source – don’t remember, had written it a lot time ago
Category: Oral And Maxillofacial Surgery
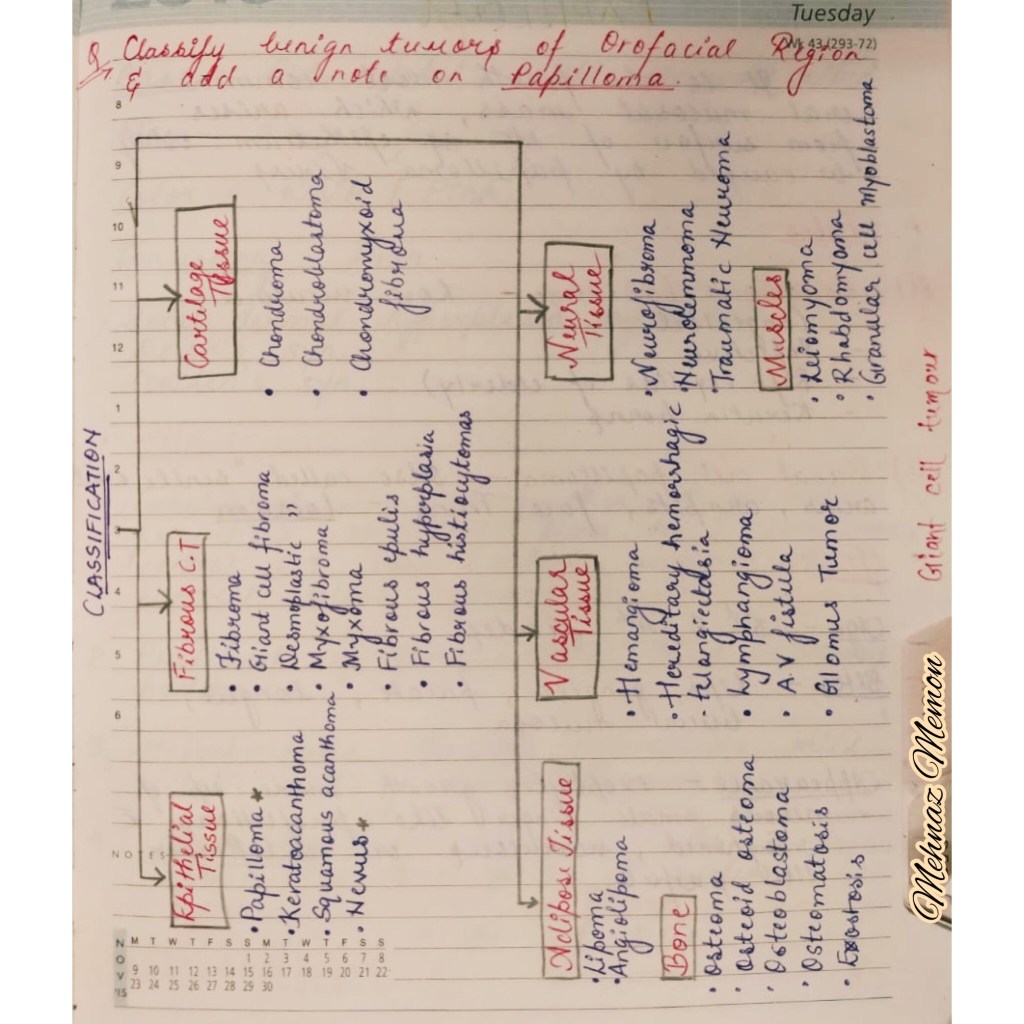
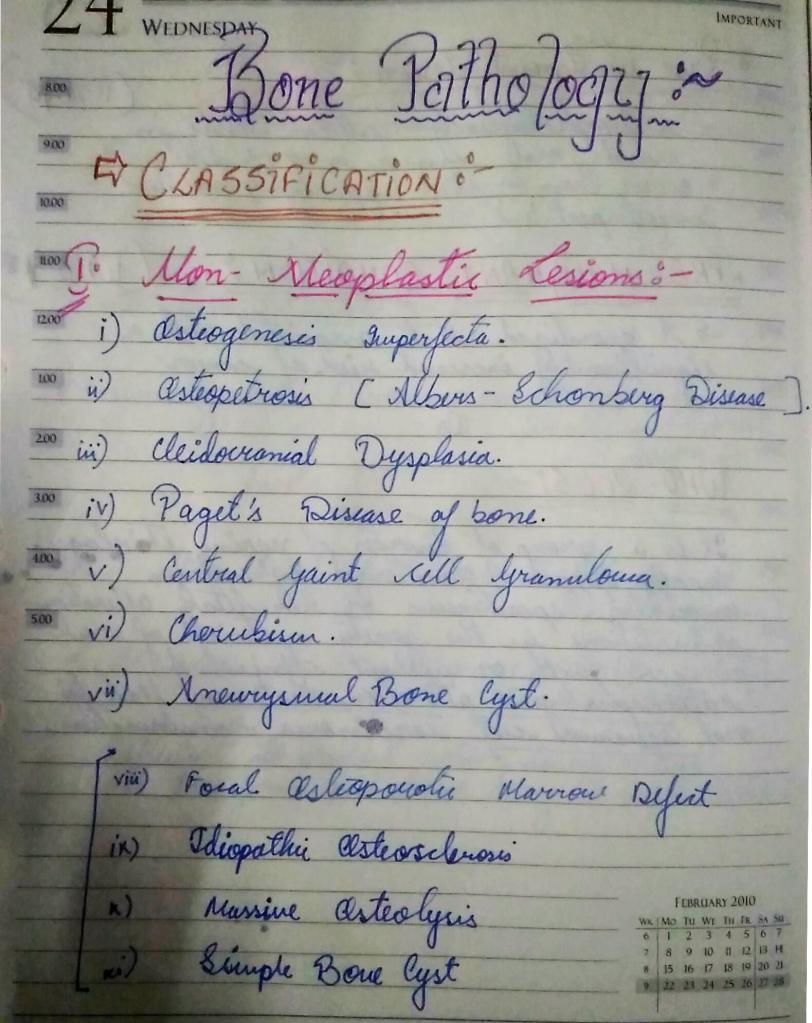
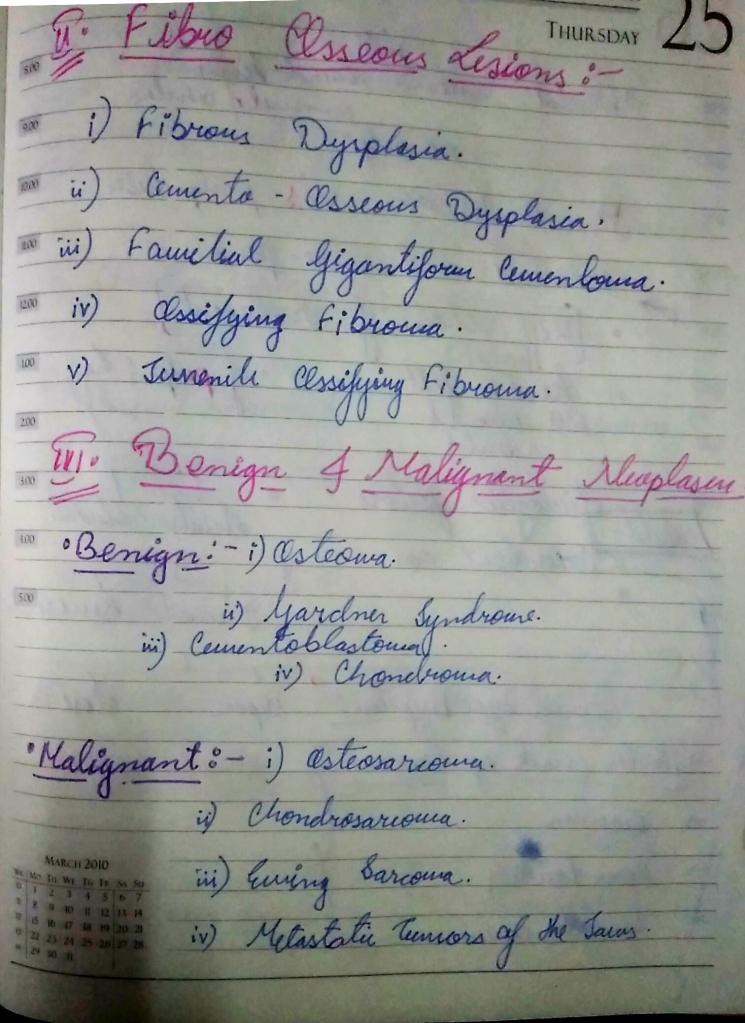
BONE PATHOLOGY
Classification of Bone pathology:-
Regards:-
Kriti Naja Jain 🙂
Reference :-
Neville oral and maxillofacial pathology 3rd e
LARYNGEAL MASK AIRWAY

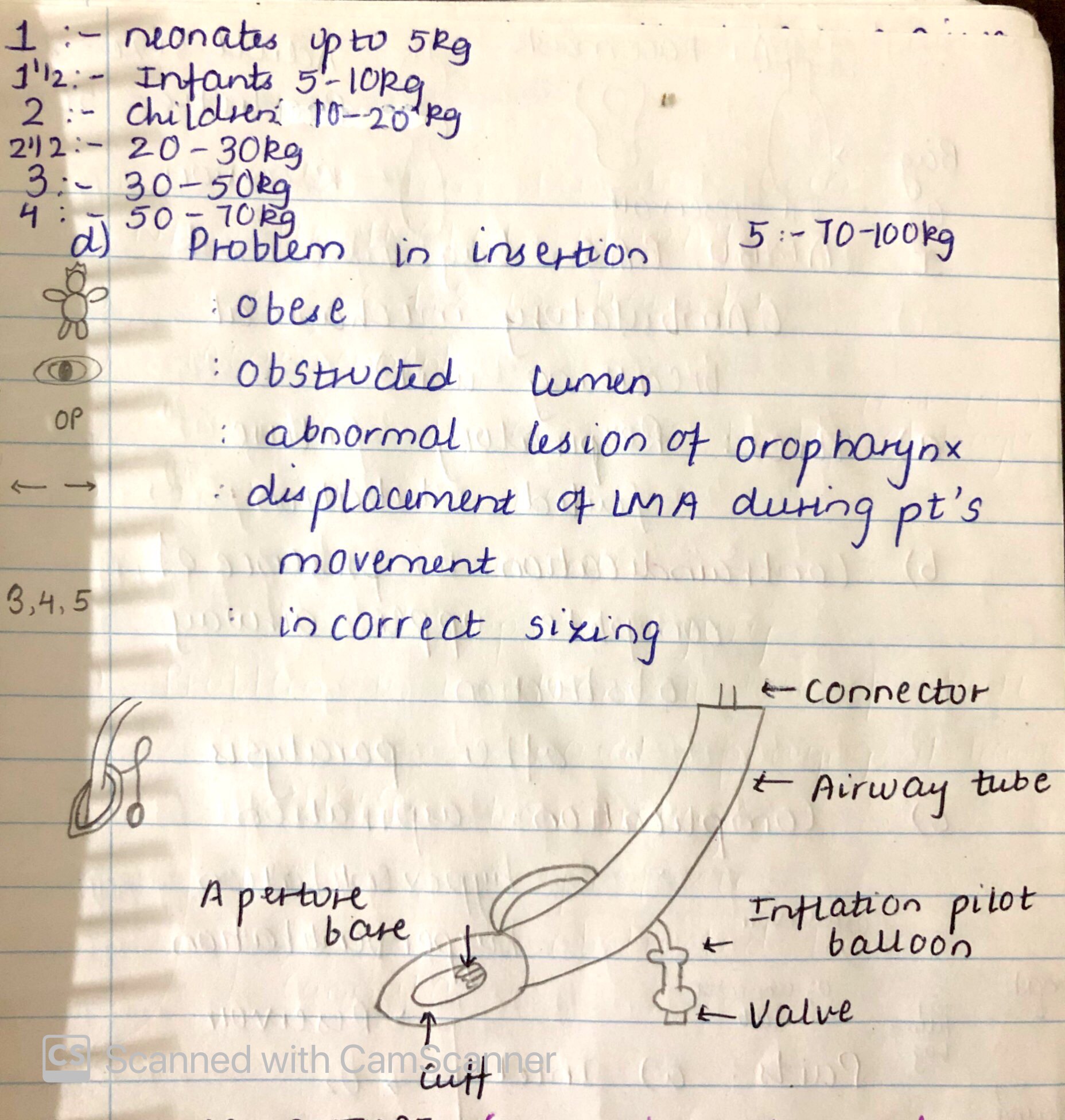
SOURCE – NANCY 13th EDITION
DEVELOPMENTAL DISORDERS OF TMJ

🔹 Classification:-
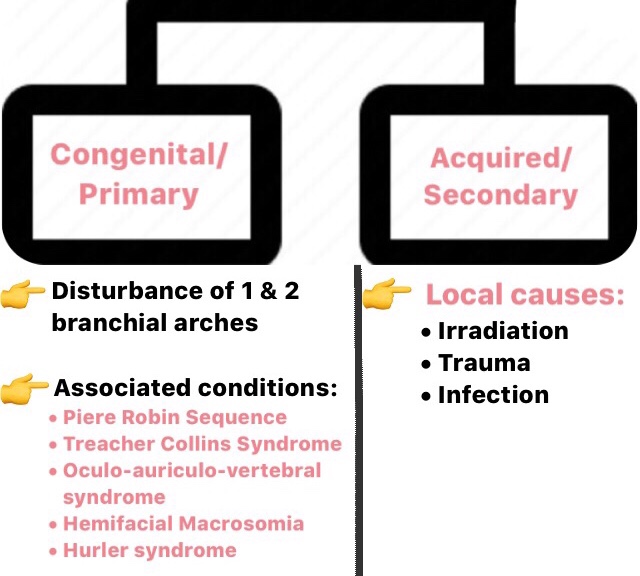
1) Condylar Hypoplasia/Aplasia –
Clinical Features
1) Unilateral involvement (most common)
- Defective/absent external ear
- Underdeveloped ramus
- Facial asymmetry
- Altered occlusion & mastication
- Lack of downward & forward growth of the body of mandible
- Thickening of bone- Angle of mandible
- Shift of mandible towards the affected side.
2) Bilateral involvement:
- Micrognathia
- Dental crowding
- Open bite
Severe Cases
- Airway obstruction
- Posterior displacement of tongue
- Feeding and speech error
Treatment
- Cartilage/Bone transplants – Osteotomy
- Tracheostomy – Airway obstruction
- Severe cases – Osteoplasty
2) Condylar Hyperplasia:-
➡️ Enlargement due to chronic inflammation.
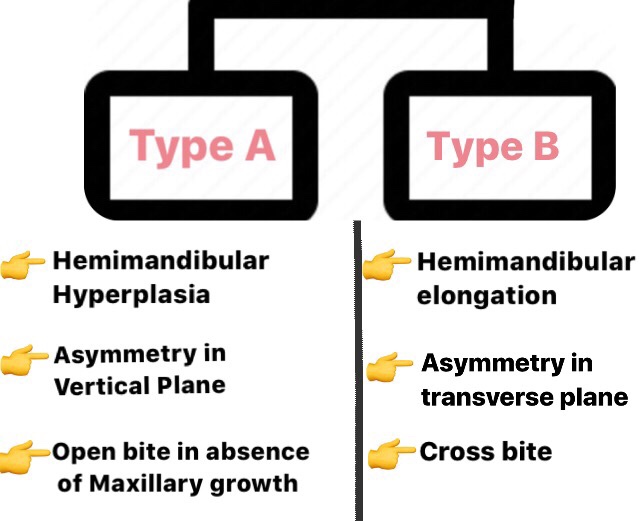
CATEGORIES
Clinical Features
- Age – 3rd decades; Sex – Females
- Elongation of face
- Deviation of chin away from the affected side.
- O/M: Malocclusion
Treatment
- Condylectomy
- Orthodontics
- Orthognathic Surgery
3) Bifid Condyle:-
➡️ A deep groove/depression around midline of condylar head due to lack of blood supply or trauma. Asymptomatic in nature.
Dr. Mehnaz Memon🖊
References: Shafers Textbook Of Oral Pathology 7Ed, Image Source: Google
OSSEOUS DEFECTS

source – do not remember had written it long back
Nausea and Vomitting
Nausea ,vomitting are common go to side effects of a drug, when external examiner asks during viva of a medical student. But, these symptoms can reveal many underlying conditions and diseases apart from the side effects of many drugs.
Nausea is imminent desire to vomit and often precedes or accompanies vomitting. vomiting is the forceful expulsion of the gastric contents through mouth.
PATHOPHYSIOLOGY:
1. Activation of the CTZ ,sends the impulses to the vomiting centre in brainstem,
2. Gastric fundus and gastroesophageal sphincter relaxes inturn cause raise in intra-abdominal pressure increase,due to increase in abdominal and diaphragm muscle contraction causes the gastric contents to enter the oesophagus ,
3. Increased intra-thoracic pressure results in further movement of food material to mouth
4.Reflex elevation of the soft palate and closure of glottis protect the nasopharynx and trachea and completes the vomiting
Causes of vomiting:
1. DRUGS:
-Cancer chemotherapy
-Antibiotics
-Cardiac antiarrhythmics
-Digoxin
-Oral hypoglycemics
-Oral contraceptives
2.Metabolic and endocrine causes:
-Pregnancy
-Uremia
-Ketoacidosis
-Thyroid and parathyroid disease.
-Adrenal insufficiency
3.Toxins:
-Liver failure
-Ethanol
4.Labyrinthine disease
- Motion sickness
- Labyrinthitis
- Malignancy
5. Bowel obstructing disorder
6. Cardiopulmonary disorders and cardiomyopathies
7.Enteric infections
-viral
-Bacterial
8.Inflammatory dieases.
- cholecystitis.
-Pancreatitis
-Appendicitis
-Hepatitis.
9.Intracerebral disorders
-Intracerebral disorders
-Malignancy
-Abscess
-Hydrocephalus
10. Post operative vomiting
11.Impaired motor functions.
Careful clinical examination, will reveal the underlying cause for nausea and vomiting, like ,vomiting that occurs predominantly in the morning is often seen in pregnancy, uremia, and alcoholic gastritis;projectile vomiting suggests increased intracranial pressure,vomiting during or shortly after a meal may be due to psychogenic causes or peptic ulcer disease.
complications, can be Rupture of the esophagus,hematemesis from a mucosal tear,dehydration, malnutrition, dental caries and erosions, metabolic alkalosis, hypokalemia, and aspiration pneumonitis.
Treatment is mainly based on the treatment of the underlying cause,
-Antihistamines such as meclizine and dimenhydrinate are effective
for nausea due to inner ear dysfunction
-Anticholinergics such as scopolamine are effective for nausea
associated with motion sickness
-Haloperidol and phenothiazine derivatives such as
prochlorperazine are often effective in controlling mild nausea
and vomiting, but sedation, hypotension, and parkinsonian
symptoms are common side effects.
-Metoclopramide may be superior to the phenothiazines in treating
severe nausea and vomiting.IV metoclopramide may be effective
as prophylaxis against nausea when given before chemotherapy.
-Ondansetron and granisetron, serotonin receptor blockers,
and glucocorticoids are used for treating nausea and vomiting
associated with cancer chemotherapy.
-Aprepitant, a neurokinin receptor blocker, is effective at
controlling nausea from highly emetic drugs like cisplatin
DISLOCATION OF CONDYLES/LUXATION OF TMJ

Let’s first understand the terms Luxation, Subluxation & Habitual Dislocation👇🏻
- Luxation of joint refers to complete dislocation – Non self reducing.
- Subluxation is partial dislocation or Self-reducing.
- Repeated anterior dislocation & self reduction leads to Habitual/Recurrent dislocation.
➡️ Condylar dislocations can be divided into Anterior (Luxation/Subluxation), Cranial & Posterior Dislocations.
Etiology:
- Fracture of condyle (due to acute trauma)
- Stretching of capsule of TMJ
- Yawning/mouth opened too widely (during extraction/ Tonsillectomy/ Endoscopy)
Clinical Features:
- Sudden locking & immobilization of jaw when the mouth is open. Hence mouth cannot be closed and patient becomes panicky.
- Spasmodic contractions of Temporal, internal pterygoid & masseter muscle with protrusion of jaw.
- Severe pain, excessive salivation & depression of skin around preauricular area
- Eating/talking – impossible.
Treatment:
- Relaxation of Muscles – Inferior & superior pressure of thumbs in mandibular molar area.
- General anesthesia
- Tiring the masticatory muscles: Cupping the chin in palm of hand & applying pressure 5-10 min.
- Recurrent Dislocation – Alter the ligament, bony musculature.
- Repositioning Dislocated Temperomandibular Joint..Do watch till the end! (Video credits: Youtube channel-The General Medicine)👇🏻
https://www.instagram.com/tv/Bz-qZqunJtF/?igshid=24valy01dqya
Read More »
GRADINNG & STAGING OF SQUAMOUS CELL CARCINOMA

Squamous Cell Carcinoma (Epidermoid Carcinoma)
- SCC is defined as ‘a malignant epithelial neoplasm exhibiting squamous differentiation as characterized by the formation of keratin and/ or the presence of intercellular bridges‘.
- The epidermoid carcinoma is the most common malignant neoplasm of the oral cavity.
- The male-female ratio is approximately 2:1 for oral carcinoma, except for carcinoma of the vermilion border of the lower lip
ETIOLOGY:-
- The cause of oral squamous cell carcinoma is multifactorial.
- No single causative agent or factor (carcinogen) has been clearly defi ned or accepted, but both extrinsic and intrinsic factors may work .
- FACTORS:-
- TOBACCO SMOKING
- SMOKELESS TOBACCO
- BETEL QUID (PAAN)
- ALCOHOL
- PHENOLIC AGENTS
- RADIATION
- IRON DEFICIENCY
- VITAMIN-A DEFICIENCY
- SYPHILIS
- CANDIDAL INFECTION
- ONCOGENIC VIRUSES
- IMMUNOSUPPRESSION
- ONCOGENES AND TUMOR SUPPRESSOR GENES
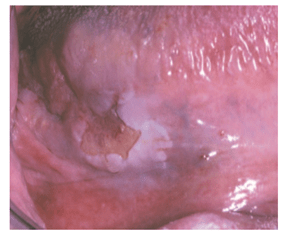
- CLINICAL FEATURES:-
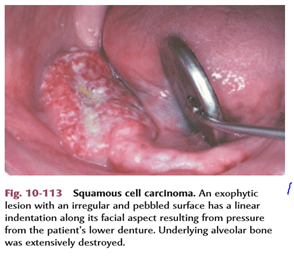

- Oral squamous cell carcinoma has a varied clinical presentation, including the following:
● Exophytic (mass forming; fungating, papillary, verruciform)
● Endophytic (invasive, burrowing, ulcerated)
● Leukoplakic (white patch)
● Erythroplakic (red patch)
● Erythroleukoplakic (combined red-and-white patch)

- STAGING :-
Tumor size and the extent of metastatic spread of oral squamous cell carcinoma are the best indicators of the patient’s prognosis. Quantifying these clinical parameters is called staging the disease.
The most popular staging protocol, the tumor-node-metastasis (TNM) system.
This staging protocol depends on three basic clinical features:
1. T—Size of the primary tumor, in centimeters
2. N—Involvement of local lymph nodes
3. M—Distant metastasis
The American Joint Committee on Cancer (AJCC) designated staging by TNM Classification was used.
TNM clinical classification:-


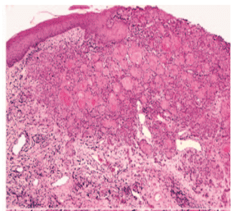
- HISTOPATHOLOGIC FEATUR:-
- Squamous cell carcinoma arises from dysplastic surface epithelium.
Features are:-
- sheets or islands of cells or cords
- a strong infl ammatory or immune cell response
- focal areas of necrosis
- invading into underlying muscles, bonesor adipose tissues
- angiogenesis
- desmoplasia or scirrhous change
- abundant eosinophilic cytoplasm with large, often darkly staining (hyperchromatic) nuclei
- increased nuclearto-cytoplasmic ratio.
- nuclear pleomorphism
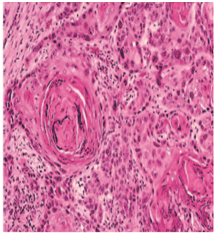
- keratin pearls (a round focus of concentrically layered keratinized cells)
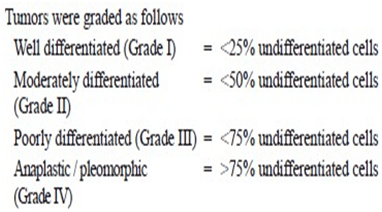
- GRADING:-
- Histopathologic evaluation of the degree to which these tumors resemble their parent tissue (squamous epithelium) and produce their normal product (keratin) is called grading.
- The one advantage of grading a tumour is that the grade reflects the anaplasticity of the lesion, which in turn indicates the general rapidity of growth, the rapidity of metastatic spread, the general reaction to be expected after X-ray radiation and the prognosis.
- There are 4 classifications used to describe grading systems :-
- 1-BRODERS CLASSIFICATION:-
- Broders’ system (1920) was first established on the basis of the proportion of highly differentiated cells in the tumour. Broders’ system was simple and widely used, it was a poor predictor for survival or me- tastasis.
* a system of grading tumours in which a grade 1 lesion was highly differentiated (its cells were producing much keratin), while grade 4 was very poorly differentiated (the cells were highly anaplastic and showed no keratin formation).
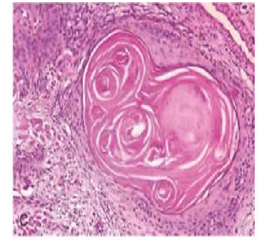
I-WELL DIFFERENTIATED:
-consists of sheets and nests of cells
-cells are generally large
– intercellular bridges or tonofibrils are not demonstrated.
-The nuclei are large and demonstrate variability in the intensity of the staining reaction.
-Nuclei that stain heavily with hematoxylin are referred to as hyperchromatic.
-mitotic figures may be found(Many of these mitotic figures are atypical.)
-the most prominent features of the welldifferentiated epidermoid carcinoma is the presence of individual cell keratinization-the formation of numerous epithelial or keratin pearls of varying size.
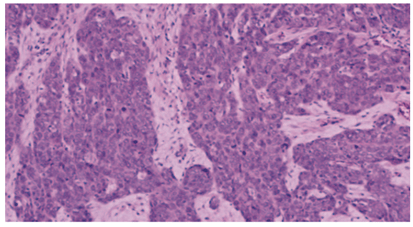
II– ModeratelyDifferentiated epidermoid carcinomas:
– lose certain features so that their resemblance to squamous epithelium is less pronounced
-The characteristic shape of the cells and their arrangement may be altered.
– The growth rate of individual cells is more rapid,
– the greater number of mitotic figures,
– even greater variation in sizes, shape and tinctorial reaction,the failure to carry out the function of a differentiated squa- mous cell, the formation of keratin.
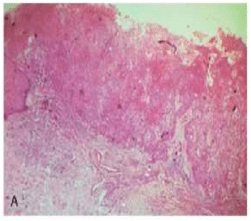
III-POORLY DIFFERENTIATED TYPE:
-bear little resemblance to their cell of origin
-will often present diagnostic difficulties because of the primitive and uncharacteristic histological appearance of malignant,
-rapidly dividing cells
– cells show an even greater lack of cohesiveness and are extremely vagarious.

2.JAKOBSS0N’s GRADING SYSTEM:-
-In 1973, Jakobsson et al developed a multifactorial
grading system which had the advantage of scoring tumour-host interactions and tumour characteristics, but eventually proved to be useful only when applied to tongue cancers.
-Parameters used in Jakobsson’s method are:-
i- KRE- keratinization
ii-NP- nuclear pleomorphism
iii-MIT-mitosis
iv-POI- pattern of invasion
v-LPR- lympho-plasmocyticrspon
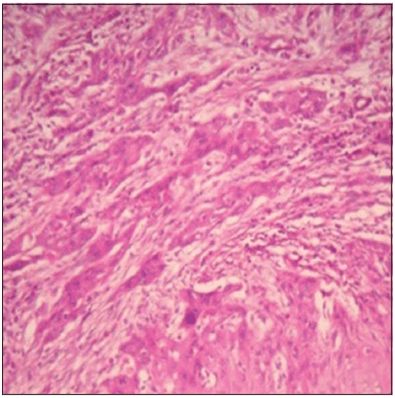
Tumor cells invading in strands and cords
-Similar findings were observed in Anneroth and Hansen’s grading where the criteria were similar except that the parameter vascular invasion (VI) was omitted.
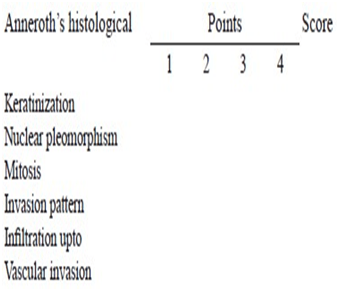
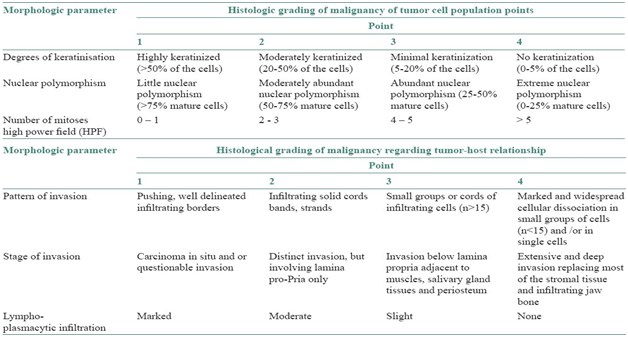
3-Anneroth’s classification:
- This system is constituted by six histological variables of equal value in the determination of the grade of malignancy, three connected with the tumor cellular population (differentiation and proliferation mitosis) and the other three connected with tumor-host relationship (pattern and stage of invasion; and cellular response).
Anneroth’s classification (multifactor grading system)
-According to the classification, three parameters reflecting tumor cell features including keratinization, polymorphism, and mitoses were evaluated in the whole thickness of the tumor and each was scored from 1 to 4. Mode of invasion and inflammatory infiltration representing tumor-host relationship were graded in the most invasive margins and scored from 1 to 4:
-Variables such as:-
i-pattern of invasion,
ii- tumor thickness,
iii-degree of keratinization,
iv-nuclear pleomorphism,
v-lymphocytic response,
vi-mitotic rate
4.BRYNE’S GRADING SYSTEM:-
-Bryne et al (1989) modified Anneroth’ s grading system and developed a malignancy grading focusing on the invasive front of the tumour.
– This method of grading appeared to be less time-consuming in the assessment of the neoplasm.
-Nevertheless, this system is not sufficiently homogeneous to allow grading parameters to be assessed individually
-This was performed at the invasive tumor front (ITF).
-The Bryne’s grading system is more predictive for LNM as compared with the multifactorial grading systems that is, Jakobsson’s and Anneroth and Hansen’s. Broder’s grading system is of no prognostic value.
-Parameters used are:-
i-Keratinisation
ii-nuclear polymorphism
iii-mitosis
iv-pattern of invasion
v-lympho-plasmocytic response
vi-lymph nodes
REFERENCES :
| 1.Comparative study of various grading systems in oral squamous cell carcinoma and their value in predicting lymph node metastasis |
| Saleha Jamadar1, TV Narayan1, Balasundari Shreedhar2, Leeky Mohanty1, Sadhana Shenoy1 1 Department of Oral Pathology and Microbiology, The Oxford Dental College, Hospital and Research Centre, Bommanahalli, Bengaluru, Karnataka, India 2 Department of Oral Pathology and Microbiology, Career Dental College, Lucknow,Uttar Pradesh, India |
2.A study on histological grading of oral squamous cell carcinoma and its co-relationship with regional metastasis
M Akhter, S Hossain, Quazi B Rahman, Motiur R Molla
Department of Oral and Maxillofacial Surgery, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
3.Shafer’s Textbook of Oral Pathology,8e
4.NEVILLE -Oral & Maxillofacial Pathology,3e