


Source- textbook of oral pathology Shafers and Google images
Source- textbook of oral pathology Shafers and Google images
LIP PRINTS
The wrinkles and grooves visible on the lips have been named by Tsuchihashi as ‘sulci labiorum rubrorum’. The imprint produced by these grooves is termed as ‘lip print’, the examination of which is referred to as ‘cheiloscopy’.
Tsuchihashi proposed a classification dividing the pattern of grooves into six types:
Type I: Clear-cut vertical grooves that run across the entire lip
Type I’: Similar to type I, but do not cover the entire lip Type II: Branched grooves
Type III: Intersected grooves
Type IV: Reticular grooves
Type V: Grooves that cannot be morphologically differentiated.

DISADVANTAGE
REFERENCE-SHAFER’S TEXTBOOK OF ORAL PATHOLOGY 8TH EDITION
Forensic Odontology defined by the Federation Dentaire International (FDI) as ‘that branch of dentistry which, in the interest of justice, deals with the proper handling and examination of dental evidence, and with the proper evaluation and presentation of dental findings’.
Scope of Forensic Odontology
• Record preparation—the correct handling and exami- nation and the proper preparation and presentation of dental evidence in both civil and criminal legal procedures.
• Identification—personal identification, either individually or in context of mass disasters.
• Age assessment—to calculate the age of patient.
• Bite mark investigation—investigation of criminal cases where bite marks are involved and the interpretation of
• Humanabuse—recognitionofdomestic,andchildabuse.
• Lipprint—comparisonandidentificationoflipprint.
• Legalaspect—legalaspectofdentaltraumatology.
A vital role the forensic dentist plays is in criminal investigation.
BITE MARKS
McDonald (1974) has defined bitemark as “a mark caused by the teeth either alone or in combination with other mouth parts”.

Bite marks may be caused by humans or animals; they may be on tissue, food items, or other objects.
CLASSIFICATION OF BITE MARKS
Cameron and Sims classification
a. Human : Children, Adults
b. Animals : Mammals, Reptiles, Fish
c. Mechanical : Full denture, belt marks etc
a. Skin : Human, Animal
b. Perishable items : Food items like cheese, apple etc.
c. Non- perishable items : Unanimated objects such as pipes, pens, pencils.
WEBSTER’S CLASSIFICATION
Type I – food item fractures readily with limited depth of tooth penetration e.g. hard chocolate.
Type II – food item fractures with considerable penetration of teeth e.g. bite marks in apple & firm fruits.
Type III – Complete or near complete penetration of the food item with slide marks e.g cheese

FACTORS AFFECTING BITE MARK INJURIES
CHARACTERISITCS OF HUMAN BITE MARK FOR IDENTIFICATION
BITE MARK INVESTIGATION
1. Description of the bite marks
2. Collection of evidence from victim
3. Collection of evidence from suspect

REFERENCE- SHAFER’S TEXTBOOK OF ORAL PATHOLOGY AND SLIDE SHARE

Source Borley Textbook
Reiter’s syndrome is associated with urethritis, balanitis, conjunctivitis, and mucocutaneous lesions.
It is a disease of unknown aetiology, although there is evidence of an infec- tious origin.
It is one of the most common complications of non-specific urethritis and it clinically mimicks gonorrhoea, although the urethral discharge is negative for Neisseria.

CLINICAL FEATURES
>Reiter’s syndrome is more prevalent in young adult men, usually between 20 and 30 years of age.
>The male-to-female ratio is 9:1.
>There is a typical tetrad of manifestations: non- gonococcal urethritis, arthritis, conjunctivitis, and mucocutaneous lesions.
>Urethritis may be the first sign. The urethral discharge is usually associated with itching and burning sensation.
>The arthritis is often bilaterally symmetrical and usually polyarticular.
>Conjunctivitis is often so mild as to be overlooked.
>The skin lesions are similar to those seen in keratoderma blennorrhagica and consist of red or yellow keratotic macules or papules which eventually desquamate.
Oral Manifestations
Sites—it is seen on the buccal mucosa, lips and gingiva.
Oral lesions appear as painless, red, slightly elevated areas, some- times granular or even vesicular, with a white circinate border on the buccal mucosa, lips, and gingiva.
The palatal lesions appear as small, bright red purpuric spots, which darken and coalesce, while the lesions on the tongue closely resemble ‘geographic’ tongue.

Laboratory Findings
The patients usually have a mild leukocytosis, an elevated erythrocyte sedimentation rate, and pyuria.

REFERENCE- SHAFER’S TEXTBOOK OF ORAL PATHOLOGY [8TH ED} AND ANIL GHOM TEXTBOOK OF ORAL MEDICINE
Wegener’s granulomatosis is a disease of unknown aetiology, which basically involves the vascular, renal and respiratory systems. It involves the nose, paranasal air sinuses, lower respiratory tract, gut, joints, nervous system, and kidneys. Involvement of the kidney is the common cause of death.
This disease is caused by an abnormal immune reaction secondary to a nonspecific infection or a hypersensitivity reaction to an unknown antigen.

Clinical Features
>Wegener’s granulomatosis may occur at any age, although the majority of cases are in the fourth and fifth decadesof life.
>There is a slight predilection for occurrence in males.
>It is best described as a multisystem disease, which is usually first characterized clinically by the development of rhinitis, sinusitis, and otitis or ocular symptoms.
>The patient soon develops a cough and hemoptysis as well as fever and joint pain.
>Hemorrhagic or vesicular skin lesions are also commonly present.
>Granulomatous lesions of the lungs are found on the chest radiograph, while the glomerulonephritis, which develops ultimately, leads to uraemia and terminal renal failure.
>In nervous system, sensory neuropathy may be an occasional finding.
>Prognosis—the disease is usually fatal, with mean survival time of 5 months. Death occurs due to involvement of kidney.
Oral Manifestations
Involvement of the gingiva has been the most common and characteristic manifestation, and is termed as strawberry gingivitis.Gingival lesions may manifest as ulcerations, friable granular lesions, or simply enlargements of the gingiva.
The inflammatory process starts in the interdental papilla and spreads rapidly to the periodontal structure and leads to bone loss and tooth mobility.
Palate—orallesionstypicallyincludeulcerationofthe palate by extension of nose lesions and destruction of nasal septum. This will lead to perforation of palate.
• Teeth—theremaybelooseningofteethwithinsomecases spontaneous exfoliation. After extraction of teeth patient is usually noticed poor healing.

Laboratory Findings
Laboratory findings include anaemia, leukocytosis, elevated erythrocyte sedimentation rate, and hyperglobulinaemia. Because of kidney involvement, haematuria is common, as well as the finding of albumin, casts, and leukocytes in the urine. Circulating immune complexes have been demonstrated in some patients, but this is not a consistent finding.
Histologic Findings
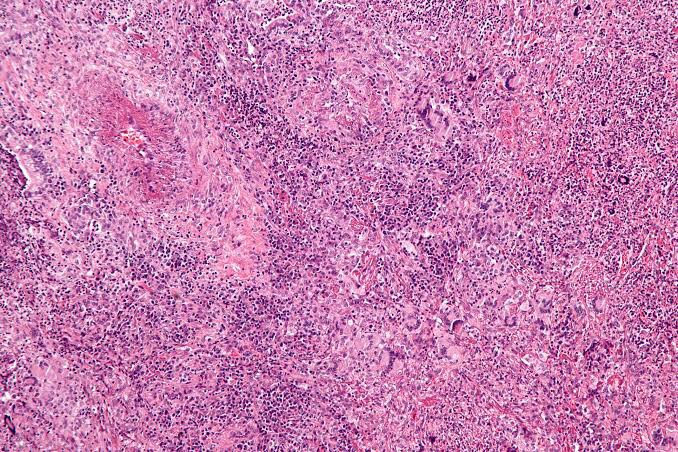
Wegener’s granulomatosis presents a pattern of mixed inflammation centred around the blood vessels.
The lesions in the upper respiratory tract and lungs consist of giant cell necrotizing granulomatous lesions showing vasculitis.
Oral biopsy specimens show pseudoepitheliomatous hyperplasia and subepithelial abscesses. The gingival and other lesions show a nonspecific granulomatous process with scattered giant cells.
Diagnosis
REFERENCE- SHAFER’S TEXTBOOK OF ORAL PATHOLOGY {8TH ED} AND ANIL GHOM TEXTBOOK OF ORAL MEDICINE
1. Recurring oral ulcers,
2.Recurring genital ulcers, and
3.Eye involvement.
ETIOLOGY
CLINICAL MANIFESTATIONS
ORAL MANIFESTATIONS
Histologic Features
The microscopic findings are not diagnostic. They consist of parakeratosis, acanthosis, and polymorphonuclear leukocyte infiltration of epithelium, sometimes with mi- croabscess formation similar to psoriasis. The connective tissue shows a lymphocyte and plasma cell infiltrate.
Laboratory Findings
The patients usually have a mild leukocytosis, an elevated erythrocyte sedimentation rate, and pyuria.
DIFFERENTIAL DIAGNOSIS
TREATMENT
The management of Behçet’s syndrome depends on the severity and the sites of involvement.
REFERENCE- BURKET TEXTBOOK OF ORAL MEDICINE AND SHAFER’S TEXTBOOK OF ORAL PATHOLOGY {8TH EDITION}
Diagnosis
• Clinical diagnosis—skin lesion with lesion present on oral mucosa which is atrophic and erythematous will suspect lupus erythematous. Oral and nasopharyngeal ulceration is major diagnostic criteria for SLE.
Laboratory diagnosis—L.E. cell inclusion phenomenon with surrounding pale nuclear mass apparently devoid of lymphocytes. Anemia, leukopenia and thrombocyto- penia, with sedimentation rate increased. Serum gamma globulin increased and Coomb’s test is positive.
Positive lupus band test—it shows deposition of IgG,IgM or complement component in skin.
REFERENCE- ANIL GHOM TEXTBOOK OF ORAL MEDICINE; BURKIT TEXTBOOK OF ORAL MEDICINE AND GOOGLE[SLIDE SHARE]

Zone I: Zone of fatty degeneration of odontoblast process
Zone 2: Zone of dentinal sclerosis characterized by deposition of cal- cium salts in dentinal tubules
Zone 3: Zone of decalcification of dentin, a narrow zone, preceding bacterial invasion
Zone 4: Zone of bacterial invasion of decalcified but intact dentin Zone 5: Zone of decomposed dentin
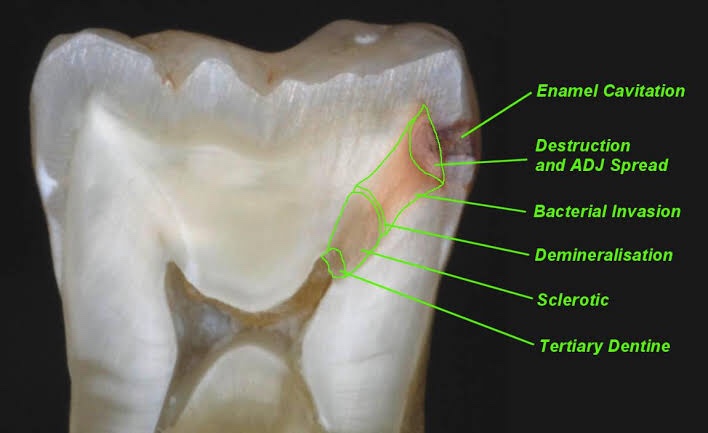
Early dentinal caries
Fatty degeneration of odontob/ast process
>Disposition of fat globules – precedes early sclerotic changes >Special stains – Sudan red
>Significance-
1.Fat contributes to impermeability
2.Predisposing factor for dental sclerosis
Sclerotic dentin
>Reaction of vital pulp – calcification of dentinal tubules (DT)
>Seals off DT from further penetration of microorganisms
>Minimal in rapidly advancing caries
>Prominent in slow caries
>Sclerotic dentin – appear white in transmitted light
Decalcification of dentinal tubules
>Above dentinal sclerosis – zone of decalcification
>Occurs in advance of bacterial invasion of DT
>Pioneer bacteria
>The initial decalcification – only the walls of DT
>Study of tubules- pure form of microorganisms
Zone of microbial invasion
>Proteolytic organisms – predominantly in deeper layers Acidogenic microorganisms – more in early caries
>Supporting the hypothesis that initiation and progression are two distinct processes and must be differentiated
Advanced dentinal caries
>Decalcification of the walls of DT – confluence
>Thickening of sheath of Neumann – along its course • Increase in the diameter of DT – microorganisms
>Focal coalescence of adjacent tubules and ovoid area of destruction- liquefaction foci
>Acidogenic organisms – initial decalcification
>Proteolytic organisms – matrix destruction
>Multiple areas of destruction>Necrotic mass of dentin (leathery consistency)
>Formation of transverse cleftsExtend at right angles to DT and parallel contour line
>Peeling away of carious dentin
REFERENCE- Shafers textbook of oral pathology 8th edition
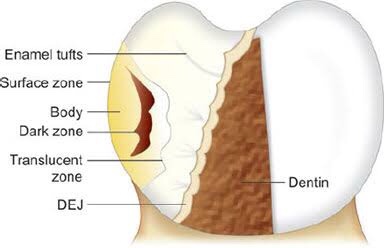
Four zones are clearly distinguishable, starting from the inner advancing front of the lesion. These are the (1) translucent zone, (2) dark zone, (3) body of the lesion and (4) surface layer.

Zones of enamel caries Translucent zone {TZ)
First recognizable zone of alteration
Advancing front of the lesion
Half the lesions demonstrate TZ, not always present
Seen in longitudinal ground sections in clearing (quinoline – RI – 1.62)
TZ appears structureless
Pore volume – I% (compared to 0.1 % of sound enamel)
Dark zone
Lies adjacent and superficial to the translucent zone Positive zone
Shows positive birefringence (in contrast to sound enamel.
Pore volume of 2-4% (polarized light)
Presence of small pores; large molecules of quinoline are unable to penetrate
Micropore system – gets filled with air and becomes dark
Medium like water may penetrate
Body of the lesion
Between unaffected, surface and dark zone
Area of greatest demineralization
Pore volume – 5% in periphery and 25% in centre
Quinoline imbibition – body appears transparent
Water imbibition – positive birefringence compared to sound enamel Striae of Retzius – prominent
Surface zone
Quantitative studies – partial demineralization of 1-10% • Pore volume – less than 5% of the spaces
Negative birefringence – water imbibition
Positive birefringence – porous subsurface
All the four zones of enamel caries cannot be seen with same immersion medium.
REFERENCE – Shafers textbook of oral pathology 8th edition





