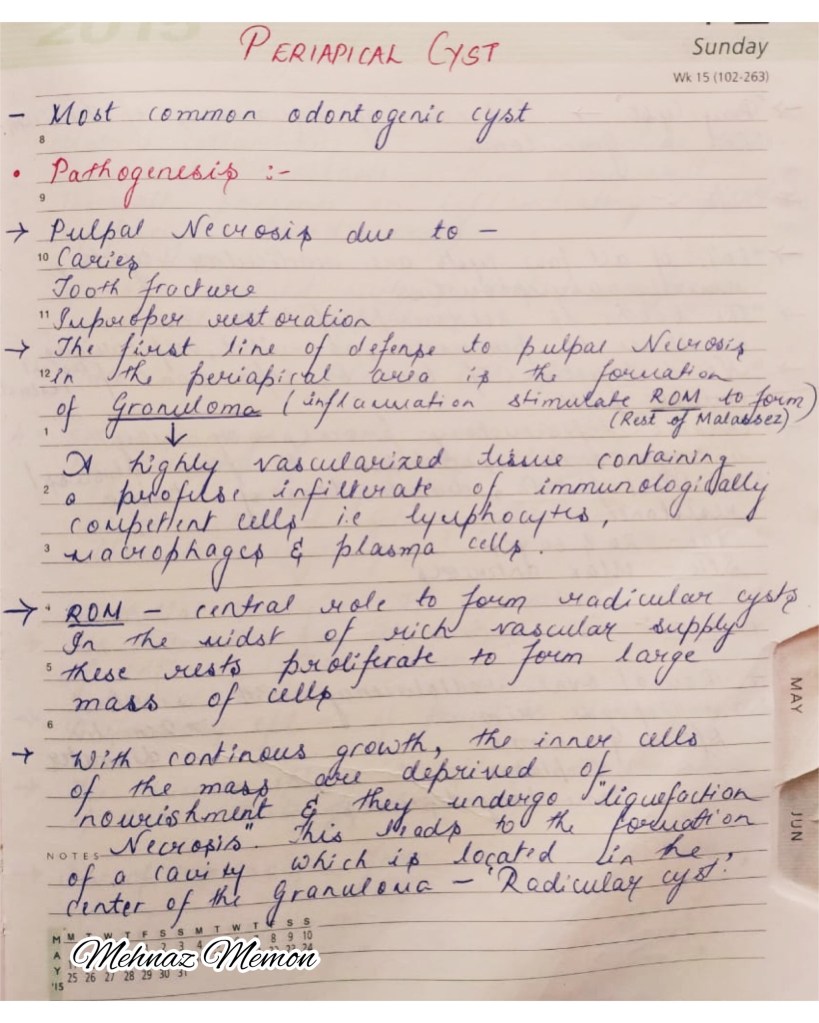
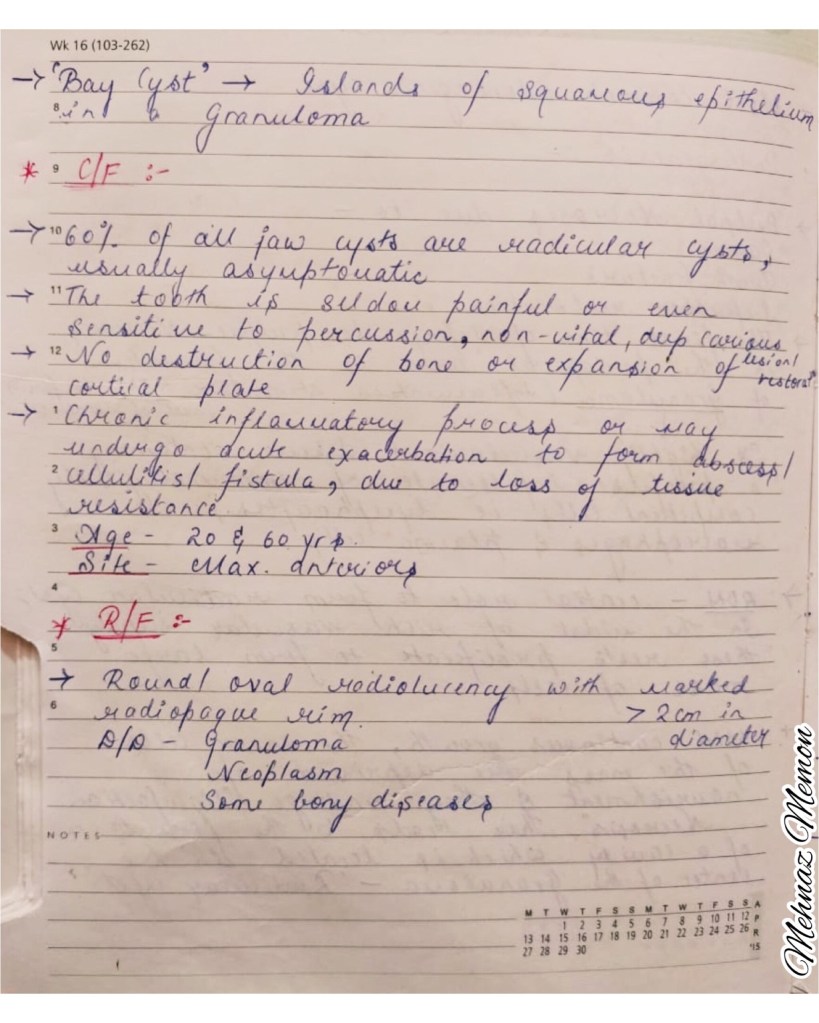
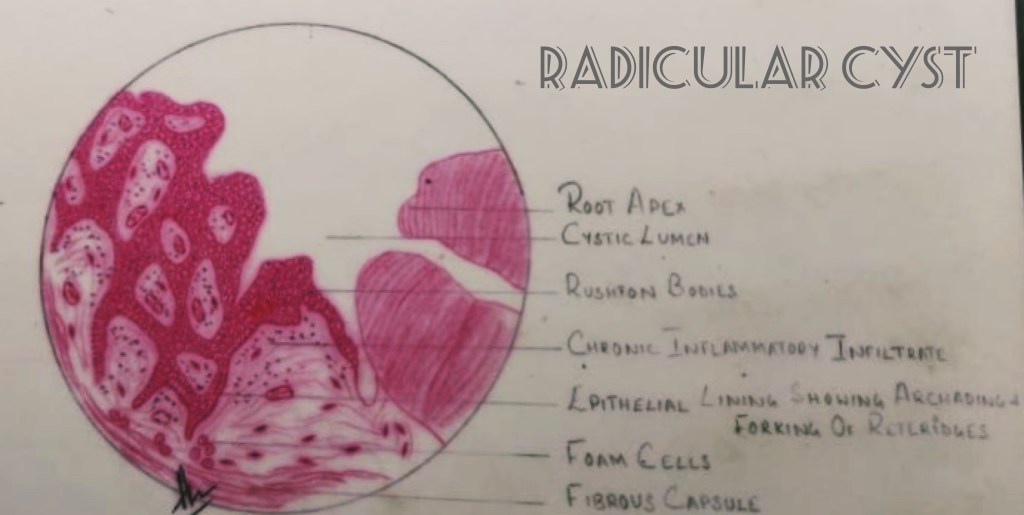
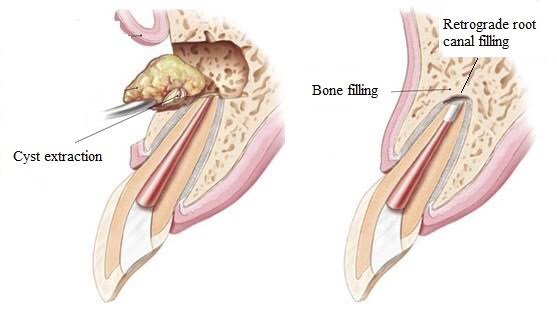
Radiolucent area around the tip of the roots indicate periradicular inflammation. #clinicaltips👇🏻 Radiographically, 1. Granulomas form small welldefined radiolucencies. 2. A radicular cyst forms a large well-defined radiolucency with or without a radiopaque (hyperostotic) border. 3. Apical abscess form large radiolucencies with diffuse irregular borders.
Pemphigus describes a group of chronic bulbous diseases (Wichman) of the skin, characterized by the appearance of vesicles & bullae (fluid-filled intradermal blisters) that develop in cycles.
➡️ A auto-immune blistering disease of the skin & mucous membrane. Finding of IgG antibody directed against the cell surface of keratinocytes is seen.
➡️ 3 primary subsets of pemphigus include –
Pemphigus Vulgaris – 70%
Pemhigus foliaceus
Paraneoplastic pemphigus
IgA pemphigus
Drug induced pemphigus
➡️ Associated factors:
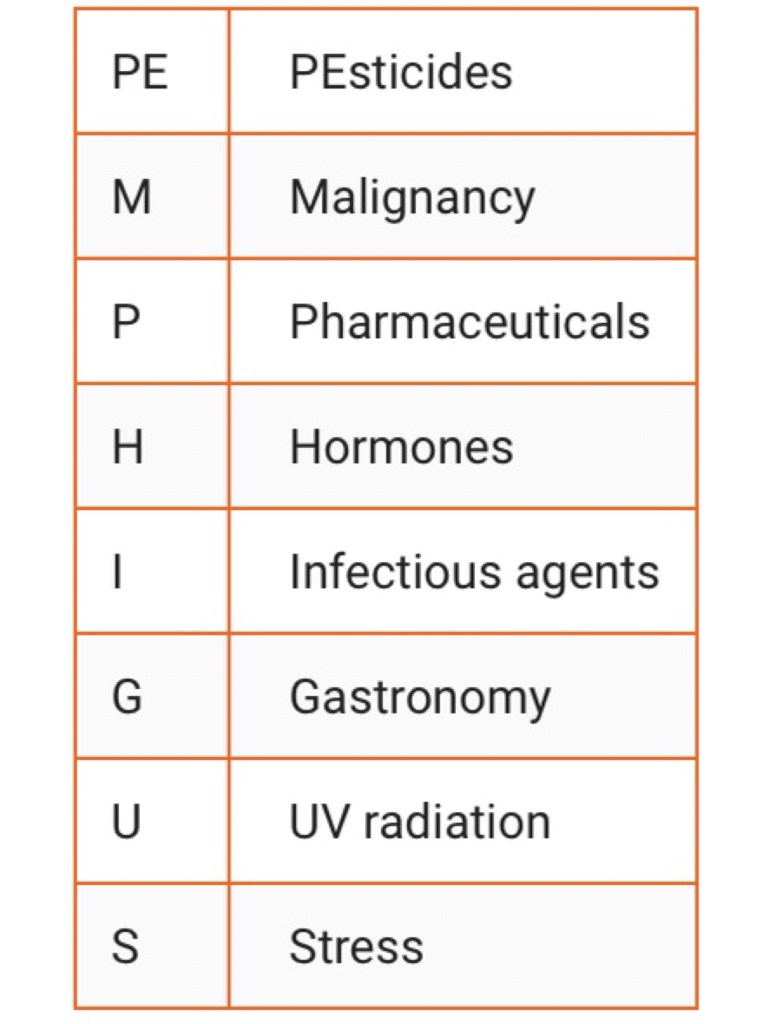
An acronym has been suggested from the name of the disease, PEMPHIGUS, to encompass those factors:
1. Drugs: The inciting medications can be classified based on their chemical structure, with the main groups being thiols drugs, phenol drugs, and non-thiol/phenol drugs. The most common offending drugs include D-penicillamine, captopril, and penicillin.
2. Diet: Once the drug-induced pemphigus has developed, besides discontinuing the drug, the nurse or physician should educate the patient on a recommended diet. Certain foods contain phenols and thiols that can exacerbate the condition. Thus a dietary consult is necessary. Foods that contain phenol and thiol like compounds include chives, garlic, onion, black pepper, cashew, and mangoes.
3. Infection: The most frequently incriminated infectious agents are the viruses of the herpetoviridae family, namely herpes simplex, EBV, CMV, and even HH8.
4. Auto-immune diseases
5. UV Radiation
6. Stress: Avoiding emotional stress may be therapeutic in pemphigus patients, hastening the healing process and reducing or stopping the use of immunosuppressive drugs.
Pemphigus Vulgaris
Pathogenesis:
Intercellular antibody(IgG) bind to the keratinocyte desmosomes & desmosome free areas of keratinocyte cell membrane (Desmoglein 1 & 3) ➡️ Loss of cell to cell adhesion
Fixation of components of complement to surface of epidermal cells
Release of inflammatory mediators & recruitment of activated T-cells.
Clinical features:
Age: 50 to 60 years
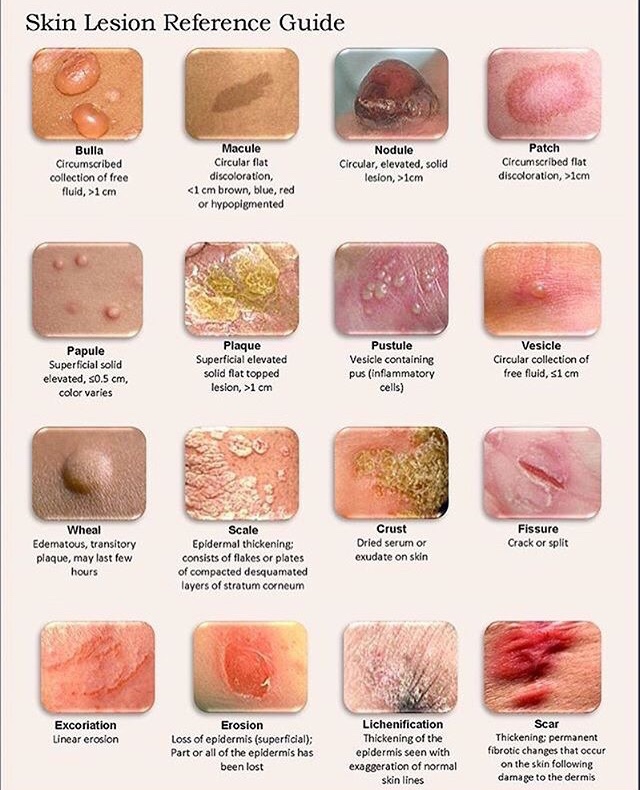
Rapid appearance of vesicles & bullae which easily rupture (mm-cm) – involve large areas of skin surface, leaving raw eroded surface.
Contain thin, watery fluid soon after development but later becomes purulent & sanguineous.
Characteristic feature of pemphigus ➡️ Nikolsky’s sign – Loss of epithelium by rubbing unaffected skin, adjacent to the vesicle, skin peels on lateral pressure. This differentiates tense bullous lesions seen in pemphigoid, which do not rupture with the slight pressure of a finger.
Due to prevesicular edema – disruption of dermal-epidermal junction.
➡️ Uncommon variant of Pemphigus Vulgaris – P. Vegetans
Occurence: 1-2%
Age of onset: 40-50 years
Clinical subtypes –
▪️1) Flaccid bullae & erosions (Neumann)
▪️2) Pustules (Hallopeau)
They develop into hyperpigmented vegetative plaques & hypertrophic granulation tissue at the periphery.
Location: Intertriginous areas, Oral mucosa
Oral invovement: Cerebriform tongue.
Oral Manifestations:
Mucosal lesions precede the cutaneous ones by months – 50-70% of the cases mucosa is affected with erosions on gingiva, palate/buccally.
Erosions are ill-defined, irregular, painful & slow to heal.
Shedding of epithelium is seen
Larynx – hoarseness & difficulty to eat or drink.
Involvement of other mucosal surfaces also seen.
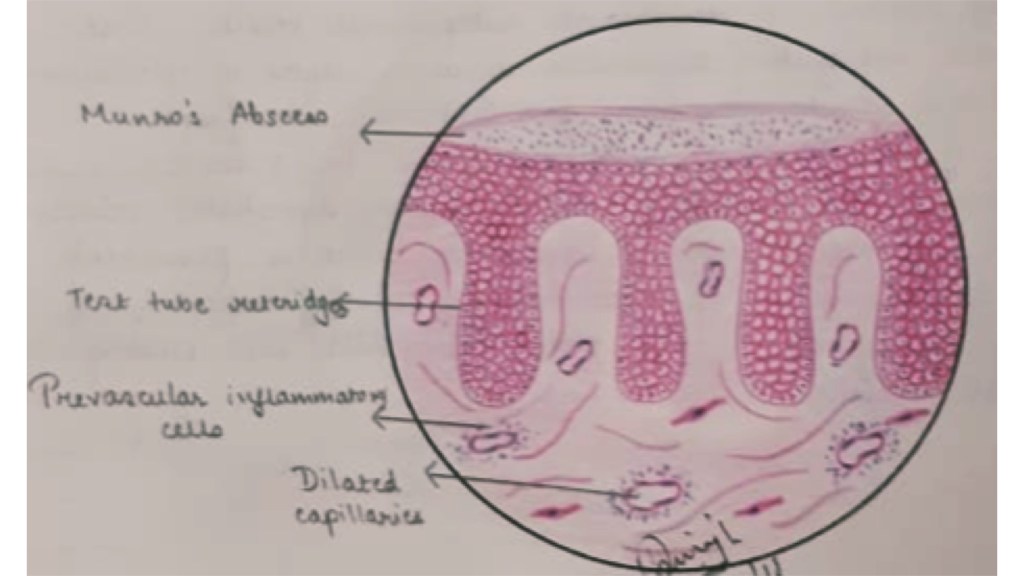
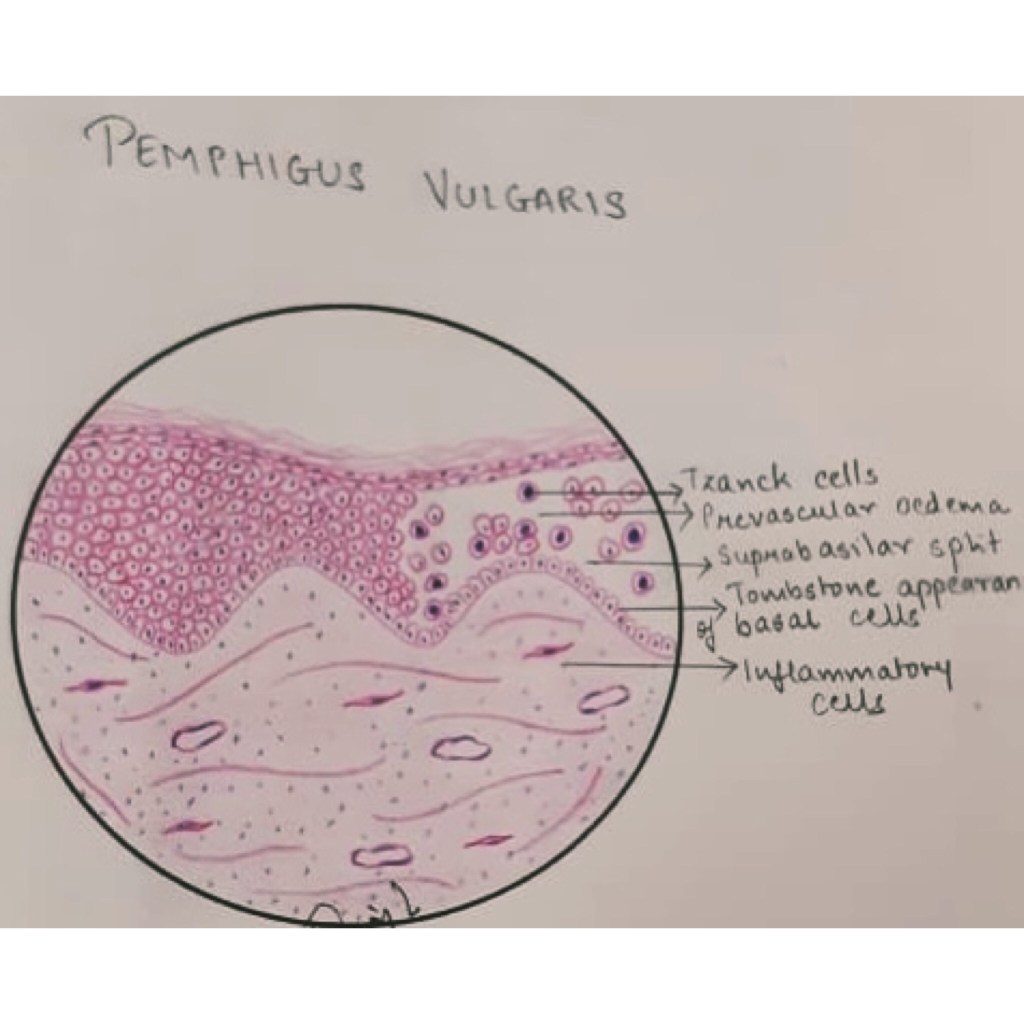
Histopathology:
Intraepithelial cleft – Suprabasilar split
Loss of intercellular bridges leads to acantholysis ➡️ Presence of clumps of epithelial cells seen within vesicular space – Tzank cells
Tzank cells: Swelling of nuclei, hyperchromatic staining & increased RNA in cytoplasm of these cells.
The fluid within vesicles contain PMN leukocytes & lymphocytes.
Scarcity of infammatory cell infiltrate seen in Pemphigus.
Note:
▪️In intraepidermal blister (as in pemphigus) the basal layer remains attached to the basement membrane-Acantholysis
▪️ In subepidermal blister (as in pemphigoid) the entire epidermis is seperated from underlying dermis.
Evaluation:
While the majority of pemphigus cases are diagnosed clinically, a skin biopsy and serum analysis can also confirm the disease.
A skin biopsy can be analyzed by light microscopy showing the separation of keratinocytes above the basal cell layer. Anti-desmoglein 1 and 3 autoantibodies can be evaluated using the indirect immunofluorescent staining or ELISA.
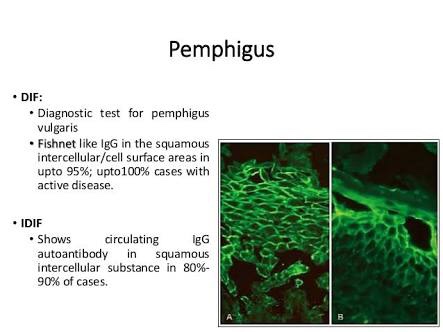
Immunofluorescent testing:
➡️ Direct(DIF) : Biopsy specimen (either frozen section or fixed in Michel Solution) is incubated with fluorescein-conjugated antiglobulin.
➡️ Indirect(IDIF)
Note: In case of auto-immune blistering diseasesbiopsy should be perilesional (b/w 0.5-1cm away from adjacent blister). Fixation not in formalin as it causes autofluorescence – nonspecific positivity.
Management:
The mainstay of treatment involves the cessation of the causal agent and the use of immunosuppressants or immunomodulators to turn off the host autoimmune response.
The main aim of treatment is to heal the blisters and prevent new ones forming. Steroid medication (corticosteroids) plus another immunosuppressant medication such as azathioprine are usually recommended.
Differential Diagnosis:
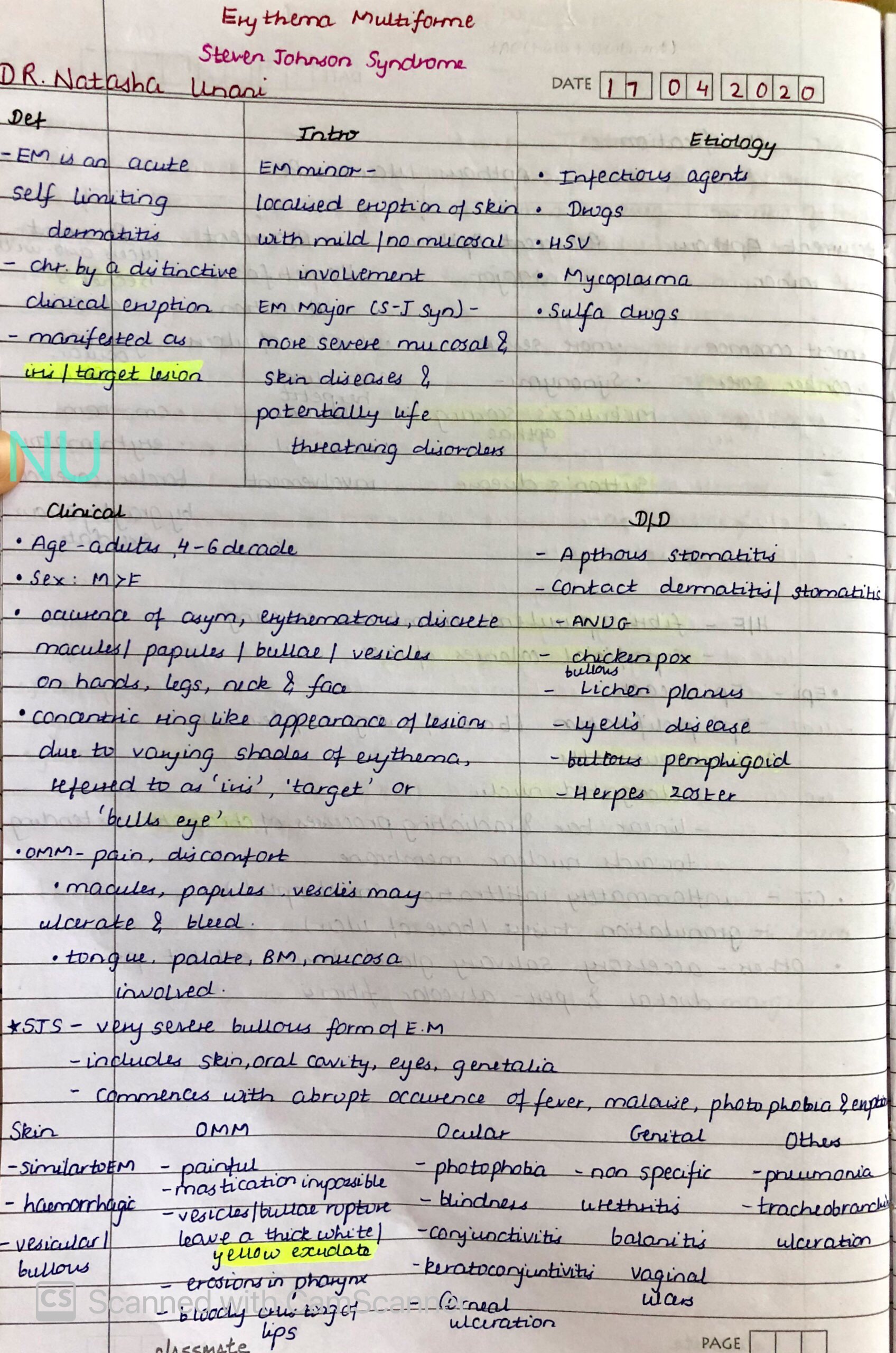
Erythema multiforme
Bullous Lichen planus
Pemphigoid
Dermatitis herpetiformis
Epidermolysis bullosa
References: Shafer’sTextbook Of Oral Pathology; Internet
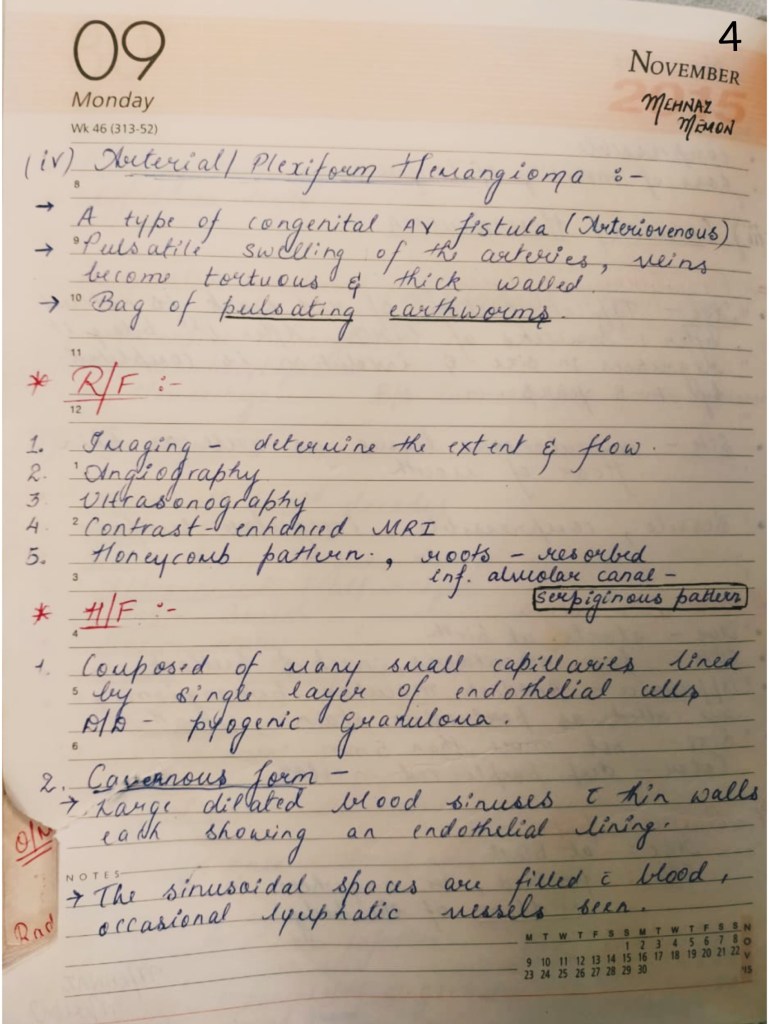
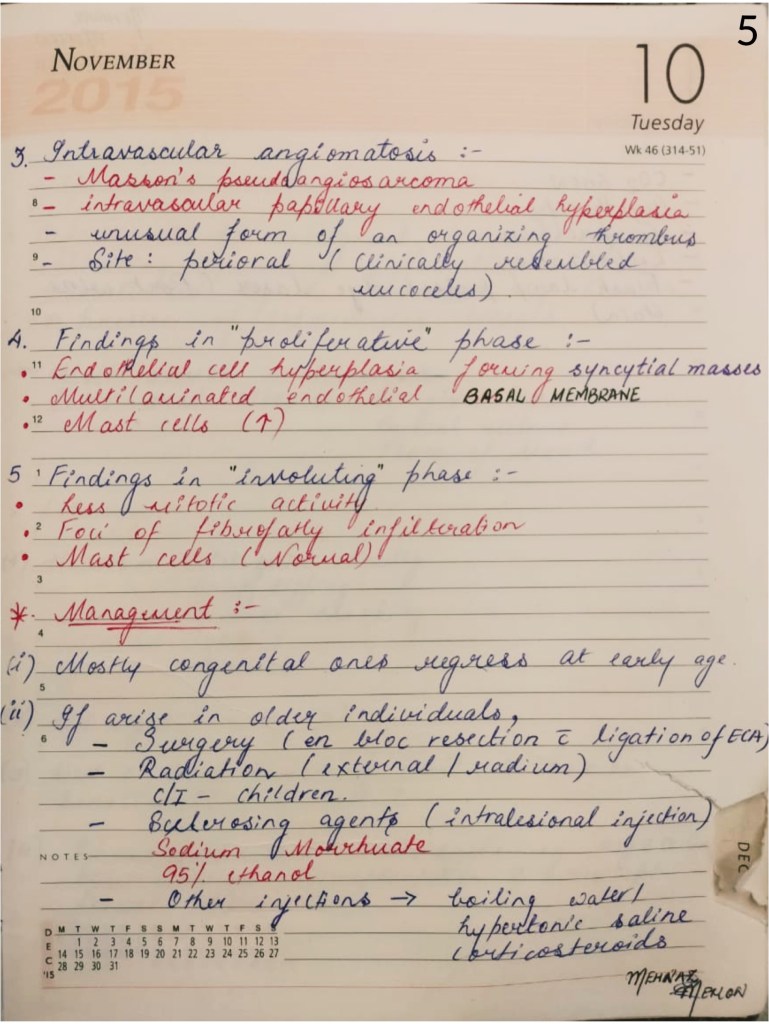
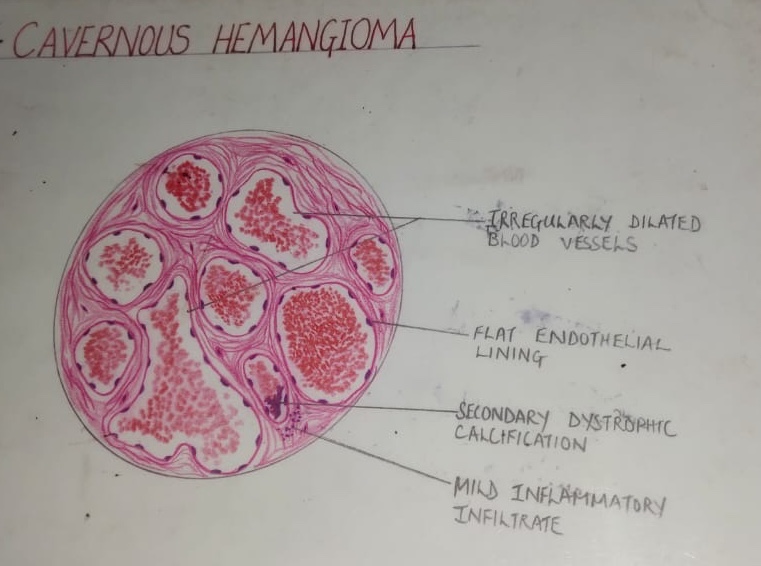
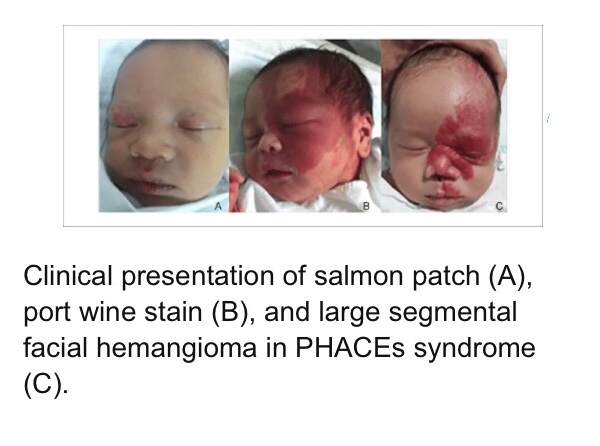
Introduction & Types of Hemangiomas👆🏻Types of Hemangioma continued..👆🏻Types of Hemangioma continued..👆🏻Types, Radiographic Features & Histologic Features of Hemangioma👆🏻 Histologic Features continued.. Management of Hemangioma👆🏻Management continued…👆🏻Histology diagram👆🏻Histology diagram👆🏻
References: Shafer’sTextbook Of Oral Pathology; Image source: Google