2.33 mm (T3)
Greater movement in A/D-RPE group, similar to Liou and Tsai (2005) findings.
Anterior Movement of Point A
Significant difference (greater in A/D-RPE)
Observed, but lesser than A/D-RPE
Liou and Tsai (2005), Merwin et al. (1997), Kapust et al. (1998), Sung & Baik (1998) showed comparable results to RPE group.
Mandibular Rotation
Posterior rotation observed
Posterior rotation observed
Consistent with previous studies (Merwin et al., 1997; Kapust et al., 1998).
Anterior Face Height Increase
Observed
Observed
Findings align with previous studies.
Maxillary Plane Angle
Decrease of 1.53 degrees (T3)
Decrease observed
A/D-RPE showed significant decrease, consistent with previous studies.
SNA Angle Increase
Significant difference (greater in A/D-RPE)
Observed
A/D-RPE resulted in more significant SNA angle increase compared to RPE group.
ANB Angle Increase
Significant difference (greater in A/D-RPE)
Observed
A/D-RPE showed more significant increase in ANB angle.
Overjet Correction
Greater correction in A/D-RPE
92.5% skeletal, 7.5% incisor tipping
A/D-RPE showed a higher skeletal contribution (93%) vs. RPE (92.5%).
Skeletal vs. Dental Contribution to Overjet
93% skeletal, 7% dental
92.5% skeletal, 7.5% dental
A/D-RPE showed a higher skeletal contribution (57.9% maxillary, 35.1% mandibular).
Soft Tissue Profile Changes
More pronounced in A/D-RPE (upper lip anterior, lower lip posterior)
Observed (less pronounced)
Profile improvement observed in both groups; A/D-RPE showed more pronounced soft tissue changes.
So you’ve got the braces thing going on, huh? A journey to a stellar smile, no doubt! But let’s face it, chomping down on everything from apples to samosas can be a real drag with those metal friends attached. Fear not, fellow food enthusiasts, for this guide will turn you into a braces-wearing, balanced-diet boss!
Carbs: Your Chapatti and Rice BFFs
Lucky you! Most grains are soft and chew-friendly. Pile on the fluffy rice, indulge in those melt-in-your-mouth rotis (dunk ’em in dal for extra protein power!), and enjoy that breakfast bread (just maybe avoid the rock-hard baguettes for now). Discomfort? Mash those chapattis into a delightful curry and rice symphony – your taste buds and braces will thank you.
Dairy: Your Calcium Cavalry
Milk, yogurt, cheese – the holy trinity of strong teeth and happy braces! They’re soft, delicious, and pack a calcium punch. Bonus points for milkshakes (because, hello, who doesn’t love a good milkshake?), but go easy on the sugar. Think of yourself as a calcium crusader, venturing forth with every spoonful of yogurt!
Veggies: Your Mashed Marvels
Ah, vegetables – the dietary champions! Most Indian meals involve cooked veggies, which are a breeze for braces. Feeling a bit adventurous? Mash them up for extra comfort. Need a raw veggie fix? Grate those carrots or chop your salad into bite-sized pieces. Just remember, you’re not a superhero (yet!), so skip the superhero-sized bites.
Fruits: Your Juicy Jewels (with a Few Caveats)
Fruits – the colorful crew that adds sweetness to life! But with braces, things can get a little tricky. Apples? Unless you’re feeling like a dental daredevil, cut them up. Unripe pears and peaches? Give them a side-eye. Feeling extra tender after a wire change? Citrus fruits and berries are your new best friends. Remember, if all else fails, fruit juice is always a healthy option. Just a heads-up, though, chomping on icy-cold fruits might not be the most pleasant experience with all that metal in your mouth. Let your food warm up a bit for a friendlier feast.
Nuts & Seeds: Your Sneaky Saboteurs (But We Can Work With Them)
Okay, nuts and seeds – they’re delicious, nutritious, but a real challenge for braces. Here’s the deal: during your orthodontic adventure, swap those whole nuts for nut butters (think creamy peanut butter heaven!) or coarsely grind your favorite seeds. This way, you get the goodness without the potential for a braces breakdown.
Meat: Your Tender and Chopped Champs
Meat – the protein powerhouse! Unfortunately, it can be a bit fibrous and tough on braces. Here’s the golden rule: avoid gnawing on meat straight off the bone (think of your teeth, not your inner caveman). Tofu and cottage cheese are great protein alternatives, but if you must have meat, choose lean, tender cuts and chop them into bite-sized pieces.
The Absolute No-Nos: Your Braces’ Nightmares
Now, let’s talk about the foods that would make your braces weep. Gum (both sugary and sugarless) is a big no-no. Sticky candies? Forget about it. Hard foods like whole nuts (unless grinded), popcorn, corn on the cob, pizza crusts (sorry!), ice, and cookies are strictly off-limits. Think of them as villains in your quest for a perfect smile.
Remember: Consistency is key! Stick to this guide, embrace some creativity in the kitchen, and you’ll be a braces-wearing, balanced-diet pro in no time. Now go forth and conquer that delicious, nutritious world, one bite at a time (and maybe cut that bite in half)!